Philip Enström, Andreas Martinsson, Mary Rezk, Susanne Nielsen, Erik Björklund, Maya Landenhed-Smith, Emily Pan, Anders Jeppsson
{"title":"四项 PRECISE-DAPT 评分可识别出出院后大出血风险较高的冠状动脉旁路移植术患者。","authors":"Philip Enström, Andreas Martinsson, Mary Rezk, Susanne Nielsen, Erik Björklund, Maya Landenhed-Smith, Emily Pan, Anders Jeppsson","doi":"10.1093/ehjcvp/pvae060","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Early identification of patients with increased bleeding risk increases the possibility to individualize antithrombotic treatment. We validated the PRECISE-DAPT score, originally developed to estimate bleeding risk in patients on dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI), in coronary artery bypass grafting (CABG) patients.</p><p><strong>Methods and results: </strong>All patients who underwent the first time, isolated CABG in Sweden 2009-2020 and survived until discharge were included. The four-item PRECISE-DAPT score, based on age, estimated glomerular filtration rate, pre-operative haemoglobin concentration, and previous spontaneous bleeding, was calculated in patients discharged on DAPT (n = 6838), or antiplatelet monotherapy (n = 15 406). High bleeding risk was defined as a score ≥25 in accordance with previous studies and major bleeding as hospitalization due to bleeding. Associations were assessed by C-statistics and Cox regression models. Major bleeding occurred during the first post-operative year in 130 patients (1.9%) in the DAPT group, and in 197 patients (1.3%) in the monotherapy group. The score identified 32.9% of the patients in the DAPT group and 38.2% in the monotherapy groups as having high bleeding risk. The area under the ROC-curve for the score was 0.67 (95%CI 0.62-0.72) for DAPT and 0.71 (0.67-0.74) for monotherapy. The hazard ratio for high bleeding risk vs. very low risk was 4.14 (2.07-8.26) for DAPT patients, and 4.95 (2.61-9.39) for monotherapy patients, both P < 0.001.</p><p><strong>Conclusion: </strong>The PRECISE-DAPT identifies patients with increased risk for major bleeding after discharge following CABG with moderate accuracy. The accuracy is comparable to what previously has been reported for patients after PCI.</p>","PeriodicalId":11982,"journal":{"name":"European Heart Journal - Cardiovascular Pharmacotherapy","volume":" ","pages":"48-56"},"PeriodicalIF":6.1000,"publicationDate":"2025-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11805682/pdf/","citationCount":"0","resultStr":"{\"title\":\"The four-item PRECISE-DAPT score identifies coronary artery bypass grafting patients with increased risk for post-discharge major bleeding.\",\"authors\":\"Philip Enström, Andreas Martinsson, Mary Rezk, Susanne Nielsen, Erik Björklund, Maya Landenhed-Smith, Emily Pan, Anders Jeppsson\",\"doi\":\"10.1093/ehjcvp/pvae060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Early identification of patients with increased bleeding risk increases the possibility to individualize antithrombotic treatment. We validated the PRECISE-DAPT score, originally developed to estimate bleeding risk in patients on dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI), in coronary artery bypass grafting (CABG) patients.</p><p><strong>Methods and results: </strong>All patients who underwent the first time, isolated CABG in Sweden 2009-2020 and survived until discharge were included. The four-item PRECISE-DAPT score, based on age, estimated glomerular filtration rate, pre-operative haemoglobin concentration, and previous spontaneous bleeding, was calculated in patients discharged on DAPT (n = 6838), or antiplatelet monotherapy (n = 15 406). High bleeding risk was defined as a score ≥25 in accordance with previous studies and major bleeding as hospitalization due to bleeding. Associations were assessed by C-statistics and Cox regression models. Major bleeding occurred during the first post-operative year in 130 patients (1.9%) in the DAPT group, and in 197 patients (1.3%) in the monotherapy group. The score identified 32.9% of the patients in the DAPT group and 38.2% in the monotherapy groups as having high bleeding risk. The area under the ROC-curve for the score was 0.67 (95%CI 0.62-0.72) for DAPT and 0.71 (0.67-0.74) for monotherapy. The hazard ratio for high bleeding risk vs. very low risk was 4.14 (2.07-8.26) for DAPT patients, and 4.95 (2.61-9.39) for monotherapy patients, both P < 0.001.</p><p><strong>Conclusion: </strong>The PRECISE-DAPT identifies patients with increased risk for major bleeding after discharge following CABG with moderate accuracy. The accuracy is comparable to what previously has been reported for patients after PCI.</p>\",\"PeriodicalId\":11982,\"journal\":{\"name\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"volume\":\" \",\"pages\":\"48-56\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2025-02-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11805682/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcvp/pvae060\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvae060","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The four-item PRECISE-DAPT score identifies coronary artery bypass grafting patients with increased risk for post-discharge major bleeding.
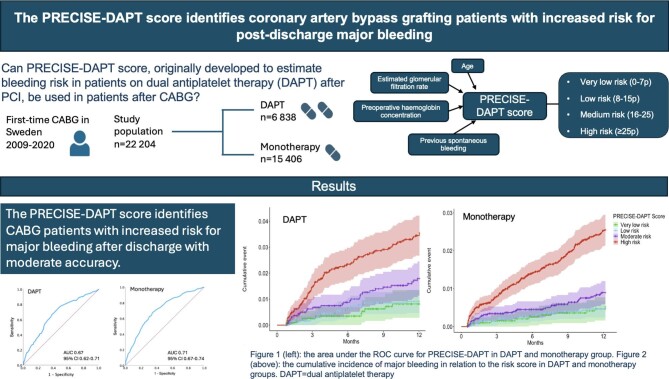
Aims: Early identification of patients with increased bleeding risk increases the possibility to individualize antithrombotic treatment. We validated the PRECISE-DAPT score, originally developed to estimate bleeding risk in patients on dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI), in coronary artery bypass grafting (CABG) patients.
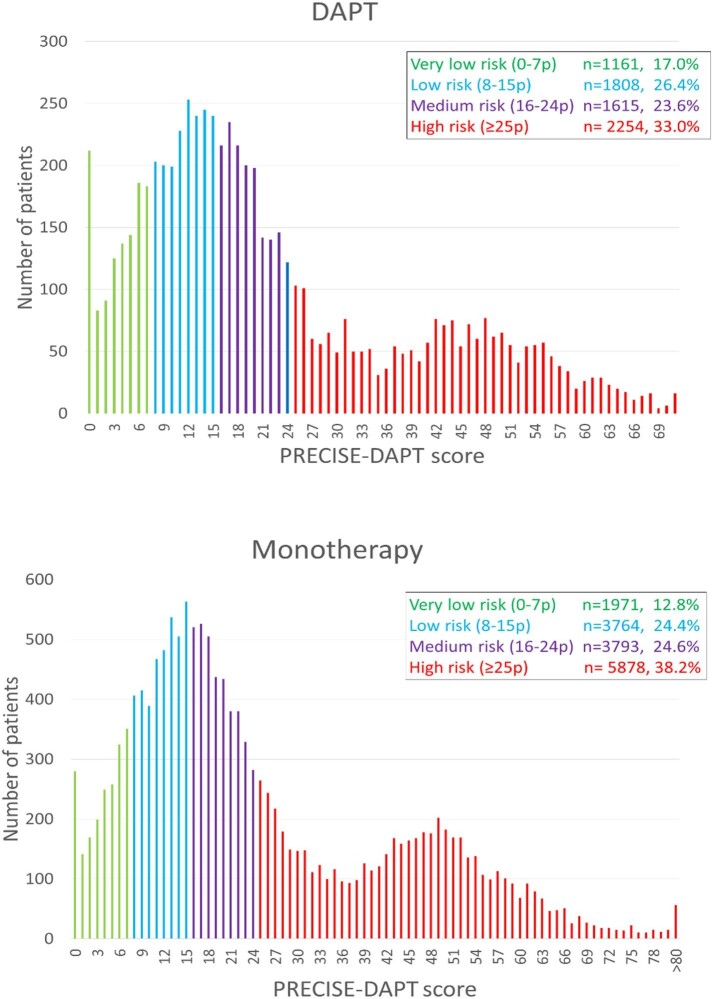
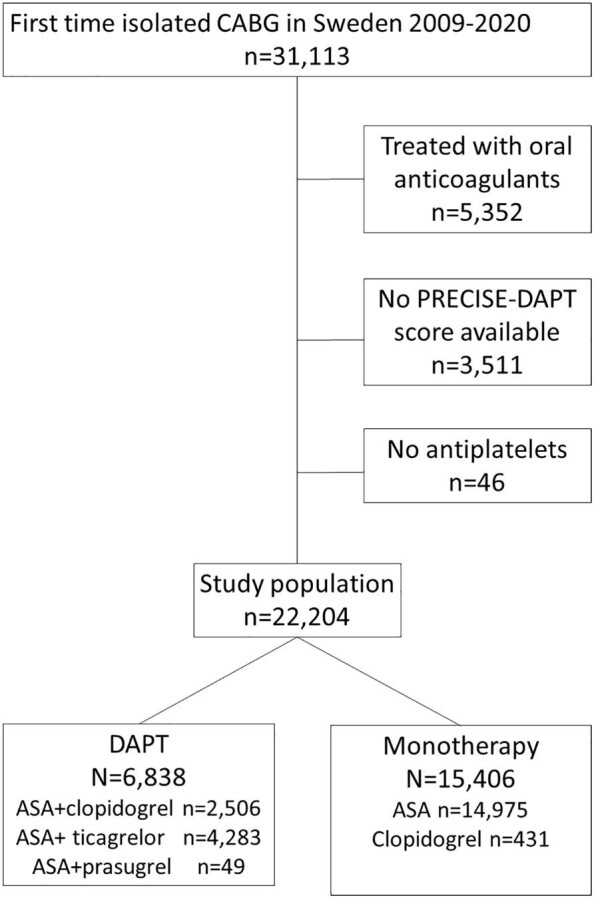
Methods and results: All patients who underwent the first time, isolated CABG in Sweden 2009-2020 and survived until discharge were included. The four-item PRECISE-DAPT score, based on age, estimated glomerular filtration rate, pre-operative haemoglobin concentration, and previous spontaneous bleeding, was calculated in patients discharged on DAPT (n = 6838), or antiplatelet monotherapy (n = 15 406). High bleeding risk was defined as a score ≥25 in accordance with previous studies and major bleeding as hospitalization due to bleeding. Associations were assessed by C-statistics and Cox regression models. Major bleeding occurred during the first post-operative year in 130 patients (1.9%) in the DAPT group, and in 197 patients (1.3%) in the monotherapy group. The score identified 32.9% of the patients in the DAPT group and 38.2% in the monotherapy groups as having high bleeding risk. The area under the ROC-curve for the score was 0.67 (95%CI 0.62-0.72) for DAPT and 0.71 (0.67-0.74) for monotherapy. The hazard ratio for high bleeding risk vs. very low risk was 4.14 (2.07-8.26) for DAPT patients, and 4.95 (2.61-9.39) for monotherapy patients, both P < 0.001.
Conclusion: The PRECISE-DAPT identifies patients with increased risk for major bleeding after discharge following CABG with moderate accuracy. The accuracy is comparable to what previously has been reported for patients after PCI.
期刊介绍:
The European Heart Journal - Cardiovascular Pharmacotherapy (EHJ-CVP) is an international, peer-reviewed journal published in English, specifically dedicated to clinical cardiovascular pharmacology. EHJ-CVP publishes original articles focusing on clinical research involving both new and established drugs and methods, along with meta-analyses and topical reviews. The journal's primary aim is to enhance the pharmacological treatment of patients with cardiovascular disease by interpreting and integrating new scientific developments in this field.
While the emphasis is on clinical topics, EHJ-CVP also considers basic research articles from fields such as physiology and molecular biology that contribute to the understanding of cardiovascular drug therapy. These may include articles related to new drug development and evaluation, the physiological and pharmacological basis of drug action, metabolism, drug interactions, and side effects.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
