Hyo Jeong Kim, Kyung Won Kim, Young Su Joo, Junghwa Ryu, Hee-Yeon Jung, Kyung Hwan Jeong, Myung-Gyu Kim, Man Ki Ju, Seungyeup Han, Jong Soo Lee, Kyung Pyo Kang, Han Ro, Kyo Won Lee, Kyu Ha Huh, Myoung Soo Kim, Beom Seok Kim, Jaeseok Yang
{"title":"血压对肾移植受者异体移植功能和存活率的影响","authors":"Hyo Jeong Kim, Kyung Won Kim, Young Su Joo, Junghwa Ryu, Hee-Yeon Jung, Kyung Hwan Jeong, Myung-Gyu Kim, Man Ki Ju, Seungyeup Han, Jong Soo Lee, Kyung Pyo Kang, Han Ro, Kyo Won Lee, Kyu Ha Huh, Myoung Soo Kim, Beom Seok Kim, Jaeseok Yang","doi":"10.3389/ti.2024.12574","DOIUrl":null,"url":null,"abstract":"<p><p>The optimal target blood pressure for kidney transplant (KT) patients remains unclear. We included 808 KT patients from the KNOW-KT as a discovery set, and 1,294 KT patients from the KOTRY as a validation set. The main exposures were baseline systolic blood pressure (SBP) at 1 year after KT and time-varying SBP. Patients were classified into five groups: SBP <110; 110-119; 120-129; 130-139; and ≥140 mmHg. SBP trajectories were classified into decreasing, stable, and increasing groups. Primary outcome was composite kidney outcome of ≥50% decrease in eGFR or death-censored graft loss. Compared with the 110-119 mmHg group, both the lowest (adjusted hazard ratio [aHR], 2.43) and the highest SBP (aHR, 2.25) were associated with a higher risk of composite kidney outcome. In time-varying model, also the lowest (aHR, 3.02) and the highest SBP (aHR, 3.60) were associated with a higher risk. In the trajectory model, an increasing SBP trajectory was associated with a higher risk than a stable SBP trajectory (aHR, 2.26). This associations were consistent in the validation set. In conclusion, SBP ≥140 mmHg and an increasing SBP trajectory were associated with a higher risk of allograft dysfunction and failure in KT patients.</p>","PeriodicalId":23343,"journal":{"name":"Transplant International","volume":"37 ","pages":"12574"},"PeriodicalIF":3.0000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11336573/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Blood Pressure on Allograft Function and Survival in Kidney Transplant Recipients.\",\"authors\":\"Hyo Jeong Kim, Kyung Won Kim, Young Su Joo, Junghwa Ryu, Hee-Yeon Jung, Kyung Hwan Jeong, Myung-Gyu Kim, Man Ki Ju, Seungyeup Han, Jong Soo Lee, Kyung Pyo Kang, Han Ro, Kyo Won Lee, Kyu Ha Huh, Myoung Soo Kim, Beom Seok Kim, Jaeseok Yang\",\"doi\":\"10.3389/ti.2024.12574\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The optimal target blood pressure for kidney transplant (KT) patients remains unclear. We included 808 KT patients from the KNOW-KT as a discovery set, and 1,294 KT patients from the KOTRY as a validation set. The main exposures were baseline systolic blood pressure (SBP) at 1 year after KT and time-varying SBP. Patients were classified into five groups: SBP <110; 110-119; 120-129; 130-139; and ≥140 mmHg. SBP trajectories were classified into decreasing, stable, and increasing groups. Primary outcome was composite kidney outcome of ≥50% decrease in eGFR or death-censored graft loss. Compared with the 110-119 mmHg group, both the lowest (adjusted hazard ratio [aHR], 2.43) and the highest SBP (aHR, 2.25) were associated with a higher risk of composite kidney outcome. In time-varying model, also the lowest (aHR, 3.02) and the highest SBP (aHR, 3.60) were associated with a higher risk. In the trajectory model, an increasing SBP trajectory was associated with a higher risk than a stable SBP trajectory (aHR, 2.26). This associations were consistent in the validation set. In conclusion, SBP ≥140 mmHg and an increasing SBP trajectory were associated with a higher risk of allograft dysfunction and failure in KT patients.</p>\",\"PeriodicalId\":23343,\"journal\":{\"name\":\"Transplant International\",\"volume\":\"37 \",\"pages\":\"12574\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11336573/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/ti.2024.12574\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/ti.2024.12574","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
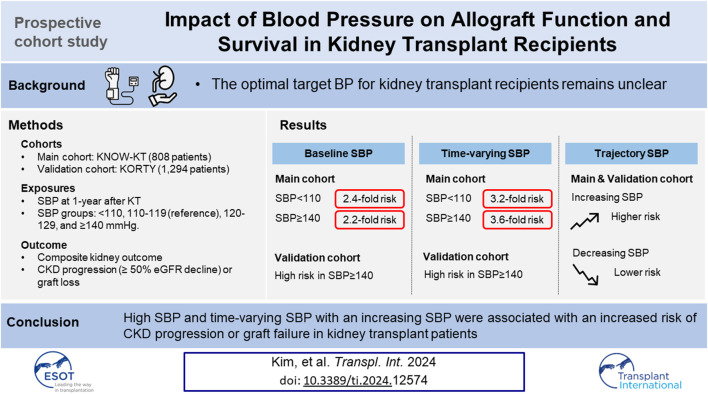
Impact of Blood Pressure on Allograft Function and Survival in Kidney Transplant Recipients.
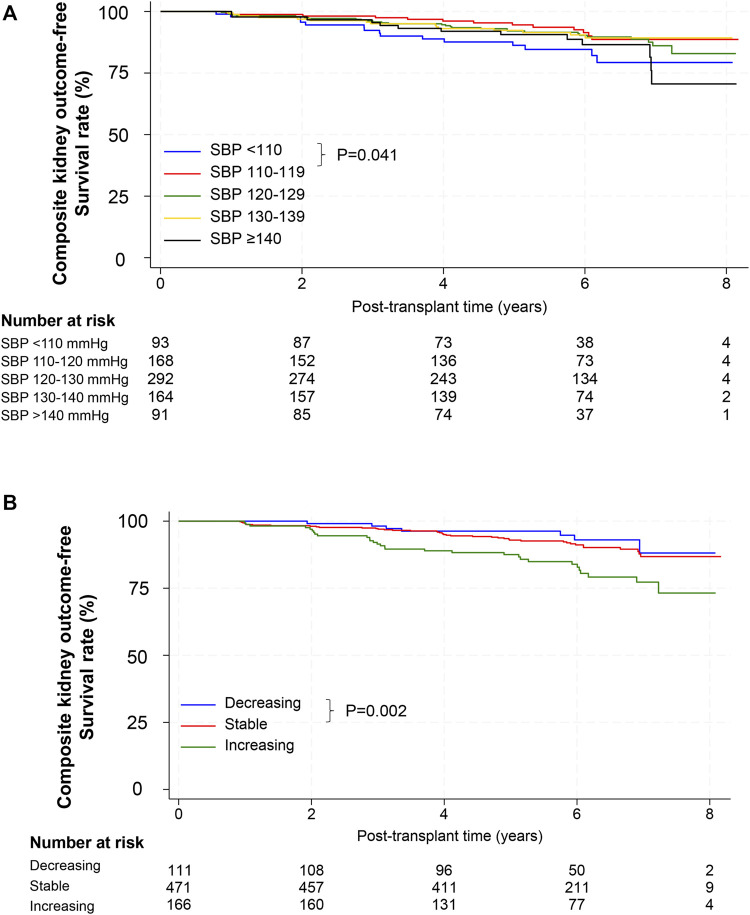
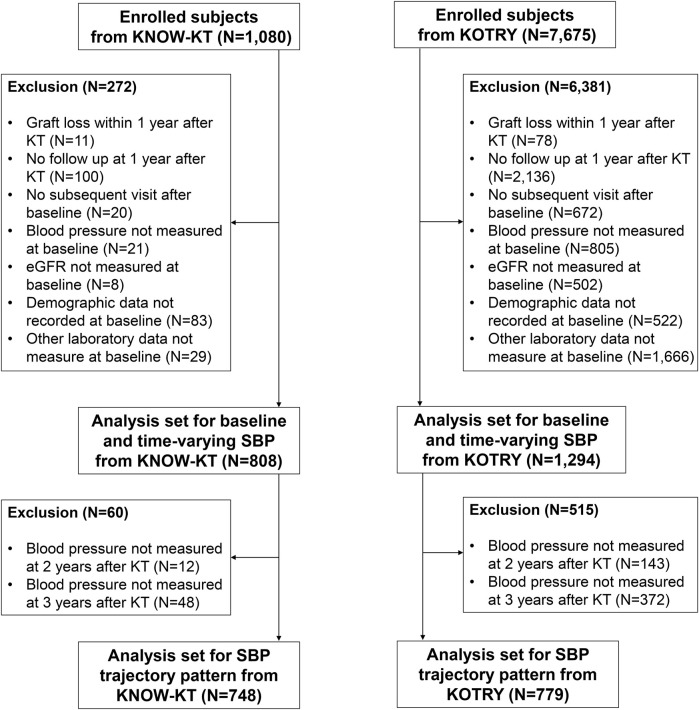
The optimal target blood pressure for kidney transplant (KT) patients remains unclear. We included 808 KT patients from the KNOW-KT as a discovery set, and 1,294 KT patients from the KOTRY as a validation set. The main exposures were baseline systolic blood pressure (SBP) at 1 year after KT and time-varying SBP. Patients were classified into five groups: SBP <110; 110-119; 120-129; 130-139; and ≥140 mmHg. SBP trajectories were classified into decreasing, stable, and increasing groups. Primary outcome was composite kidney outcome of ≥50% decrease in eGFR or death-censored graft loss. Compared with the 110-119 mmHg group, both the lowest (adjusted hazard ratio [aHR], 2.43) and the highest SBP (aHR, 2.25) were associated with a higher risk of composite kidney outcome. In time-varying model, also the lowest (aHR, 3.02) and the highest SBP (aHR, 3.60) were associated with a higher risk. In the trajectory model, an increasing SBP trajectory was associated with a higher risk than a stable SBP trajectory (aHR, 2.26). This associations were consistent in the validation set. In conclusion, SBP ≥140 mmHg and an increasing SBP trajectory were associated with a higher risk of allograft dysfunction and failure in KT patients.
期刊介绍:
The aim of the journal is to serve as a forum for the exchange of scientific information in the form of original and high quality papers in the field of transplantation. Clinical and experimental studies, as well as editorials, letters to the editors, and, occasionally, reviews on the biology, physiology, and immunology of transplantation of tissues and organs, are published. Publishing time for the latter is approximately six months, provided major revisions are not needed. The journal is published in yearly volumes, each volume containing twelve issues. Papers submitted to the journal are subject to peer review.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
