Patrick Heindel, James J Fitzgibbon, Eric Secemsky, Deepak L Bhatt, Mohammed Al-Omran, Subodh Verma, Ibrahim A Almaghlouth, Arin Madenci, Mohamad A Hussain
{"title":"秋水仙碱用于降低患有外周动脉疾病的医疗保险受益人的心血管和肢体风险:仿效目标试验。","authors":"Patrick Heindel, James J Fitzgibbon, Eric Secemsky, Deepak L Bhatt, Mohammed Al-Omran, Subodh Verma, Ibrahim A Almaghlouth, Arin Madenci, Mohamad A Hussain","doi":"10.1093/ehjopen/oeae062","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Recent evidence from randomized trials demonstrates that colchicine can reduce the risk of major adverse cardiovascular events (MACE) in patients with coronary artery disease. Colchicine's effect on lower-extremity peripheral artery disease (PAD) is not known.</p><p><strong>Methods and results: </strong>To make inferences about the real-world effectiveness of colchicine in PAD, we emulated two target trials leveraging the variable prescribing practice of adding colchicine vs. a non-steroidal anti-inflammatory drug (NSAID) to urate-lowering therapy in patients with gout and PAD. Emulated Trial 1 compared colchicine initiators with NSAID initiators. Emulated Trial 2 compared long-term (indefinite) and short-term (3 months) treatment strategies after initiating colchicine. Eligible individuals were those continuously enrolled in Medicare receiving care at a multicentre academic health system between July 2007 and December 2019. The primary outcome for both trials was a 2 year composite of major adverse limb events (MALE), MACE, and all-cause mortality. Secondary outcomes included MALE and death, MACE and death, and individual components of the primary outcome. Inverse probability weighting was used to adjust for confounding. Percentile-based 95% confidence intervals (CIs) were estimated using non-parametric bootstrapping. A total of 1820 eligible patients were included; the mean age was 77 years [standard deviation (SD) 7], 32% were female, and 9% were non-White. The mean (SD) duration of colchicine and NSAID therapy was 247 (345) and 137 (237) days, respectively. In the emulation of Trial 1, the risk of the primary composite outcome of MALE, MACE, and death at 2 years was 29.9% (95% CI 27.2%, 32.3%) in the colchicine group and 31.5% (28.3%, 34.6%) in the NSAID group, with a risk difference of -1.7% (95% CI -6.5%, 3.1%) and a risk ratio of 0.95 (95% CI 0.83, 1.07). Similar findings were noted in the emulation of Trial 2, with a risk of the primary composite outcome at 2 years of 30.7% (95% CI 23.7%, 38.1%) in the long-term colchicine group and 33.4% (95% CI 29.4%, 37.7%) in the short-term group, with a risk difference of -2.7% (95% CI -10.3%, 5.4%) and risk ratio of 0.92 (95% CI 0.70, 1.16).</p><p><strong>Conclusion: </strong>In a real-world sample of patients with PAD and gout, estimates of the effect of colchicine were consistent across two analyses and provided no conclusive evidence that colchicine decreased the risk of adverse cardiovascular or limb events and death. The cardiovascular and limb benefits of colchicine in older, comorbid populations with PAD and advanced systematic atherosclerosis remain uncertain.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 4","pages":"oeae062"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339712/pdf/","citationCount":"0","resultStr":"{\"title\":\"Colchicine for cardiovascular and limb risk reduction in Medicare beneficiaries with peripheral artery disease: emulation of target trials.\",\"authors\":\"Patrick Heindel, James J Fitzgibbon, Eric Secemsky, Deepak L Bhatt, Mohammed Al-Omran, Subodh Verma, Ibrahim A Almaghlouth, Arin Madenci, Mohamad A Hussain\",\"doi\":\"10.1093/ehjopen/oeae062\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Recent evidence from randomized trials demonstrates that colchicine can reduce the risk of major adverse cardiovascular events (MACE) in patients with coronary artery disease. Colchicine's effect on lower-extremity peripheral artery disease (PAD) is not known.</p><p><strong>Methods and results: </strong>To make inferences about the real-world effectiveness of colchicine in PAD, we emulated two target trials leveraging the variable prescribing practice of adding colchicine vs. a non-steroidal anti-inflammatory drug (NSAID) to urate-lowering therapy in patients with gout and PAD. Emulated Trial 1 compared colchicine initiators with NSAID initiators. Emulated Trial 2 compared long-term (indefinite) and short-term (3 months) treatment strategies after initiating colchicine. Eligible individuals were those continuously enrolled in Medicare receiving care at a multicentre academic health system between July 2007 and December 2019. The primary outcome for both trials was a 2 year composite of major adverse limb events (MALE), MACE, and all-cause mortality. Secondary outcomes included MALE and death, MACE and death, and individual components of the primary outcome. Inverse probability weighting was used to adjust for confounding. Percentile-based 95% confidence intervals (CIs) were estimated using non-parametric bootstrapping. A total of 1820 eligible patients were included; the mean age was 77 years [standard deviation (SD) 7], 32% were female, and 9% were non-White. The mean (SD) duration of colchicine and NSAID therapy was 247 (345) and 137 (237) days, respectively. In the emulation of Trial 1, the risk of the primary composite outcome of MALE, MACE, and death at 2 years was 29.9% (95% CI 27.2%, 32.3%) in the colchicine group and 31.5% (28.3%, 34.6%) in the NSAID group, with a risk difference of -1.7% (95% CI -6.5%, 3.1%) and a risk ratio of 0.95 (95% CI 0.83, 1.07). Similar findings were noted in the emulation of Trial 2, with a risk of the primary composite outcome at 2 years of 30.7% (95% CI 23.7%, 38.1%) in the long-term colchicine group and 33.4% (95% CI 29.4%, 37.7%) in the short-term group, with a risk difference of -2.7% (95% CI -10.3%, 5.4%) and risk ratio of 0.92 (95% CI 0.70, 1.16).</p><p><strong>Conclusion: </strong>In a real-world sample of patients with PAD and gout, estimates of the effect of colchicine were consistent across two analyses and provided no conclusive evidence that colchicine decreased the risk of adverse cardiovascular or limb events and death. The cardiovascular and limb benefits of colchicine in older, comorbid populations with PAD and advanced systematic atherosclerosis remain uncertain.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"4 4\",\"pages\":\"oeae062\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339712/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeae062\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:随机试验的最新证据表明,秋水仙碱可降低冠心病患者发生主要不良心血管事件(MACE)的风险。秋水仙碱对下肢外周动脉疾病(PAD)的影响尚不清楚:为了推断秋水仙碱对 PAD 的实际疗效,我们模拟了两项目标试验,利用痛风和 PAD 患者在降尿酸治疗中添加秋水仙碱与非类固醇消炎药 (NSAID) 的不同处方做法。仿真试验 1 对开始使用秋水仙碱的患者和开始使用非甾体抗炎药的患者进行了比较。仿真试验 2 比较了开始使用秋水仙碱后的长期(无限期)和短期(3 个月)治疗策略。符合条件的患者是在2007年7月至2019年12月期间连续参加医疗保险并在多中心学术医疗系统接受治疗的患者。两项试验的主要结果均为两年内肢体主要不良事件(MALE)、MACE和全因死亡率的复合结果。次要结果包括肢体主要不良事件和死亡、肢体主要不良事件和死亡以及主要结果的各个组成部分。采用反概率加权法调整混杂因素。采用非参数引导法估算基于百分位数的 95% 置信区间 (CI)。共纳入了 1820 名符合条件的患者;平均年龄为 77 岁[标准差(SD)为 7],32% 为女性,9% 为非白人。秋水仙碱和非甾体抗炎药的平均(标准差)治疗时间分别为 247 天(345 天)和 137 天(237 天)。在仿真试验 1 中,秋水仙碱组 2 年后出现 MALE、MACE 和死亡的主要复合结局的风险为 29.9% (95% CI 27.2%, 32.3%),NSAID 组为 31.5% (28.3%, 34.6%),风险差异为-1.7% (95% CI -6.5%, 3.1%),风险比为 0.95 (95% CI 0.83, 1.07)。试验2的模拟研究也发现了类似的结果,2年后,长期服用秋水仙碱组的主要综合结果风险为30.7%(95% CI 23.7%,38.1%),短期服用秋水仙碱组的主要综合结果风险为33.4%(95% CI 29.4%,37.7%),风险差异为-2.7%(95% CI -10.3%,5.4%),风险比为0.92(95% CI 0.70,1.16):在PAD和痛风患者的真实世界样本中,两次分析对秋水仙碱效果的估计是一致的,并没有提供秋水仙碱能降低不良心血管或肢体事件和死亡风险的确凿证据。在患有 PAD 和晚期系统性动脉粥样硬化的老年合并人群中,秋水仙碱对心血管和肢体的益处仍不确定。
Colchicine for cardiovascular and limb risk reduction in Medicare beneficiaries with peripheral artery disease: emulation of target trials.
Aims: Recent evidence from randomized trials demonstrates that colchicine can reduce the risk of major adverse cardiovascular events (MACE) in patients with coronary artery disease. Colchicine's effect on lower-extremity peripheral artery disease (PAD) is not known.
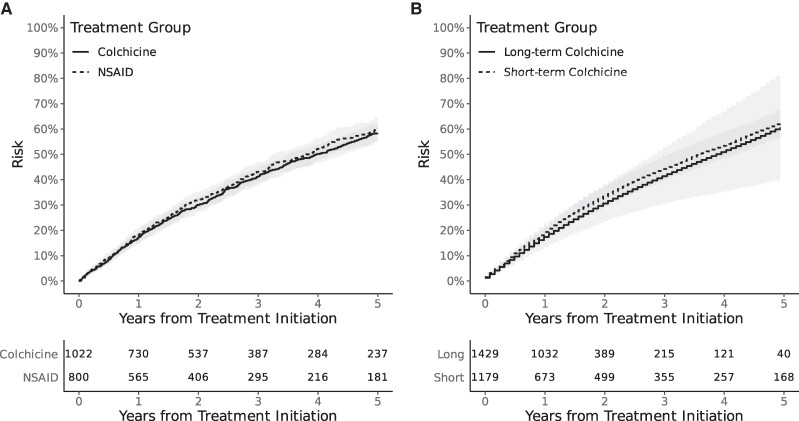
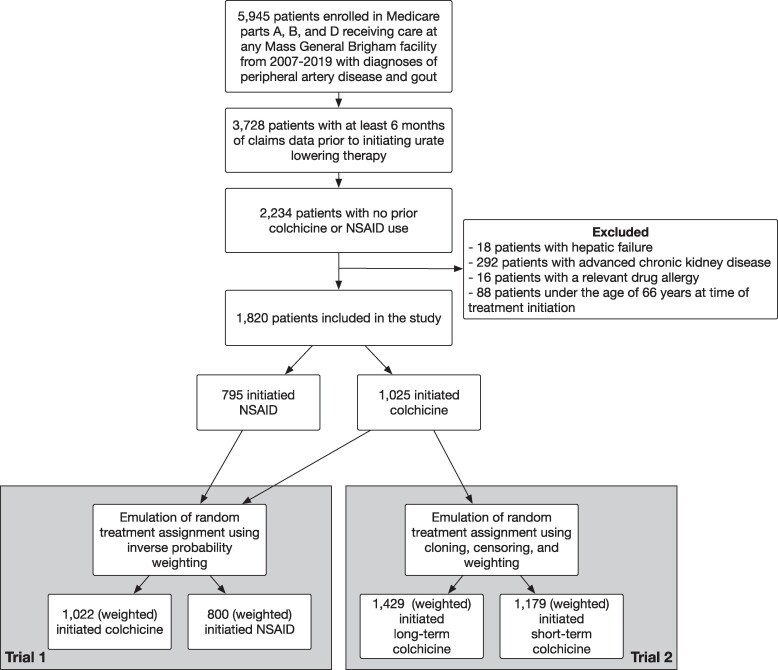
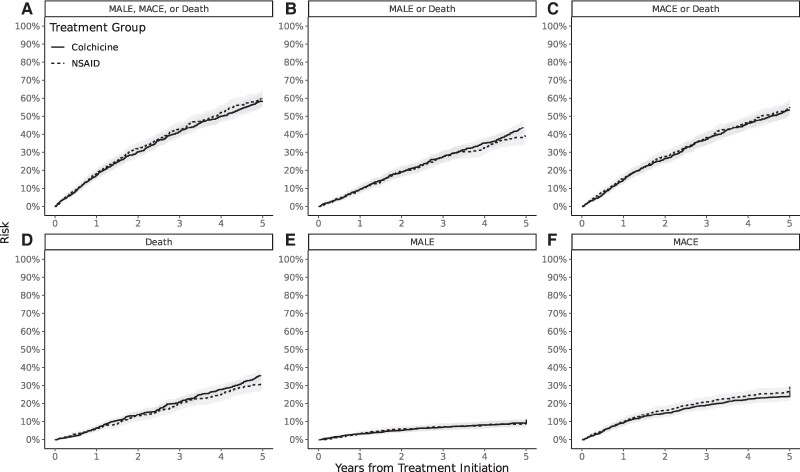
Methods and results: To make inferences about the real-world effectiveness of colchicine in PAD, we emulated two target trials leveraging the variable prescribing practice of adding colchicine vs. a non-steroidal anti-inflammatory drug (NSAID) to urate-lowering therapy in patients with gout and PAD. Emulated Trial 1 compared colchicine initiators with NSAID initiators. Emulated Trial 2 compared long-term (indefinite) and short-term (3 months) treatment strategies after initiating colchicine. Eligible individuals were those continuously enrolled in Medicare receiving care at a multicentre academic health system between July 2007 and December 2019. The primary outcome for both trials was a 2 year composite of major adverse limb events (MALE), MACE, and all-cause mortality. Secondary outcomes included MALE and death, MACE and death, and individual components of the primary outcome. Inverse probability weighting was used to adjust for confounding. Percentile-based 95% confidence intervals (CIs) were estimated using non-parametric bootstrapping. A total of 1820 eligible patients were included; the mean age was 77 years [standard deviation (SD) 7], 32% were female, and 9% were non-White. The mean (SD) duration of colchicine and NSAID therapy was 247 (345) and 137 (237) days, respectively. In the emulation of Trial 1, the risk of the primary composite outcome of MALE, MACE, and death at 2 years was 29.9% (95% CI 27.2%, 32.3%) in the colchicine group and 31.5% (28.3%, 34.6%) in the NSAID group, with a risk difference of -1.7% (95% CI -6.5%, 3.1%) and a risk ratio of 0.95 (95% CI 0.83, 1.07). Similar findings were noted in the emulation of Trial 2, with a risk of the primary composite outcome at 2 years of 30.7% (95% CI 23.7%, 38.1%) in the long-term colchicine group and 33.4% (95% CI 29.4%, 37.7%) in the short-term group, with a risk difference of -2.7% (95% CI -10.3%, 5.4%) and risk ratio of 0.92 (95% CI 0.70, 1.16).
Conclusion: In a real-world sample of patients with PAD and gout, estimates of the effect of colchicine were consistent across two analyses and provided no conclusive evidence that colchicine decreased the risk of adverse cardiovascular or limb events and death. The cardiovascular and limb benefits of colchicine in older, comorbid populations with PAD and advanced systematic atherosclerosis remain uncertain.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
