Tamazoust Guiddir, Audrey Siberil, Françoise Lepape, Marion Hacker, Ariane Nemni
{"title":"腰果过敏会自愈吗?","authors":"Tamazoust Guiddir, Audrey Siberil, Françoise Lepape, Marion Hacker, Ariane Nemni","doi":"10.1002/clt2.12385","DOIUrl":null,"url":null,"abstract":"<p>To the Editor</p><p>Cashew nut allergy (CNA) is increasing worldwide and is responsible for severe anaphylaxis, particularly in young children.<span><sup>1</sup></span> Symptoms range from mild reactions to severe anaphylaxis. The three main allergens are storage proteins: Ana o 1, Ana o 2 (cupin superfamily) and Ana o 3 (prolamin superfamily).<span><sup>2</sup></span> Lifetime avoidance of cashew nut is currently recommended for those with CNA. However, little is known about the natural history of CNA.</p><p>We report a cohort of five children with severe anaphylaxis to cashew nut who recovered and were able to eat cashew nut after a successful oral food challenge (Table 1). They all presented severe anaphylaxis according to the ordinal food allergy severity score (oFAAS-5)<span><sup>3</sup></span> (grade 3 to grade 5) at diagnosis at a mean age of 3 years [1.5–4]. Two patients had no atopy, one had a personal and familial atopic history and two others had only personal atopy. They all had no allergies or sensitizations to peanuts or tree nuts. Three patients consumed native cashew (between one and three cashew units) during the first reaction and two patients consumed cashew in cooked meals (unknown quantity). Allergology explorations were performed a mean 1.1 years [0.15–5] after the first reaction. All patients were sensitized to pistachio, but only two had a confirmed food allergy to pistachio. Skin prick tests (SPTs) were performed with commercial extract (ALK-Abello) and were deemed positive when wheal size was ≥ 3 mm. Cashew SPTs were positive for four children (mean 6 mm, range [3–20]). Cashew-specific IgEs (ImmunoCap® by Phadia 1000 System, Thermo Fisher Scientific) were positive for all patients, with a mean of 1 KU/L [0.36–2.49]. The recombinant Ana o 3 was not tested for at diagnosis for three patients and was positive for two of them (0.63 and 1.97 KU/L). After the reaction, they all observed strict avoidance of cashew and pistachio in their diet, without any recurrence. During a mean follow-up of 2.4 years (range [1–4]), the SPT and the cashew-specific IgEs became negative (Figure 1) and all patients tested negative for recombinant Ana o 3. An oral food challenge in four patients was successful at a cashew nut cumulated dose of 7800 mg. One patient refused the challenge, but after a successful pistachio challenge, he ate one cashew unit at home without any reaction.</p><p>We reported the cases of five children who presented severe anaphylaxis to cashew nut and who spontaneously recovered after a mean follow-up of 2.4 years [1–4]. As for peanut, ingestion of cashew is associated with a high rate of severe anaphylactic reactions,<span><sup>4</sup></span> but in our cohort it seemed not to be correlated with persistence of the allergy. Oral immunotherapy (OIT) may help develop tolerance to cashew, as reported by Elizur et al.<span><sup>5</sup></span> in a cohort of 50 children aged >4 years, who presented severe clinical reactions with cutaneous and biological sensitization. At the end of their protocol, 88% of the children were able to consume 4000 mg of cashew, and 94% ate more than 1200 mg. However, severe reactions were reported during OIT, with use of epinephrine during consultation in the emergency department. This tolerance was obtained by consuming cashew nut daily. Concerning our patients, cashew tolerance was achieved spontaneously after a cashew avoidance diet. In our cohort, data on recombinant Ana o 3 sensitization at diagnosis were not available for 3 patients, but all patients tested negative for recombinant Ana o 3 after follow-up. We hypothesize that all patients were positive for recombinant Ana o 3 at diagnosis, as all had severe clinical anaphylaxis at the first reaction. Recombinant Ana o 3 is associated with severe anaphylaxis to cashew nut, with a specificity of 94%.<span><sup>6</sup></span> In the cohort of Elizur et al., recombinant Ana o 3 was high at diagnosis in all patients and did not significantly decrease in control patients (Ana o 3- sIgE, median 8.3–5.9 kU/L, <i>p</i> = 0.5) but only in desensitized patients (median 3.7–1.6 kU/L, <i>p</i> < 0.001). In their study, the median follow-up was 12 months (range, 3–57 months) in desensitized patients and 17 months (range, 5–44.1 months) in control patients, whereas in our cohort, the mean follow-up was 28 months [12–48], which could require a longer follow-up to monitor IgEs and SPTs. As described by Foong et al., tree nut-specific IgE <2 KU/L may be predictive of resolution of allergy during follow-up.<span><sup>7</sup></span> However, in cashew allergy, there is a discordance between clinical and laboratory findings as specific IgEs are not always high in patients with severe anaphylaxis.<span><sup>6</sup></span></p><p>To conclude, we propose that clinicians should continue to perform SPTs and monitor cashew-specific IgEs even if the first reaction is severe, as it is possible that sensitization to cashew may spontaneously disappear. Oral food challenge can be then proposed if the laboratory parameters became negative, in order to confirm the recovery. Prospective studies will help confirm our hypothesis that CNA may resolve spontaneously.</p><p><b>Tamazoust Guiddir</b>: Conceptualization, investigation, methodology, validation, writing - review & editing, writing - original draft, formal analysis. <b>Audrey Siberil</b>: Methodology, writing - original draft, investigation. <b>Francoise Lepape</b>: Methodology, investigation. <b>Marion Hacker</b>: Writing - original draft, methodology, investigation. <b>Ariane Nemni</b>: Conceptualization, investigation, methodology, validation, writing - review & editing, writing - original draft, supervision.</p><p>The authors declare that they have no conflicts of interest for this article.</p>","PeriodicalId":10334,"journal":{"name":"Clinical and Translational Allergy","volume":"14 8","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.12385","citationCount":"0","resultStr":"{\"title\":\"Can cashew nut allergy resolve spontaneously?\",\"authors\":\"Tamazoust Guiddir, Audrey Siberil, Françoise Lepape, Marion Hacker, Ariane Nemni\",\"doi\":\"10.1002/clt2.12385\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>To the Editor</p><p>Cashew nut allergy (CNA) is increasing worldwide and is responsible for severe anaphylaxis, particularly in young children.<span><sup>1</sup></span> Symptoms range from mild reactions to severe anaphylaxis. The three main allergens are storage proteins: Ana o 1, Ana o 2 (cupin superfamily) and Ana o 3 (prolamin superfamily).<span><sup>2</sup></span> Lifetime avoidance of cashew nut is currently recommended for those with CNA. However, little is known about the natural history of CNA.</p><p>We report a cohort of five children with severe anaphylaxis to cashew nut who recovered and were able to eat cashew nut after a successful oral food challenge (Table 1). They all presented severe anaphylaxis according to the ordinal food allergy severity score (oFAAS-5)<span><sup>3</sup></span> (grade 3 to grade 5) at diagnosis at a mean age of 3 years [1.5–4]. Two patients had no atopy, one had a personal and familial atopic history and two others had only personal atopy. They all had no allergies or sensitizations to peanuts or tree nuts. Three patients consumed native cashew (between one and three cashew units) during the first reaction and two patients consumed cashew in cooked meals (unknown quantity). Allergology explorations were performed a mean 1.1 years [0.15–5] after the first reaction. All patients were sensitized to pistachio, but only two had a confirmed food allergy to pistachio. Skin prick tests (SPTs) were performed with commercial extract (ALK-Abello) and were deemed positive when wheal size was ≥ 3 mm. Cashew SPTs were positive for four children (mean 6 mm, range [3–20]). Cashew-specific IgEs (ImmunoCap® by Phadia 1000 System, Thermo Fisher Scientific) were positive for all patients, with a mean of 1 KU/L [0.36–2.49]. The recombinant Ana o 3 was not tested for at diagnosis for three patients and was positive for two of them (0.63 and 1.97 KU/L). After the reaction, they all observed strict avoidance of cashew and pistachio in their diet, without any recurrence. During a mean follow-up of 2.4 years (range [1–4]), the SPT and the cashew-specific IgEs became negative (Figure 1) and all patients tested negative for recombinant Ana o 3. An oral food challenge in four patients was successful at a cashew nut cumulated dose of 7800 mg. One patient refused the challenge, but after a successful pistachio challenge, he ate one cashew unit at home without any reaction.</p><p>We reported the cases of five children who presented severe anaphylaxis to cashew nut and who spontaneously recovered after a mean follow-up of 2.4 years [1–4]. As for peanut, ingestion of cashew is associated with a high rate of severe anaphylactic reactions,<span><sup>4</sup></span> but in our cohort it seemed not to be correlated with persistence of the allergy. Oral immunotherapy (OIT) may help develop tolerance to cashew, as reported by Elizur et al.<span><sup>5</sup></span> in a cohort of 50 children aged >4 years, who presented severe clinical reactions with cutaneous and biological sensitization. At the end of their protocol, 88% of the children were able to consume 4000 mg of cashew, and 94% ate more than 1200 mg. However, severe reactions were reported during OIT, with use of epinephrine during consultation in the emergency department. This tolerance was obtained by consuming cashew nut daily. Concerning our patients, cashew tolerance was achieved spontaneously after a cashew avoidance diet. In our cohort, data on recombinant Ana o 3 sensitization at diagnosis were not available for 3 patients, but all patients tested negative for recombinant Ana o 3 after follow-up. We hypothesize that all patients were positive for recombinant Ana o 3 at diagnosis, as all had severe clinical anaphylaxis at the first reaction. Recombinant Ana o 3 is associated with severe anaphylaxis to cashew nut, with a specificity of 94%.<span><sup>6</sup></span> In the cohort of Elizur et al., recombinant Ana o 3 was high at diagnosis in all patients and did not significantly decrease in control patients (Ana o 3- sIgE, median 8.3–5.9 kU/L, <i>p</i> = 0.5) but only in desensitized patients (median 3.7–1.6 kU/L, <i>p</i> < 0.001). In their study, the median follow-up was 12 months (range, 3–57 months) in desensitized patients and 17 months (range, 5–44.1 months) in control patients, whereas in our cohort, the mean follow-up was 28 months [12–48], which could require a longer follow-up to monitor IgEs and SPTs. As described by Foong et al., tree nut-specific IgE <2 KU/L may be predictive of resolution of allergy during follow-up.<span><sup>7</sup></span> However, in cashew allergy, there is a discordance between clinical and laboratory findings as specific IgEs are not always high in patients with severe anaphylaxis.<span><sup>6</sup></span></p><p>To conclude, we propose that clinicians should continue to perform SPTs and monitor cashew-specific IgEs even if the first reaction is severe, as it is possible that sensitization to cashew may spontaneously disappear. Oral food challenge can be then proposed if the laboratory parameters became negative, in order to confirm the recovery. Prospective studies will help confirm our hypothesis that CNA may resolve spontaneously.</p><p><b>Tamazoust Guiddir</b>: Conceptualization, investigation, methodology, validation, writing - review & editing, writing - original draft, formal analysis. <b>Audrey Siberil</b>: Methodology, writing - original draft, investigation. <b>Francoise Lepape</b>: Methodology, investigation. <b>Marion Hacker</b>: Writing - original draft, methodology, investigation. <b>Ariane Nemni</b>: Conceptualization, investigation, methodology, validation, writing - review & editing, writing - original draft, supervision.</p><p>The authors declare that they have no conflicts of interest for this article.</p>\",\"PeriodicalId\":10334,\"journal\":{\"name\":\"Clinical and Translational Allergy\",\"volume\":\"14 8\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.12385\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12385\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12385","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
摘要
致编辑腰果过敏(CNA)在全球范围内呈上升趋势,是导致严重过敏性休克的原因之一,尤其是在幼儿中。三种主要过敏原是贮存蛋白:Ana o 1、Ana o 2(cupin 超家族)和 Ana o 3(prolamin 超家族)。2 目前建议 CNA 患者终生避免食用腰果。然而,人们对 CNA 的自然病史知之甚少。我们报告了一组对腰果有严重过敏性休克的五名儿童,他们在成功接受口服食物挑战后恢复并能够食用腰果(表 1)。根据食物过敏严重程度顺序评分(oFAAS-5)3(3 级至 5 级),他们在确诊时均出现严重过敏性休克,平均年龄为 3 岁 [1.5-4]。两名患者没有过敏史,一名患者有个人和家族过敏史,另外两名患者只有个人过敏史。他们都对花生或树坚果没有过敏反应。三名患者在第一次反应期间食用了本地腰果(1 至 3 个腰果单位),两名患者在熟食中食用了腰果(数量不详)。在首次反应后平均 1.1 年 [0.15-5] 进行了过敏学检查。所有患者都对开心果过敏,但只有两名患者确诊对开心果食物过敏。皮肤点刺试验(SPTs)是用商品提取物(ALK-Abello)进行的,当出现≥3 毫米的皮疹时即为阳性。四名儿童的腰果 SPT 呈阳性(平均 6 毫米,范围 [3-20])。所有患者的腰果特异性 IgE(ImmunoCap® by Phadia 1000 System,赛默飞世尔科技公司)均呈阳性,平均值为 1 KU/L [0.36-2.49]。3 名患者在诊断时未检测重组 Ana o 3,其中 2 人呈阳性(0.63 和 1.97 KU/L)。反应发生后,他们都严格遵守了在饮食中避免食用腰果和开心果的规定,但没有复发。在平均 2.4 年(范围 [1-4])的随访期间,SPT 和腰果特异性 IgE 均为阴性(图 1),所有患者的重组 Ana o 3 检测结果均为阴性。四名患者成功接受了腰果累积剂量为 7800 毫克的口服食物挑战。一名患者拒绝接受挑战,但在挑战开心果成功后,他在家中吃了一个腰果单位,没有出现任何反应。我们曾报告过五名儿童对腰果出现严重过敏性休克的病例,他们在平均 2.4 年的随访后自发康复[1-4]。至于花生,摄入腰果与严重过敏性反应的发生率很高4,但在我们的队列中,这似乎与过敏的持续性无关。口服免疫疗法 (OIT) 可能有助于培养对腰果的耐受性,Elizur 等人5 对 50 名 4 岁儿童进行了研究,这些儿童出现了严重的皮肤和生物过敏临床反应。在治疗方案结束时,88% 的儿童能够食用 4000 毫克腰果,94% 的儿童食用量超过 1200 毫克。然而,据报告,在 OIT 期间出现了严重的反应,在急诊科就诊时使用了肾上腺素。这种耐受性是通过每天食用腰果获得的。就我们的患者而言,在避免食用腰果后,他们自然而然地对腰果产生了耐受性。在我们的队列中,有 3 名患者在诊断时没有重组 Ana o 3 致敏数据,但所有患者在随访后的重组 Ana o 3 检测结果均为阴性。我们推测所有患者在确诊时都对重组 Ana o 3 呈阳性反应,因为所有患者在首次反应时都出现了严重的临床过敏性休克。6 在 Elizur 等人的队列中,所有患者在诊断时重组 Ana o 3 均呈高水平,对照组患者(Ana o 3- sIgE,中位数为 8.3-5.9 kU/L,p = 0.5)的重组 Ana o 3 并未显著下降,而只有脱敏患者(中位数为 3.7-1.6 kU/L,p <0.001)的重组 Ana o 3 呈下降趋势。在他们的研究中,脱敏患者的中位随访时间为 12 个月(范围为 3-57 个月),对照组患者的中位随访时间为 17 个月(范围为 5-44.1 个月),而在我们的队列中,平均随访时间为 28 个月 [12-48],这可能需要更长时间的随访来监测 IgE 和 SPT。正如 Foong 等人所述,树坚果特异性 IgE <2 KU/L 可预测随访期间过敏症的缓解。7 然而,在腰果过敏症患者中,临床和实验室结果并不一致,因为严重过敏性休克患者的特异性 IgE 并不总是很高。如果实验室指标呈阴性,则可建议进行口服食物挑战,以确认恢复情况。
Cashew nut allergy (CNA) is increasing worldwide and is responsible for severe anaphylaxis, particularly in young children.1 Symptoms range from mild reactions to severe anaphylaxis. The three main allergens are storage proteins: Ana o 1, Ana o 2 (cupin superfamily) and Ana o 3 (prolamin superfamily).2 Lifetime avoidance of cashew nut is currently recommended for those with CNA. However, little is known about the natural history of CNA.
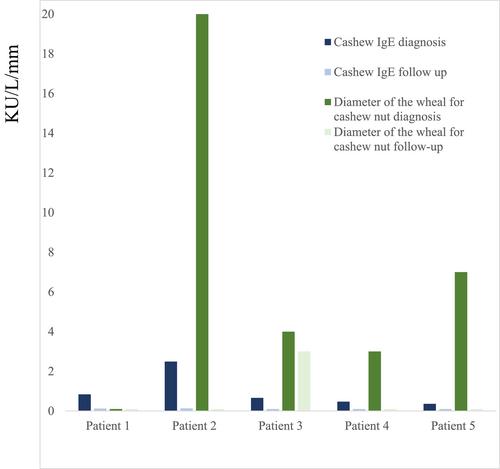
We report a cohort of five children with severe anaphylaxis to cashew nut who recovered and were able to eat cashew nut after a successful oral food challenge (Table 1). They all presented severe anaphylaxis according to the ordinal food allergy severity score (oFAAS-5)3 (grade 3 to grade 5) at diagnosis at a mean age of 3 years [1.5–4]. Two patients had no atopy, one had a personal and familial atopic history and two others had only personal atopy. They all had no allergies or sensitizations to peanuts or tree nuts. Three patients consumed native cashew (between one and three cashew units) during the first reaction and two patients consumed cashew in cooked meals (unknown quantity). Allergology explorations were performed a mean 1.1 years [0.15–5] after the first reaction. All patients were sensitized to pistachio, but only two had a confirmed food allergy to pistachio. Skin prick tests (SPTs) were performed with commercial extract (ALK-Abello) and were deemed positive when wheal size was ≥ 3 mm. Cashew SPTs were positive for four children (mean 6 mm, range [3–20]). Cashew-specific IgEs (ImmunoCap® by Phadia 1000 System, Thermo Fisher Scientific) were positive for all patients, with a mean of 1 KU/L [0.36–2.49]. The recombinant Ana o 3 was not tested for at diagnosis for three patients and was positive for two of them (0.63 and 1.97 KU/L). After the reaction, they all observed strict avoidance of cashew and pistachio in their diet, without any recurrence. During a mean follow-up of 2.4 years (range [1–4]), the SPT and the cashew-specific IgEs became negative (Figure 1) and all patients tested negative for recombinant Ana o 3. An oral food challenge in four patients was successful at a cashew nut cumulated dose of 7800 mg. One patient refused the challenge, but after a successful pistachio challenge, he ate one cashew unit at home without any reaction.
We reported the cases of five children who presented severe anaphylaxis to cashew nut and who spontaneously recovered after a mean follow-up of 2.4 years [1–4]. As for peanut, ingestion of cashew is associated with a high rate of severe anaphylactic reactions,4 but in our cohort it seemed not to be correlated with persistence of the allergy. Oral immunotherapy (OIT) may help develop tolerance to cashew, as reported by Elizur et al.5 in a cohort of 50 children aged >4 years, who presented severe clinical reactions with cutaneous and biological sensitization. At the end of their protocol, 88% of the children were able to consume 4000 mg of cashew, and 94% ate more than 1200 mg. However, severe reactions were reported during OIT, with use of epinephrine during consultation in the emergency department. This tolerance was obtained by consuming cashew nut daily. Concerning our patients, cashew tolerance was achieved spontaneously after a cashew avoidance diet. In our cohort, data on recombinant Ana o 3 sensitization at diagnosis were not available for 3 patients, but all patients tested negative for recombinant Ana o 3 after follow-up. We hypothesize that all patients were positive for recombinant Ana o 3 at diagnosis, as all had severe clinical anaphylaxis at the first reaction. Recombinant Ana o 3 is associated with severe anaphylaxis to cashew nut, with a specificity of 94%.6 In the cohort of Elizur et al., recombinant Ana o 3 was high at diagnosis in all patients and did not significantly decrease in control patients (Ana o 3- sIgE, median 8.3–5.9 kU/L, p = 0.5) but only in desensitized patients (median 3.7–1.6 kU/L, p < 0.001). In their study, the median follow-up was 12 months (range, 3–57 months) in desensitized patients and 17 months (range, 5–44.1 months) in control patients, whereas in our cohort, the mean follow-up was 28 months [12–48], which could require a longer follow-up to monitor IgEs and SPTs. As described by Foong et al., tree nut-specific IgE <2 KU/L may be predictive of resolution of allergy during follow-up.7 However, in cashew allergy, there is a discordance between clinical and laboratory findings as specific IgEs are not always high in patients with severe anaphylaxis.6
To conclude, we propose that clinicians should continue to perform SPTs and monitor cashew-specific IgEs even if the first reaction is severe, as it is possible that sensitization to cashew may spontaneously disappear. Oral food challenge can be then proposed if the laboratory parameters became negative, in order to confirm the recovery. Prospective studies will help confirm our hypothesis that CNA may resolve spontaneously.
期刊介绍:
Clinical and Translational Allergy, one of several journals in the portfolio of the European Academy of Allergy and Clinical Immunology, provides a platform for the dissemination of allergy research and reviews, as well as EAACI position papers, task force reports and guidelines, amongst an international scientific audience.
Clinical and Translational Allergy accepts clinical and translational research in the following areas and other related topics: asthma, rhinitis, rhinosinusitis, drug hypersensitivity, allergic conjunctivitis, allergic skin diseases, atopic eczema, urticaria, angioedema, venom hypersensitivity, anaphylaxis, food allergy, immunotherapy, immune modulators and biologics, animal models of allergic disease, immune mechanisms, or any other topic related to allergic disease.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
