T P Schlösser, I Blaauw, M R van der Valk, Guido van Solinge, C Faber, M C Kruyt
{"title":"脊柱侧弯手术中结构末端螺钉处的轴向杆滑脱:相关性、发生率和预防。","authors":"T P Schlösser, I Blaauw, M R van der Valk, Guido van Solinge, C Faber, M C Kruyt","doi":"10.1007/s43390-024-00925-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Despite standardized biomechanical tests for spinal implants, we recently recognized pedicle screw failure to maintain the rod fixated as a clinical concern in scoliosis surgery. This occurrence study investigates the risk and magnitude of axial rod slip (ARS), its relation with technique and preventive measures.</p><p><strong>Methods: </strong>Retrospective multicenter review of all primary scoliosis cases (2018-2020) with > 1 year FU from three centers, instrumented with uniplanar screws and 5.5 mm CoCr rods (Mesa 2, Stryker Corporation, Kalamazoo, MI, USA). ARS was defined as > 1 mm change in residual distal rod length from the screw in the lowest instrumented vertebra (LIV) and assessed by two independent observers. Slip distance, direction, relation to distal screw density and time of observation were recorded, as well as the effect of ARS on caudal curve increase. To prevent slip, more recent patients were instrumented with a different end-of-construct screw (Reline, NuVasive Inc. San Diego, CA, USA) and analyzed for comparison.</p><p><strong>Results: </strong>ARS risk was 27% (56/205) with a distance of 3.6 ± 2.2 mm, predominantly convex. 42% occurred before 4 months, the rest before 1 year. The caudal curve substantially increased three times more often in patients with ARS. Interobserver reliability was high and slip was in the expected direction. ARS was unrelated to distal screw density. Remarkable variation in ARS rates (53%, 31%, 13%) existed between the centers, while there was no difference in mean screw density (≈1.3 screws/level) or curve correction (≈60%). Revision surgery for ARS was required in 2.9% (6/207). Using the different end-of-construct screw, ARS risk was only 2% (1/56) and no revisions were required.</p><p><strong>Conclusion: </strong>This study demonstrates the prevalence of axial rod slip at the end of construct in scoliosis surgery and its clinical relevance. While minimal ARS can be subclinical, ARS should not be mistaken for adding on. The most severe ARS predominantly occurred convex at the high-loaded distal screw when L3 was the LIV. Longer constructs (LIV L3 or L4) have a higher risk of ARS. The minimal risk of ARS with another end-of-construct screw underscores the influence of screw type on ARS occurrence in our series. Further research is essential to refine techniques and enhance patient outcomes.</p>","PeriodicalId":21796,"journal":{"name":"Spine deformity","volume":" ","pages":"1699-1707"},"PeriodicalIF":1.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499526/pdf/","citationCount":"0","resultStr":"{\"title\":\"Axial rod slip at the end-of-construct screw in scoliosis surgery: relevance, occurrence and prevention.\",\"authors\":\"T P Schlösser, I Blaauw, M R van der Valk, Guido van Solinge, C Faber, M C Kruyt\",\"doi\":\"10.1007/s43390-024-00925-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Despite standardized biomechanical tests for spinal implants, we recently recognized pedicle screw failure to maintain the rod fixated as a clinical concern in scoliosis surgery. This occurrence study investigates the risk and magnitude of axial rod slip (ARS), its relation with technique and preventive measures.</p><p><strong>Methods: </strong>Retrospective multicenter review of all primary scoliosis cases (2018-2020) with > 1 year FU from three centers, instrumented with uniplanar screws and 5.5 mm CoCr rods (Mesa 2, Stryker Corporation, Kalamazoo, MI, USA). ARS was defined as > 1 mm change in residual distal rod length from the screw in the lowest instrumented vertebra (LIV) and assessed by two independent observers. Slip distance, direction, relation to distal screw density and time of observation were recorded, as well as the effect of ARS on caudal curve increase. To prevent slip, more recent patients were instrumented with a different end-of-construct screw (Reline, NuVasive Inc. San Diego, CA, USA) and analyzed for comparison.</p><p><strong>Results: </strong>ARS risk was 27% (56/205) with a distance of 3.6 ± 2.2 mm, predominantly convex. 42% occurred before 4 months, the rest before 1 year. The caudal curve substantially increased three times more often in patients with ARS. Interobserver reliability was high and slip was in the expected direction. ARS was unrelated to distal screw density. Remarkable variation in ARS rates (53%, 31%, 13%) existed between the centers, while there was no difference in mean screw density (≈1.3 screws/level) or curve correction (≈60%). Revision surgery for ARS was required in 2.9% (6/207). Using the different end-of-construct screw, ARS risk was only 2% (1/56) and no revisions were required.</p><p><strong>Conclusion: </strong>This study demonstrates the prevalence of axial rod slip at the end of construct in scoliosis surgery and its clinical relevance. While minimal ARS can be subclinical, ARS should not be mistaken for adding on. The most severe ARS predominantly occurred convex at the high-loaded distal screw when L3 was the LIV. Longer constructs (LIV L3 or L4) have a higher risk of ARS. The minimal risk of ARS with another end-of-construct screw underscores the influence of screw type on ARS occurrence in our series. Further research is essential to refine techniques and enhance patient outcomes.</p>\",\"PeriodicalId\":21796,\"journal\":{\"name\":\"Spine deformity\",\"volume\":\" \",\"pages\":\"1699-1707\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499526/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine deformity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s43390-024-00925-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine deformity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43390-024-00925-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Axial rod slip at the end-of-construct screw in scoliosis surgery: relevance, occurrence and prevention.
Purpose: Despite standardized biomechanical tests for spinal implants, we recently recognized pedicle screw failure to maintain the rod fixated as a clinical concern in scoliosis surgery. This occurrence study investigates the risk and magnitude of axial rod slip (ARS), its relation with technique and preventive measures.
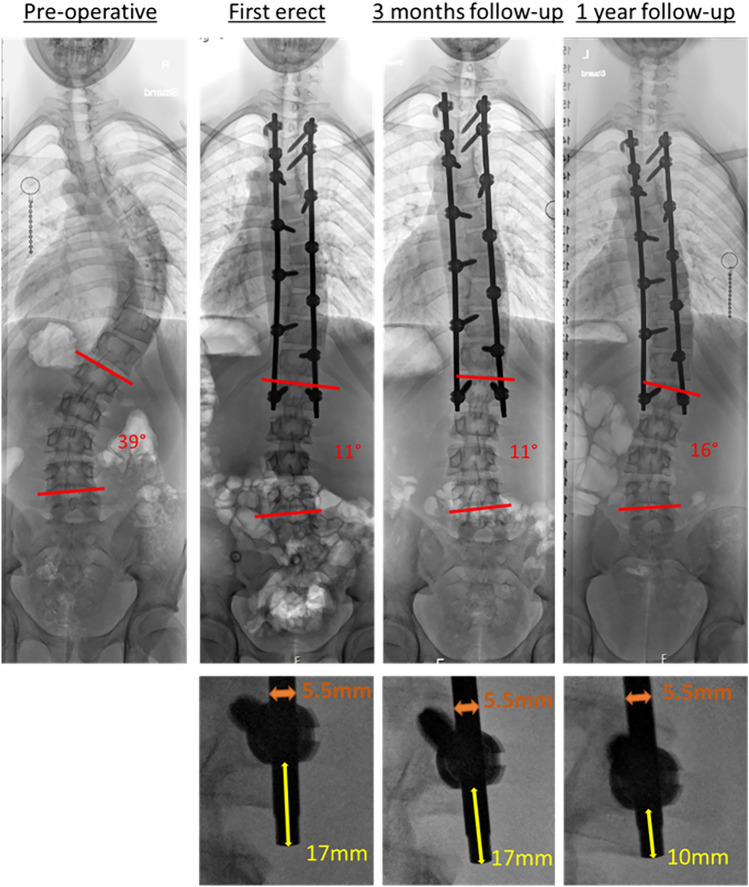
Methods: Retrospective multicenter review of all primary scoliosis cases (2018-2020) with > 1 year FU from three centers, instrumented with uniplanar screws and 5.5 mm CoCr rods (Mesa 2, Stryker Corporation, Kalamazoo, MI, USA). ARS was defined as > 1 mm change in residual distal rod length from the screw in the lowest instrumented vertebra (LIV) and assessed by two independent observers. Slip distance, direction, relation to distal screw density and time of observation were recorded, as well as the effect of ARS on caudal curve increase. To prevent slip, more recent patients were instrumented with a different end-of-construct screw (Reline, NuVasive Inc. San Diego, CA, USA) and analyzed for comparison.
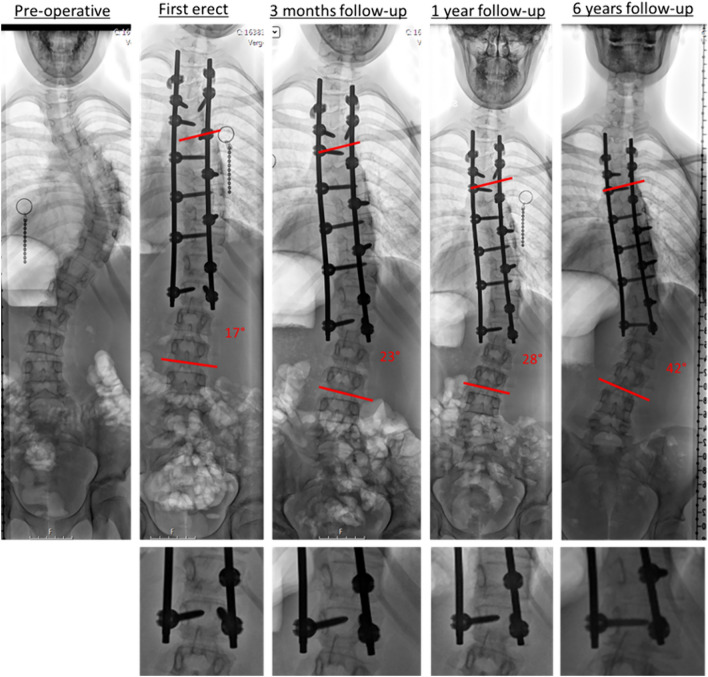
Results: ARS risk was 27% (56/205) with a distance of 3.6 ± 2.2 mm, predominantly convex. 42% occurred before 4 months, the rest before 1 year. The caudal curve substantially increased three times more often in patients with ARS. Interobserver reliability was high and slip was in the expected direction. ARS was unrelated to distal screw density. Remarkable variation in ARS rates (53%, 31%, 13%) existed between the centers, while there was no difference in mean screw density (≈1.3 screws/level) or curve correction (≈60%). Revision surgery for ARS was required in 2.9% (6/207). Using the different end-of-construct screw, ARS risk was only 2% (1/56) and no revisions were required.
Conclusion: This study demonstrates the prevalence of axial rod slip at the end of construct in scoliosis surgery and its clinical relevance. While minimal ARS can be subclinical, ARS should not be mistaken for adding on. The most severe ARS predominantly occurred convex at the high-loaded distal screw when L3 was the LIV. Longer constructs (LIV L3 or L4) have a higher risk of ARS. The minimal risk of ARS with another end-of-construct screw underscores the influence of screw type on ARS occurrence in our series. Further research is essential to refine techniques and enhance patient outcomes.
期刊介绍:
Spine Deformity the official journal of the?Scoliosis Research Society is a peer-refereed publication to disseminate knowledge on basic science and clinical research into the?etiology?biomechanics?treatment?methods and outcomes of all types of?spinal deformities. The international members of the Editorial Board provide a worldwide perspective for the journal's area of interest.The?journal?will enhance the mission of the Society which is to foster the optimal care of all patients with?spine?deformities worldwide. Articles published in?Spine Deformity?are Medline indexed in PubMed.? The journal publishes original articles in the form of clinical and basic research. Spine Deformity will only publish studies that have institutional review board (IRB) or similar ethics committee approval for human and animal studies and have strictly observed these guidelines. The minimum follow-up period for follow-up clinical studies is 24 months.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
