{"title":"比较双门和单门内窥镜减压术治疗颈椎根性病变的临床效果和并发症:系统回顾和荟萃分析。","authors":"Jun Li, Ting Zhang","doi":"10.52312/jdrs.2024.1820","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aimed to compare the clinical efficacy and complication rates of decompression with unilateral biportal endoscopy (UBE) and percutaneous endoscopy (PE) in cervical spondylotic radiculopathy (CSR).</p><p><strong>Materials and methods: </strong>A comprehensive literature review was conducted up to April 2024 across multiple databases, including EMBASE, PubMed, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Data, focusing on clinical studies that compare UBE with PE for posterior foraminotomy and discectomy decompression in CSR. The meta-analysis was performed with an emphasis on evaluating clinical outcomes such as operation time, blood loss, incision length, Neck Disability Index (NDI), Visual Analog Scale (VAS) for neck pain and arm pain, and complications.</p><p><strong>Results: </strong>Out of an initial 1,041 studies identified from electronic databases, eight were deemed eligible based on title, abstract, and full-text screening. These studies involved 552 patients (269 males, 283 females; mean age: 53.9±11.4 years; range, 30 to 79 years), with 287 in the UBE group and 265 in the PE group. Meta-analysis indicated no significant difference in operation time between UBE and PE (mean difference [MD]=-3.68; 95% confidence interval [CI]:-19.38, 12.02; p=0.65). However, both blood loss (MD=17.01; 95% CI: 2.61, 31.41; p=0.02) and incision length (MD=11.62; 95% CI: 9.23, 14.01; p<0.00001) were significantly lower in the PE group compared to the UBE group. Regarding clinical outcomes, no significant differences were observed between the two groups in terms of NDI (MD=0.12; 95% CI:-0.10, 0.34; 0.28), VAS for neck pain (MD=-0.06; 95% CI:-0.19, 0.06; p=0.32), VAS for arm pain (MD=-0.14; 95% CI:-0.26, -0.01; p=0.84), or complications (OR=1.07; 95% CI: 0.54, 2.10; p=0.85).</p><p><strong>Conclusion: </strong>Our findings suggest that there are no significant disparities in clinical outcomes between UBE and PE, encompassing NDI, VAS for arm pain, and VAS for neck pain, as well as complication rates. Notably, compared to PE, UBE results in increased bleeding and longer incision lengths when treating CSR, without substantially reducing operation time.</p>","PeriodicalId":73560,"journal":{"name":"Joint diseases and related surgery","volume":"35 3","pages":"583-593"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411877/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of clinical outcomes and complications of biportal and uniportal endoscopic decompression for the treatment of cervical spondylotic radiculopathy: A systematic review and meta-analysis.\",\"authors\":\"Jun Li, Ting Zhang\",\"doi\":\"10.52312/jdrs.2024.1820\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This study aimed to compare the clinical efficacy and complication rates of decompression with unilateral biportal endoscopy (UBE) and percutaneous endoscopy (PE) in cervical spondylotic radiculopathy (CSR).</p><p><strong>Materials and methods: </strong>A comprehensive literature review was conducted up to April 2024 across multiple databases, including EMBASE, PubMed, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Data, focusing on clinical studies that compare UBE with PE for posterior foraminotomy and discectomy decompression in CSR. The meta-analysis was performed with an emphasis on evaluating clinical outcomes such as operation time, blood loss, incision length, Neck Disability Index (NDI), Visual Analog Scale (VAS) for neck pain and arm pain, and complications.</p><p><strong>Results: </strong>Out of an initial 1,041 studies identified from electronic databases, eight were deemed eligible based on title, abstract, and full-text screening. These studies involved 552 patients (269 males, 283 females; mean age: 53.9±11.4 years; range, 30 to 79 years), with 287 in the UBE group and 265 in the PE group. Meta-analysis indicated no significant difference in operation time between UBE and PE (mean difference [MD]=-3.68; 95% confidence interval [CI]:-19.38, 12.02; p=0.65). However, both blood loss (MD=17.01; 95% CI: 2.61, 31.41; p=0.02) and incision length (MD=11.62; 95% CI: 9.23, 14.01; p<0.00001) were significantly lower in the PE group compared to the UBE group. Regarding clinical outcomes, no significant differences were observed between the two groups in terms of NDI (MD=0.12; 95% CI:-0.10, 0.34; 0.28), VAS for neck pain (MD=-0.06; 95% CI:-0.19, 0.06; p=0.32), VAS for arm pain (MD=-0.14; 95% CI:-0.26, -0.01; p=0.84), or complications (OR=1.07; 95% CI: 0.54, 2.10; p=0.85).</p><p><strong>Conclusion: </strong>Our findings suggest that there are no significant disparities in clinical outcomes between UBE and PE, encompassing NDI, VAS for arm pain, and VAS for neck pain, as well as complication rates. Notably, compared to PE, UBE results in increased bleeding and longer incision lengths when treating CSR, without substantially reducing operation time.</p>\",\"PeriodicalId\":73560,\"journal\":{\"name\":\"Joint diseases and related surgery\",\"volume\":\"35 3\",\"pages\":\"583-593\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411877/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Joint diseases and related surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.52312/jdrs.2024.1820\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Joint diseases and related surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52312/jdrs.2024.1820","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
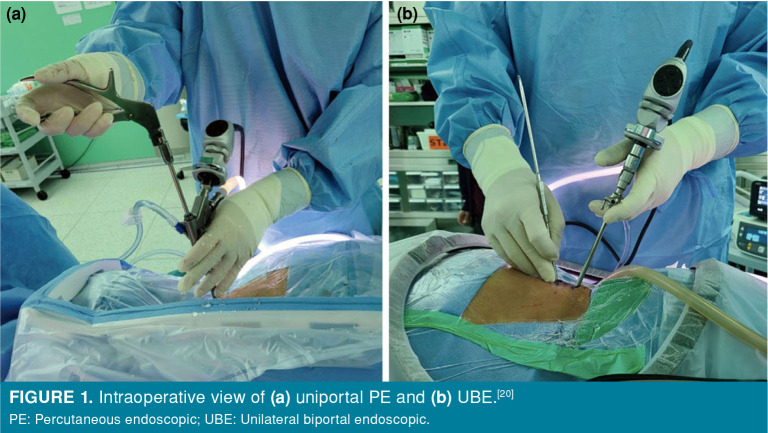
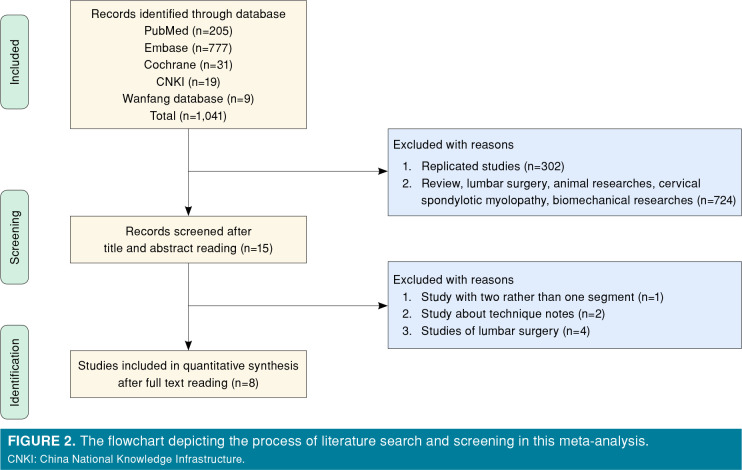
研究目的本研究旨在比较单侧双侧内镜(UBE)和经皮内镜(PE)减压治疗颈椎病(CSR)的临床疗效和并发症发生率:截至2024年4月,在EMBASE、PubMed、Cochrane图书馆、中国国家知识基础设施和万方数据等多个数据库中进行了全面的文献综述,重点关注UBE与PE在CSR后椎板切除和椎间盘切除减压术中的临床研究比较。荟萃分析的重点是评估手术时间、失血量、切口长度、颈部残疾指数(NDI)、颈部疼痛和手臂疼痛的视觉模拟量表(VAS)以及并发症等临床结果:在最初从电子数据库中找到的 1,041 项研究中,根据标题、摘要和全文筛选,有 8 项研究被认为符合条件。这些研究涉及 552 名患者(269 名男性,283 名女性;平均年龄:53.9±11.4 岁;范围:30 至 79 岁),其中 287 名患者属于 UBE 组,265 名患者属于 PE 组。Meta 分析表明,UBE 和 PE 的手术时间无显著差异(平均差异 [MD]=-3.68; 95% 置信区间 [CI]:-19.38, 12.02; p=0.65)。然而,失血量(MD=17.01;95% CI:2.61,31.41;P=0.02)和切口长度(MD=11.62;95% CI:9.23,14.01;P结论:我们的研究结果表明,UBE 和 PE 的临床疗效(包括 NDI、手臂疼痛 VAS 和颈部疼痛 VAS 以及并发症发生率)没有明显差异。值得注意的是,与 PE 相比,在治疗 CSR 时,UBE 会导致出血量增加和切口长度延长,但手术时间并未大幅缩短。
Comparison of clinical outcomes and complications of biportal and uniportal endoscopic decompression for the treatment of cervical spondylotic radiculopathy: A systematic review and meta-analysis.
Objectives: This study aimed to compare the clinical efficacy and complication rates of decompression with unilateral biportal endoscopy (UBE) and percutaneous endoscopy (PE) in cervical spondylotic radiculopathy (CSR).
Materials and methods: A comprehensive literature review was conducted up to April 2024 across multiple databases, including EMBASE, PubMed, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Data, focusing on clinical studies that compare UBE with PE for posterior foraminotomy and discectomy decompression in CSR. The meta-analysis was performed with an emphasis on evaluating clinical outcomes such as operation time, blood loss, incision length, Neck Disability Index (NDI), Visual Analog Scale (VAS) for neck pain and arm pain, and complications.
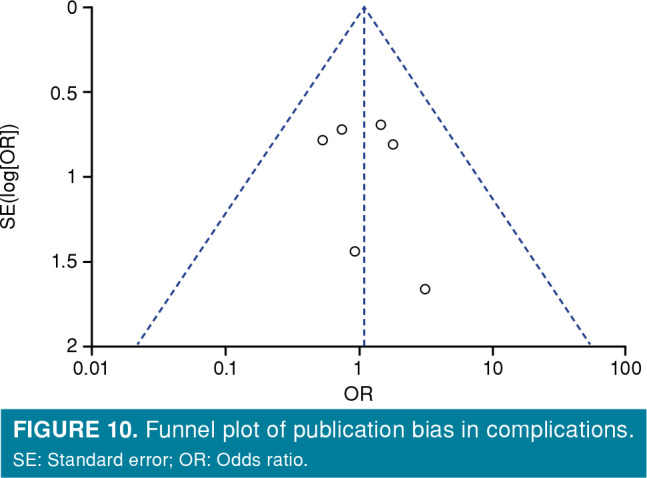
Results: Out of an initial 1,041 studies identified from electronic databases, eight were deemed eligible based on title, abstract, and full-text screening. These studies involved 552 patients (269 males, 283 females; mean age: 53.9±11.4 years; range, 30 to 79 years), with 287 in the UBE group and 265 in the PE group. Meta-analysis indicated no significant difference in operation time between UBE and PE (mean difference [MD]=-3.68; 95% confidence interval [CI]:-19.38, 12.02; p=0.65). However, both blood loss (MD=17.01; 95% CI: 2.61, 31.41; p=0.02) and incision length (MD=11.62; 95% CI: 9.23, 14.01; p<0.00001) were significantly lower in the PE group compared to the UBE group. Regarding clinical outcomes, no significant differences were observed between the two groups in terms of NDI (MD=0.12; 95% CI:-0.10, 0.34; 0.28), VAS for neck pain (MD=-0.06; 95% CI:-0.19, 0.06; p=0.32), VAS for arm pain (MD=-0.14; 95% CI:-0.26, -0.01; p=0.84), or complications (OR=1.07; 95% CI: 0.54, 2.10; p=0.85).
Conclusion: Our findings suggest that there are no significant disparities in clinical outcomes between UBE and PE, encompassing NDI, VAS for arm pain, and VAS for neck pain, as well as complication rates. Notably, compared to PE, UBE results in increased bleeding and longer incision lengths when treating CSR, without substantially reducing operation time.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
