Alexander J Nedopil, Anand Singh Dhaliwal, Antonio Klasan, Stephen M Howell, Maury L Hull
{"title":"膝关节外翻骨关节炎患者的内侧副韧带伸长在影像学上无明显证据,因此可采用运动对齐全膝关节置换术进行治疗。","authors":"Alexander J Nedopil, Anand Singh Dhaliwal, Antonio Klasan, Stephen M Howell, Maury L Hull","doi":"10.1055/a-2395-6831","DOIUrl":null,"url":null,"abstract":"<p><p>When performing caliper-verified kinematically aligned total knee arthroplasty (KA TKA) in the osteoarthritic (OA) knee with valgus deformity, an elongated medial collateral ligament (MCL) could result in a valgus setting of the tibial component. The present study analyzed KA TKA in patients with valgus deformities (i.e., tibiofemoral angle > 10 degrees of valgus) and determined (1) the occurrence of radiographic MCL elongation, (2) the incidence of lateral collateral ligament (LCL) and posterior cruciate ligament (PCL) release and the use of constrained components, and (3) whether the 1-year Forgotten Joint Score (FJS), Oxford Knee Score (OKS), Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), and Likert satisfaction score were comparable to KA TKAs for OA deformities ≤10 degrees of valgus. One hundred and two consecutive patients who underwent KA TKA by a single surgeon were analyzed radiographically and clinically at a minimum follow-up of 1 year. Radiographic MCL elongation was identified by a greater than 1 degree of valgus orientation of the tibial component relative to the OA tibial joint line. Twenty-six patients had a radiographic anatomic tibiofemoral angle greater than 10 degrees of valgus (range of OA deformity: 11-23 degrees of valgus). Seventy-six had an OA deformity ≤10 degrees of valgus (10-degree valgus to -14-degree varus). No patient had MCL elongation or a ligament release, or required constrained components. The median FJS of 78, OKS of 42, and KOOS JR of 76, and the 85% satisfaction rate of the patients with greater than 10 degrees of OA valgus deformity were not significantly different from those with ≤10 degrees of OA valgus deformity (<i>p</i> ≥ 0.17). Because MCL elongation was not detected in OA deformities up to 23 degrees of valgus, the risk of under-correcting the valgus deformity leading to instability and poor outcome scores is low when performing KA TKA using primary components without releasing the LCL and/or PCL. LEVEL OF EVIDENCE:: IV.</p>","PeriodicalId":48798,"journal":{"name":"Journal of Knee Surgery","volume":" ","pages":"328-335"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143935/pdf/","citationCount":"0","resultStr":"{\"title\":\"No Radiographic Evidence of Medial Collateral Ligament Elongation in Valgus Osteoarthritic Knees Enables Treatment with Kinematically Aligned Total Knee Arthroplasty.\",\"authors\":\"Alexander J Nedopil, Anand Singh Dhaliwal, Antonio Klasan, Stephen M Howell, Maury L Hull\",\"doi\":\"10.1055/a-2395-6831\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>When performing caliper-verified kinematically aligned total knee arthroplasty (KA TKA) in the osteoarthritic (OA) knee with valgus deformity, an elongated medial collateral ligament (MCL) could result in a valgus setting of the tibial component. The present study analyzed KA TKA in patients with valgus deformities (i.e., tibiofemoral angle > 10 degrees of valgus) and determined (1) the occurrence of radiographic MCL elongation, (2) the incidence of lateral collateral ligament (LCL) and posterior cruciate ligament (PCL) release and the use of constrained components, and (3) whether the 1-year Forgotten Joint Score (FJS), Oxford Knee Score (OKS), Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), and Likert satisfaction score were comparable to KA TKAs for OA deformities ≤10 degrees of valgus. One hundred and two consecutive patients who underwent KA TKA by a single surgeon were analyzed radiographically and clinically at a minimum follow-up of 1 year. Radiographic MCL elongation was identified by a greater than 1 degree of valgus orientation of the tibial component relative to the OA tibial joint line. Twenty-six patients had a radiographic anatomic tibiofemoral angle greater than 10 degrees of valgus (range of OA deformity: 11-23 degrees of valgus). Seventy-six had an OA deformity ≤10 degrees of valgus (10-degree valgus to -14-degree varus). No patient had MCL elongation or a ligament release, or required constrained components. The median FJS of 78, OKS of 42, and KOOS JR of 76, and the 85% satisfaction rate of the patients with greater than 10 degrees of OA valgus deformity were not significantly different from those with ≤10 degrees of OA valgus deformity (<i>p</i> ≥ 0.17). Because MCL elongation was not detected in OA deformities up to 23 degrees of valgus, the risk of under-correcting the valgus deformity leading to instability and poor outcome scores is low when performing KA TKA using primary components without releasing the LCL and/or PCL. LEVEL OF EVIDENCE:: IV.</p>\",\"PeriodicalId\":48798,\"journal\":{\"name\":\"Journal of Knee Surgery\",\"volume\":\" \",\"pages\":\"328-335\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143935/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Knee Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2395-6831\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Knee Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2395-6831","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:在对伴有外翻畸形的骨关节炎(OA)膝关节进行卡尺验证的运动学配准全膝关节置换术(KA TKA)时,内侧副韧带(MCL)的拉长可能会导致胫骨组件的外翻设置。本研究分析了膝关节外翻畸形患者的 KA TKA(即、2)外侧副韧带(LCL)和后交叉韧带(PCL)松解的发生率以及受限组件的使用情况、3)对于髋关节外翻≤10°的OA畸形,一年的 "遗忘关节评分"(FJS)、"牛津膝关节评分"(OKS)、"膝关节损伤和骨关节炎关节置换术结果评分"(KOOS JR)和Likert满意度评分是否与KA TKAs相当。方法:对由一名外科医生实施 KA TKA 的 112 名连续患者进行了至少 1 年的放射学和临床随访分析。胫骨组件相对于OA胫骨关节线的外翻方向大于1°,即可确定MCL的影像学伸长:26名患者的胫股关节放射解剖角度大于10°外翻(OA畸形范围为11°至23°外翻)。76名患者的OA畸形≤10°外翻(10°外翻至-14°内翻)。没有患者出现 MCL 拉长、韧带松解或需要约束组件。OA外翻畸形大于10°的患者的FJS中位数为78,OKS中位数为42,KOOS JR中位数为76,满意率为85%,与OA外翻畸形小于10°的患者相比无显著差异(P≥0.17):由于在外翻23°以下的OA畸形中未检测到MCL伸长,因此在不释放LCL和/或PCL的情况下使用主组件进行KA TKA手术时,外翻畸形矫正不足导致不稳定和不良结果评分的风险很低。
No Radiographic Evidence of Medial Collateral Ligament Elongation in Valgus Osteoarthritic Knees Enables Treatment with Kinematically Aligned Total Knee Arthroplasty.
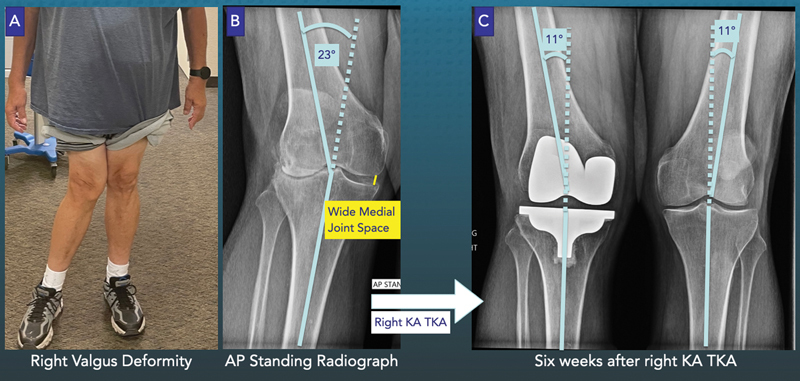
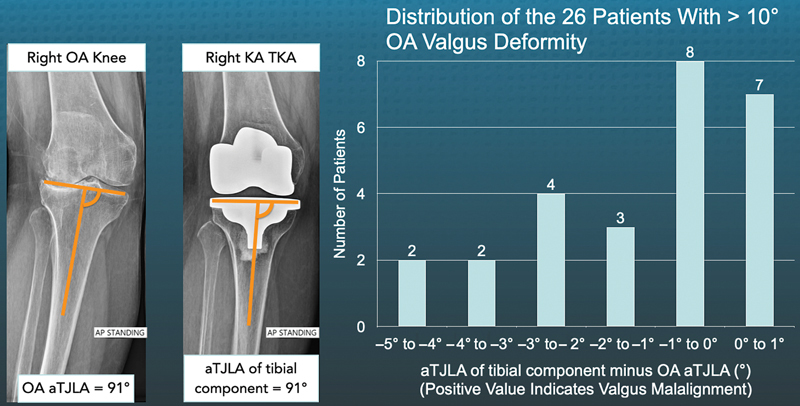
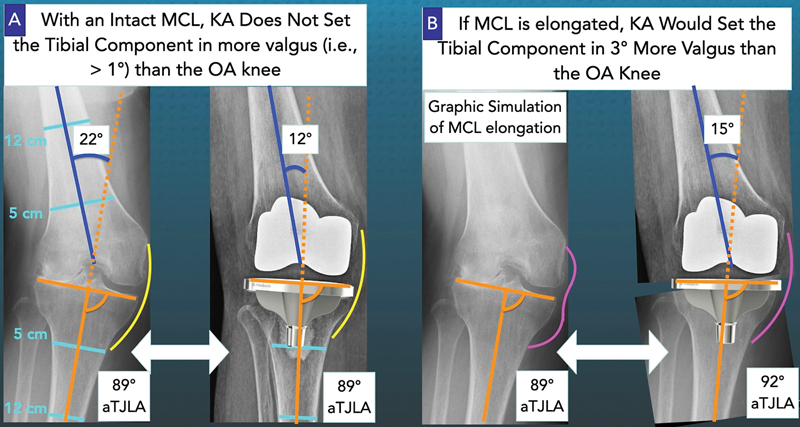
When performing caliper-verified kinematically aligned total knee arthroplasty (KA TKA) in the osteoarthritic (OA) knee with valgus deformity, an elongated medial collateral ligament (MCL) could result in a valgus setting of the tibial component. The present study analyzed KA TKA in patients with valgus deformities (i.e., tibiofemoral angle > 10 degrees of valgus) and determined (1) the occurrence of radiographic MCL elongation, (2) the incidence of lateral collateral ligament (LCL) and posterior cruciate ligament (PCL) release and the use of constrained components, and (3) whether the 1-year Forgotten Joint Score (FJS), Oxford Knee Score (OKS), Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), and Likert satisfaction score were comparable to KA TKAs for OA deformities ≤10 degrees of valgus. One hundred and two consecutive patients who underwent KA TKA by a single surgeon were analyzed radiographically and clinically at a minimum follow-up of 1 year. Radiographic MCL elongation was identified by a greater than 1 degree of valgus orientation of the tibial component relative to the OA tibial joint line. Twenty-six patients had a radiographic anatomic tibiofemoral angle greater than 10 degrees of valgus (range of OA deformity: 11-23 degrees of valgus). Seventy-six had an OA deformity ≤10 degrees of valgus (10-degree valgus to -14-degree varus). No patient had MCL elongation or a ligament release, or required constrained components. The median FJS of 78, OKS of 42, and KOOS JR of 76, and the 85% satisfaction rate of the patients with greater than 10 degrees of OA valgus deformity were not significantly different from those with ≤10 degrees of OA valgus deformity (p ≥ 0.17). Because MCL elongation was not detected in OA deformities up to 23 degrees of valgus, the risk of under-correcting the valgus deformity leading to instability and poor outcome scores is low when performing KA TKA using primary components without releasing the LCL and/or PCL. LEVEL OF EVIDENCE:: IV.
期刊介绍:
The Journal of Knee Surgery covers a range of issues relating to the orthopaedic techniques of arthroscopy, arthroplasty, and reconstructive surgery of the knee joint. In addition to original peer-review articles, this periodical provides details on emerging surgical techniques, as well as reviews and special focus sections. Topics of interest include cruciate ligament repair and reconstruction, bone grafting, cartilage regeneration, and magnetic resonance imaging.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
