Keegan M Hones, Kevin A Hao, Timothy R Buchanan, Amy P Trammell, Jonathan O Wright, Thomas W Wright, Tyler J LaMonica, Bradley S Schoch, Joseph J King
{"title":"对于患有盂肱骨关节炎和完整肩袖的解剖型或反向全肩关节置换术患者,术前前倾无力是否会影响临床效果?","authors":"Keegan M Hones, Kevin A Hao, Timothy R Buchanan, Amy P Trammell, Jonathan O Wright, Thomas W Wright, Tyler J LaMonica, Bradley S Schoch, Joseph J King","doi":"10.5397/cise.2024.00262","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study sought to determine if preoperative forward elevation (FE) weakness affects outcomes of anatomic (aTSA) and reverse total shoulder arthroplasty (rTSA) for patients with rotator cuff-intact glenohumeral osteoarthritis (RCI-GHOA).</p><p><strong>Methods: </strong>A retrospective review of a single institution's prospectively collected shoulder arthroplasty database was performed between 2007 and 2020, including 333 aTSAs and 155 rTSAs for primary RCI-GHOA with a minimum 2-year follow-up. Defining preoperative weakness as FE strength ≤4.9 lb (2.2 kg), three cohorts were matched 1:1:1 by age, sex, and follow-up: weak (n=82) to normal aTSAs, weak (n=44) to normal rTSAs, and weak aTSAs (n=61) to weak rTSAs. Compared outcomes included range of motion, outcome scores, and complication and revision rates at latest follow-up.</p><p><strong>Results: </strong>Weak aTSAs and weak rTSAs achieved similar postoperative outcome measures to normal aTSAs and normal rTSAs, respectively (P>0.05). Compared to weak rTSAs, weak aTSAs achieved superior postoperative passive (P=0.006) and active external rotation (ER) (P=0.014) but less favorable postoperative Shoulder Pain and Disability Index (P=0.032), American Shoulder and Elbow Surgeons (P=0.024), and University of California, Los Angeles scores (P=0.008). Weak aTSAs achieved the minimal clinically important difference and substantial clinical benefit at a lower rate for abduction (P=0.045 and P=0.003) and FE (P=0.011 and P=0.001). Weak aTSAs had a higher revision rate (P=0.025) but a similar complication rate (P=0.291) compared to weak rTSAs.</p><p><strong>Conclusions: </strong>Patients with RCI-GHOA and preoperative FE weakness obtain postoperative outcomes similar to patients with normal preoperative strength after either aTSA or rTSA. Preoperatively, weak aTSAs achieved greater ER but lower rates of clinically relevant improvement in overhead motion compared to weak rTSAs. Level of evidence: III.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":" ","pages":"316-326"},"PeriodicalIF":1.7000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11393438/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does preoperative forward elevation weakness affect clinical outcomes in anatomic or reverse total shoulder arthroplasty patients with glenohumeral osteoarthritis and intact rotator cuff?\",\"authors\":\"Keegan M Hones, Kevin A Hao, Timothy R Buchanan, Amy P Trammell, Jonathan O Wright, Thomas W Wright, Tyler J LaMonica, Bradley S Schoch, Joseph J King\",\"doi\":\"10.5397/cise.2024.00262\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study sought to determine if preoperative forward elevation (FE) weakness affects outcomes of anatomic (aTSA) and reverse total shoulder arthroplasty (rTSA) for patients with rotator cuff-intact glenohumeral osteoarthritis (RCI-GHOA).</p><p><strong>Methods: </strong>A retrospective review of a single institution's prospectively collected shoulder arthroplasty database was performed between 2007 and 2020, including 333 aTSAs and 155 rTSAs for primary RCI-GHOA with a minimum 2-year follow-up. Defining preoperative weakness as FE strength ≤4.9 lb (2.2 kg), three cohorts were matched 1:1:1 by age, sex, and follow-up: weak (n=82) to normal aTSAs, weak (n=44) to normal rTSAs, and weak aTSAs (n=61) to weak rTSAs. Compared outcomes included range of motion, outcome scores, and complication and revision rates at latest follow-up.</p><p><strong>Results: </strong>Weak aTSAs and weak rTSAs achieved similar postoperative outcome measures to normal aTSAs and normal rTSAs, respectively (P>0.05). Compared to weak rTSAs, weak aTSAs achieved superior postoperative passive (P=0.006) and active external rotation (ER) (P=0.014) but less favorable postoperative Shoulder Pain and Disability Index (P=0.032), American Shoulder and Elbow Surgeons (P=0.024), and University of California, Los Angeles scores (P=0.008). Weak aTSAs achieved the minimal clinically important difference and substantial clinical benefit at a lower rate for abduction (P=0.045 and P=0.003) and FE (P=0.011 and P=0.001). Weak aTSAs had a higher revision rate (P=0.025) but a similar complication rate (P=0.291) compared to weak rTSAs.</p><p><strong>Conclusions: </strong>Patients with RCI-GHOA and preoperative FE weakness obtain postoperative outcomes similar to patients with normal preoperative strength after either aTSA or rTSA. Preoperatively, weak aTSAs achieved greater ER but lower rates of clinically relevant improvement in overhead motion compared to weak rTSAs. Level of evidence: III.</p>\",\"PeriodicalId\":33981,\"journal\":{\"name\":\"Clinics in Shoulder and Elbow\",\"volume\":\" \",\"pages\":\"316-326\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11393438/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics in Shoulder and Elbow\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5397/cise.2024.00262\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2024.00262","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Does preoperative forward elevation weakness affect clinical outcomes in anatomic or reverse total shoulder arthroplasty patients with glenohumeral osteoarthritis and intact rotator cuff?
Background: This study sought to determine if preoperative forward elevation (FE) weakness affects outcomes of anatomic (aTSA) and reverse total shoulder arthroplasty (rTSA) for patients with rotator cuff-intact glenohumeral osteoarthritis (RCI-GHOA).
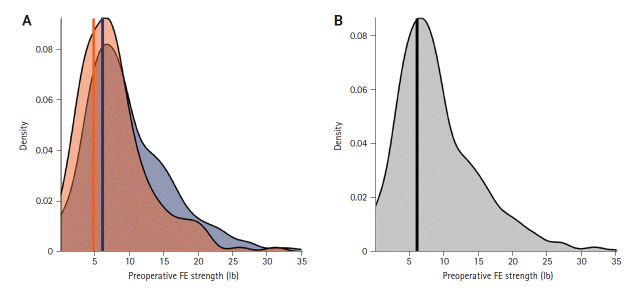
Methods: A retrospective review of a single institution's prospectively collected shoulder arthroplasty database was performed between 2007 and 2020, including 333 aTSAs and 155 rTSAs for primary RCI-GHOA with a minimum 2-year follow-up. Defining preoperative weakness as FE strength ≤4.9 lb (2.2 kg), three cohorts were matched 1:1:1 by age, sex, and follow-up: weak (n=82) to normal aTSAs, weak (n=44) to normal rTSAs, and weak aTSAs (n=61) to weak rTSAs. Compared outcomes included range of motion, outcome scores, and complication and revision rates at latest follow-up.
Results: Weak aTSAs and weak rTSAs achieved similar postoperative outcome measures to normal aTSAs and normal rTSAs, respectively (P>0.05). Compared to weak rTSAs, weak aTSAs achieved superior postoperative passive (P=0.006) and active external rotation (ER) (P=0.014) but less favorable postoperative Shoulder Pain and Disability Index (P=0.032), American Shoulder and Elbow Surgeons (P=0.024), and University of California, Los Angeles scores (P=0.008). Weak aTSAs achieved the minimal clinically important difference and substantial clinical benefit at a lower rate for abduction (P=0.045 and P=0.003) and FE (P=0.011 and P=0.001). Weak aTSAs had a higher revision rate (P=0.025) but a similar complication rate (P=0.291) compared to weak rTSAs.
Conclusions: Patients with RCI-GHOA and preoperative FE weakness obtain postoperative outcomes similar to patients with normal preoperative strength after either aTSA or rTSA. Preoperatively, weak aTSAs achieved greater ER but lower rates of clinically relevant improvement in overhead motion compared to weak rTSAs. Level of evidence: III.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
