{"title":"意义不明的单克隆性腺病引起的弥漫性平面黄瘤病。","authors":"Marisa Lenga, Jennifer Nam Choi","doi":"10.1111/1346-8138.17432","DOIUrl":null,"url":null,"abstract":"<p>A woman in her 60s presented to the clinic for progressively accumulating, asymptomatic, yellow plaques for 6 years. Her medical history included monoclonal gammopathy of undetermined significance (MGUS) of IgG lambda light chain subtype for 6 years and hypercholesteremia. On physical examination, well-defined, thin, yellow plaques were located on the eyelids, upper chest, anterior upper arms, axillae, and antecubital fossae without mucosal lesions (Figure 1). Histopathological examination revealed scattered collections of foamy histiocytes in the superficial and midreticular dermis with mild perivascular lymphohistiocytic infiltrate. Lipid panel findings demonstrated a mildly elevated low-density lipoprotein cholesterol at 122 mg/dL (reference < 100 mg/dL). The patient was diagnosed with diffuse planar xanthomatosis in the setting of MGUS. Because the patient did not require treatment for MGUS at the time, skin-directed treatment options were reviewed with the patient, and she elected to treat the left anterior arm with cryotherapy. She was lost to follow-up.</p><p>Diffuse planar xanthomatosis is characterized by the dispersed accumulation of cholesterol-rich material in the skin and can develop in patients either with familial hyperlipidemia or with normal and slightly elevated lipids without family history.<span><sup>1, 2</sup></span> In normolipidemic patients, there is a described phenomenon of diffuse xanthomas forming in the setting of hematological or lymphoproliferative disorders.<span><sup>1</sup></span> Xanthomas form in the setting of MGUS (most commonly the IgG kappa subtype) through the creation of monoclonal IgG and low-density lipoprotein complexes and the subsequent phagocytosis of these complexes by macrophages.<span><sup>3</sup></span> This disease presents as asymptomatic, symmetric, yellow to orange plaques most commonly on the eyelids, neck, upper trunk, and flexural folds.<span><sup>4</sup></span> Histopathologic examination demonstrates diffuse foamy cells in the dermis with variable numbers of giant cells, lymphocytes, and foamy histiocytes.<span><sup>4</sup></span> Xanthomatosis may resolve spontaneously, with the treatment of MGUS, or with intervention like excision, chemabrasion, ablative laser, and cryotherapy.<span><sup>3, 4</sup></span></p><p>This case serves as representative examination findings to improve clinical recognition of diffuse xanthomatosis in the setting of MGUS.</p><p>The authors declare no conflicts of interest for this article.</p>","PeriodicalId":54848,"journal":{"name":"Journal of Dermatology","volume":"51 10","pages":"e327-e328"},"PeriodicalIF":2.7000,"publicationDate":"2024-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1346-8138.17432","citationCount":"0","resultStr":"{\"title\":\"Diffuse planar xanthomatosis in the setting of monoclonal gammopathy of undetermined significance\",\"authors\":\"Marisa Lenga, Jennifer Nam Choi\",\"doi\":\"10.1111/1346-8138.17432\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A woman in her 60s presented to the clinic for progressively accumulating, asymptomatic, yellow plaques for 6 years. Her medical history included monoclonal gammopathy of undetermined significance (MGUS) of IgG lambda light chain subtype for 6 years and hypercholesteremia. On physical examination, well-defined, thin, yellow plaques were located on the eyelids, upper chest, anterior upper arms, axillae, and antecubital fossae without mucosal lesions (Figure 1). Histopathological examination revealed scattered collections of foamy histiocytes in the superficial and midreticular dermis with mild perivascular lymphohistiocytic infiltrate. Lipid panel findings demonstrated a mildly elevated low-density lipoprotein cholesterol at 122 mg/dL (reference < 100 mg/dL). The patient was diagnosed with diffuse planar xanthomatosis in the setting of MGUS. Because the patient did not require treatment for MGUS at the time, skin-directed treatment options were reviewed with the patient, and she elected to treat the left anterior arm with cryotherapy. She was lost to follow-up.</p><p>Diffuse planar xanthomatosis is characterized by the dispersed accumulation of cholesterol-rich material in the skin and can develop in patients either with familial hyperlipidemia or with normal and slightly elevated lipids without family history.<span><sup>1, 2</sup></span> In normolipidemic patients, there is a described phenomenon of diffuse xanthomas forming in the setting of hematological or lymphoproliferative disorders.<span><sup>1</sup></span> Xanthomas form in the setting of MGUS (most commonly the IgG kappa subtype) through the creation of monoclonal IgG and low-density lipoprotein complexes and the subsequent phagocytosis of these complexes by macrophages.<span><sup>3</sup></span> This disease presents as asymptomatic, symmetric, yellow to orange plaques most commonly on the eyelids, neck, upper trunk, and flexural folds.<span><sup>4</sup></span> Histopathologic examination demonstrates diffuse foamy cells in the dermis with variable numbers of giant cells, lymphocytes, and foamy histiocytes.<span><sup>4</sup></span> Xanthomatosis may resolve spontaneously, with the treatment of MGUS, or with intervention like excision, chemabrasion, ablative laser, and cryotherapy.<span><sup>3, 4</sup></span></p><p>This case serves as representative examination findings to improve clinical recognition of diffuse xanthomatosis in the setting of MGUS.</p><p>The authors declare no conflicts of interest for this article.</p>\",\"PeriodicalId\":54848,\"journal\":{\"name\":\"Journal of Dermatology\",\"volume\":\"51 10\",\"pages\":\"e327-e328\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1346-8138.17432\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Dermatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/1346-8138.17432\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Dermatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1346-8138.17432","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Diffuse planar xanthomatosis in the setting of monoclonal gammopathy of undetermined significance
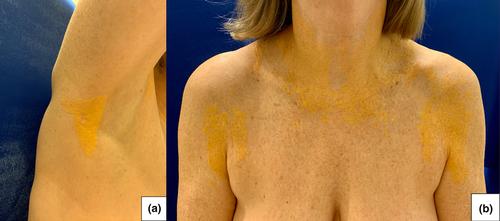
A woman in her 60s presented to the clinic for progressively accumulating, asymptomatic, yellow plaques for 6 years. Her medical history included monoclonal gammopathy of undetermined significance (MGUS) of IgG lambda light chain subtype for 6 years and hypercholesteremia. On physical examination, well-defined, thin, yellow plaques were located on the eyelids, upper chest, anterior upper arms, axillae, and antecubital fossae without mucosal lesions (Figure 1). Histopathological examination revealed scattered collections of foamy histiocytes in the superficial and midreticular dermis with mild perivascular lymphohistiocytic infiltrate. Lipid panel findings demonstrated a mildly elevated low-density lipoprotein cholesterol at 122 mg/dL (reference < 100 mg/dL). The patient was diagnosed with diffuse planar xanthomatosis in the setting of MGUS. Because the patient did not require treatment for MGUS at the time, skin-directed treatment options were reviewed with the patient, and she elected to treat the left anterior arm with cryotherapy. She was lost to follow-up.
Diffuse planar xanthomatosis is characterized by the dispersed accumulation of cholesterol-rich material in the skin and can develop in patients either with familial hyperlipidemia or with normal and slightly elevated lipids without family history.1, 2 In normolipidemic patients, there is a described phenomenon of diffuse xanthomas forming in the setting of hematological or lymphoproliferative disorders.1 Xanthomas form in the setting of MGUS (most commonly the IgG kappa subtype) through the creation of monoclonal IgG and low-density lipoprotein complexes and the subsequent phagocytosis of these complexes by macrophages.3 This disease presents as asymptomatic, symmetric, yellow to orange plaques most commonly on the eyelids, neck, upper trunk, and flexural folds.4 Histopathologic examination demonstrates diffuse foamy cells in the dermis with variable numbers of giant cells, lymphocytes, and foamy histiocytes.4 Xanthomatosis may resolve spontaneously, with the treatment of MGUS, or with intervention like excision, chemabrasion, ablative laser, and cryotherapy.3, 4
This case serves as representative examination findings to improve clinical recognition of diffuse xanthomatosis in the setting of MGUS.
The authors declare no conflicts of interest for this article.
期刊介绍:
The Journal of Dermatology is the official peer-reviewed publication of the Japanese Dermatological Association and the Asian Dermatological Association. The journal aims to provide a forum for the exchange of information about new and significant research in dermatology and to promote the discipline of dermatology in Japan and throughout the world. Research articles are supplemented by reviews, theoretical articles, special features, commentaries, book reviews and proceedings of workshops and conferences.
Preliminary or short reports and letters to the editor of two printed pages or less will be published as soon as possible. Papers in all fields of dermatology will be considered.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
