Lucía de Jorge-Huerta, José Tiago Silva, Mario Fernández-Ruiz, Isabel Rodríguez-Goncer, M Asunción Pérez-Jacoiste Asín, Tamara Ruiz-Merlo, Carlos Heredia-Mena, Esther González-Monte, Natalia Polanco, Rafael San Juan, Amado Andrés, José María Aguado, Francisco López-Medrano
{"title":"基于个性化护理包的新型干预措施,减少肾移植受者的感染。","authors":"Lucía de Jorge-Huerta, José Tiago Silva, Mario Fernández-Ruiz, Isabel Rodríguez-Goncer, M Asunción Pérez-Jacoiste Asín, Tamara Ruiz-Merlo, Carlos Heredia-Mena, Esther González-Monte, Natalia Polanco, Rafael San Juan, Amado Andrés, José María Aguado, Francisco López-Medrano","doi":"10.1111/tid.14354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infection remains a relevant complication after kidney transplantation (KT). A well-established strategy in modern medicine is the application of bundles of evidence-based practice in clinical settings. The objective of this study is to explore the application of a personalized bundle of measures aimed to reduce the incidence of infection in the first 12 months after KT.</p><p><strong>Methods: </strong>A single-center prospective cohort of 148 patients undergoing KT between February 2018 and September 2019 that received an individualized infection prevention strategy was compared to a preintervention cohort (n = 159). The bundle comprised a review of the patient's immunization history, infection risk by country of origin, screening for latent tuberculosis infection (LTBI), antimicrobial prophylaxis, and immunological assessment. Individualized recommendations were accordingly provided at a scheduled visit at day +30 after transplantation.</p><p><strong>Results: </strong>The intervention cohort showed a higher compliance rate with the recommended vaccine schedule, screening for geographically restricted infections and LTBI, and intravenous immunoglobulin and vitamin D supplementation (p values <.001). The 1-year incidence rate of infection was lower in the intervention cohort (42.6% vs. 57.9%; p value = .037), as was the rate of infection-related hospitalization (17.6% vs. 32.1%; p value = .003) and the incidence of severe bacterial infection. There were no differences in graft rejection or mortality rates between groups.</p><p><strong>Conclusions: </strong>A multifaceted intervention, including a bundle of evidence-based practices, enhanced compliance with recommended preventive measures and was correlated with a reduction in the 12-month incidence of infection after KT.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e14354"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666872/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel intervention based on an individualized bundle of care to decrease infection in kidney transplant recipients.\",\"authors\":\"Lucía de Jorge-Huerta, José Tiago Silva, Mario Fernández-Ruiz, Isabel Rodríguez-Goncer, M Asunción Pérez-Jacoiste Asín, Tamara Ruiz-Merlo, Carlos Heredia-Mena, Esther González-Monte, Natalia Polanco, Rafael San Juan, Amado Andrés, José María Aguado, Francisco López-Medrano\",\"doi\":\"10.1111/tid.14354\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Infection remains a relevant complication after kidney transplantation (KT). A well-established strategy in modern medicine is the application of bundles of evidence-based practice in clinical settings. The objective of this study is to explore the application of a personalized bundle of measures aimed to reduce the incidence of infection in the first 12 months after KT.</p><p><strong>Methods: </strong>A single-center prospective cohort of 148 patients undergoing KT between February 2018 and September 2019 that received an individualized infection prevention strategy was compared to a preintervention cohort (n = 159). The bundle comprised a review of the patient's immunization history, infection risk by country of origin, screening for latent tuberculosis infection (LTBI), antimicrobial prophylaxis, and immunological assessment. Individualized recommendations were accordingly provided at a scheduled visit at day +30 after transplantation.</p><p><strong>Results: </strong>The intervention cohort showed a higher compliance rate with the recommended vaccine schedule, screening for geographically restricted infections and LTBI, and intravenous immunoglobulin and vitamin D supplementation (p values <.001). The 1-year incidence rate of infection was lower in the intervention cohort (42.6% vs. 57.9%; p value = .037), as was the rate of infection-related hospitalization (17.6% vs. 32.1%; p value = .003) and the incidence of severe bacterial infection. There were no differences in graft rejection or mortality rates between groups.</p><p><strong>Conclusions: </strong>A multifaceted intervention, including a bundle of evidence-based practices, enhanced compliance with recommended preventive measures and was correlated with a reduction in the 12-month incidence of infection after KT.</p>\",\"PeriodicalId\":23318,\"journal\":{\"name\":\"Transplant Infectious Disease\",\"volume\":\" \",\"pages\":\"e14354\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666872/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant Infectious Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/tid.14354\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.14354","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/13 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Novel intervention based on an individualized bundle of care to decrease infection in kidney transplant recipients.
Background: Infection remains a relevant complication after kidney transplantation (KT). A well-established strategy in modern medicine is the application of bundles of evidence-based practice in clinical settings. The objective of this study is to explore the application of a personalized bundle of measures aimed to reduce the incidence of infection in the first 12 months after KT.
Methods: A single-center prospective cohort of 148 patients undergoing KT between February 2018 and September 2019 that received an individualized infection prevention strategy was compared to a preintervention cohort (n = 159). The bundle comprised a review of the patient's immunization history, infection risk by country of origin, screening for latent tuberculosis infection (LTBI), antimicrobial prophylaxis, and immunological assessment. Individualized recommendations were accordingly provided at a scheduled visit at day +30 after transplantation.
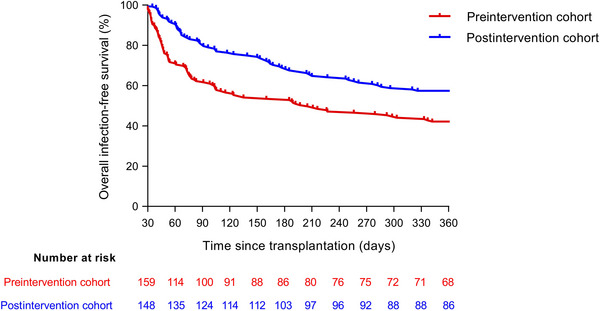
Results: The intervention cohort showed a higher compliance rate with the recommended vaccine schedule, screening for geographically restricted infections and LTBI, and intravenous immunoglobulin and vitamin D supplementation (p values <.001). The 1-year incidence rate of infection was lower in the intervention cohort (42.6% vs. 57.9%; p value = .037), as was the rate of infection-related hospitalization (17.6% vs. 32.1%; p value = .003) and the incidence of severe bacterial infection. There were no differences in graft rejection or mortality rates between groups.
Conclusions: A multifaceted intervention, including a bundle of evidence-based practices, enhanced compliance with recommended preventive measures and was correlated with a reduction in the 12-month incidence of infection after KT.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
