Mohamed Elshawy MD, David Liska MD, FACS, Joshua Sommovilla MD, Sami Judeeba MD
{"title":"通过经肛门内窥镜辅助缝合隔膜切除术处理回肠J袋桥。","authors":"Mohamed Elshawy MD, David Liska MD, FACS, Joshua Sommovilla MD, Sami Judeeba MD","doi":"10.1111/ans.19222","DOIUrl":null,"url":null,"abstract":"<p>We demonstrate the technical details of transanal endoscopic assisted stapled division for a midpouch bridge diagnosed before ileostomy closure in patient with ulcerative colitis who underwent staged proctocolectomy with ileal pouch anal anastomosis (IPAA). The endoscopic assisted technique prevented pouch dysfunction following ileostomy closure with good postoperative outcomes.</p><p>A 20-year-old male with 3-years history of medically refractory ulcerative colitis presented with pancolitis underwent 3-stages proctocolectomy with IPAA and diverting loop ileostomy. Postoperative pouchoscopy revealed longitudinal bridge dividing the mid-pouch body into two compartments. A pouchogram showed no evidence of leak nor stricture, Figure 1. A third-stage procedure was scheduled, with plan to divide the bridge, followed by simultaneous ileostomy closure. The patient was placed in lithotomy position under general anaesthesia. A paediatric colonoscope was introduced transanally and 1.5 cm bridge along the longitudinal axis of the pouch was identified. We fixed the scope in retroflexed position then introduced powered stapler with reinforced and articulating Tri-Staple™ 2.0, 30 mm in length transanally, Figure 2. The stapler was directed under endoscopic guidance, and we used one firing to complete transaction of the pouch bridge. Two endoscopic clips were used to control staple line bleeding, Figure 3. After successful division of the midpouch bridge, sutured closure of the loop ileostomy was performed. The patient tolerated the procedure well with an uneventful recovery. Follow-up visits showed no evidence of anal dysfunction, urgency, seepage, or faecal incontinence. The patient reported no social limitations due to bowel function imperfections.</p><p>To date, few reports in English literature document management of Apical pouch bridge (APB).<span><sup>1-3</sup></span> APB syndrome is a structural complication with symptoms related to outlet obstruction, presenting up to 2.5 years after IPAA procedure, including difficulty in evacuation, tenesmus, anal bleeding, and perianal soreness. The original technique of the J-pouch, through creating enterotomies in the midportion of both ileal limbs then firing GIA stapler towards the apex and base of J-pouch, can leave approximately 1 cm length bridge of tissue near the apex of the pouch.<span><sup>3</sup></span> Oresland <i>et al</i>.<span><sup>1</sup></span> reported six of 100 J-pouch patients who experienced evacuation difficulties, with or without anal bleeding more than 6 months after pouch surgery. The bridge of the J-pouch was identified during anal examination and symptoms improved after severing the bridge by transanal division.<span><sup>3</sup></span> Furthermore, inflammatory processes contribute to the development of pouch mucosal bridge that was not present during pouch construction.<span><sup>2</sup></span> In the present case, we created the J-shaped ileal pouch through enterotomies at the apex of the ileal limbs ensuring there is no residual mucosal septum at time of pouch construction. Since the patient was diverted, he did not report functional or outlet obstruction symptoms. Evaluation of the pouch prior to ileostomy reversal is crucial to diagnose the pouch bridge. To our knowledge, this is the first report to demonstrate endoscopy-assisted transanal division of the midpouch bridge at time of ileostomy closure, preventing a decline in pouch function and quality of life after surgery.</p><p>Written informed consent was obtained from the patient for the publication.</p><p><b>Mohamed Elshawy:</b> Formal analysis; investigation; methodology; writing – original draft. <b>David Liska:</b> Conceptualization; formal analysis; methodology; supervision. <b>Joshua Sommovilla:</b> Supervision. <b>Sami Judeeba:</b> Conceptualization; investigation; methodology; supervision.</p>","PeriodicalId":8158,"journal":{"name":"ANZ Journal of Surgery","volume":"94 11","pages":"2075-2076"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19222","citationCount":"0","resultStr":"{\"title\":\"Management of ileoanal J-pouch bridge by transanal endoscopic assisted stapled septotomy\",\"authors\":\"Mohamed Elshawy MD, David Liska MD, FACS, Joshua Sommovilla MD, Sami Judeeba MD\",\"doi\":\"10.1111/ans.19222\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>We demonstrate the technical details of transanal endoscopic assisted stapled division for a midpouch bridge diagnosed before ileostomy closure in patient with ulcerative colitis who underwent staged proctocolectomy with ileal pouch anal anastomosis (IPAA). The endoscopic assisted technique prevented pouch dysfunction following ileostomy closure with good postoperative outcomes.</p><p>A 20-year-old male with 3-years history of medically refractory ulcerative colitis presented with pancolitis underwent 3-stages proctocolectomy with IPAA and diverting loop ileostomy. Postoperative pouchoscopy revealed longitudinal bridge dividing the mid-pouch body into two compartments. A pouchogram showed no evidence of leak nor stricture, Figure 1. A third-stage procedure was scheduled, with plan to divide the bridge, followed by simultaneous ileostomy closure. The patient was placed in lithotomy position under general anaesthesia. A paediatric colonoscope was introduced transanally and 1.5 cm bridge along the longitudinal axis of the pouch was identified. We fixed the scope in retroflexed position then introduced powered stapler with reinforced and articulating Tri-Staple™ 2.0, 30 mm in length transanally, Figure 2. The stapler was directed under endoscopic guidance, and we used one firing to complete transaction of the pouch bridge. Two endoscopic clips were used to control staple line bleeding, Figure 3. After successful division of the midpouch bridge, sutured closure of the loop ileostomy was performed. The patient tolerated the procedure well with an uneventful recovery. Follow-up visits showed no evidence of anal dysfunction, urgency, seepage, or faecal incontinence. The patient reported no social limitations due to bowel function imperfections.</p><p>To date, few reports in English literature document management of Apical pouch bridge (APB).<span><sup>1-3</sup></span> APB syndrome is a structural complication with symptoms related to outlet obstruction, presenting up to 2.5 years after IPAA procedure, including difficulty in evacuation, tenesmus, anal bleeding, and perianal soreness. The original technique of the J-pouch, through creating enterotomies in the midportion of both ileal limbs then firing GIA stapler towards the apex and base of J-pouch, can leave approximately 1 cm length bridge of tissue near the apex of the pouch.<span><sup>3</sup></span> Oresland <i>et al</i>.<span><sup>1</sup></span> reported six of 100 J-pouch patients who experienced evacuation difficulties, with or without anal bleeding more than 6 months after pouch surgery. The bridge of the J-pouch was identified during anal examination and symptoms improved after severing the bridge by transanal division.<span><sup>3</sup></span> Furthermore, inflammatory processes contribute to the development of pouch mucosal bridge that was not present during pouch construction.<span><sup>2</sup></span> In the present case, we created the J-shaped ileal pouch through enterotomies at the apex of the ileal limbs ensuring there is no residual mucosal septum at time of pouch construction. Since the patient was diverted, he did not report functional or outlet obstruction symptoms. Evaluation of the pouch prior to ileostomy reversal is crucial to diagnose the pouch bridge. To our knowledge, this is the first report to demonstrate endoscopy-assisted transanal division of the midpouch bridge at time of ileostomy closure, preventing a decline in pouch function and quality of life after surgery.</p><p>Written informed consent was obtained from the patient for the publication.</p><p><b>Mohamed Elshawy:</b> Formal analysis; investigation; methodology; writing – original draft. <b>David Liska:</b> Conceptualization; formal analysis; methodology; supervision. <b>Joshua Sommovilla:</b> Supervision. <b>Sami Judeeba:</b> Conceptualization; investigation; methodology; supervision.</p>\",\"PeriodicalId\":8158,\"journal\":{\"name\":\"ANZ Journal of Surgery\",\"volume\":\"94 11\",\"pages\":\"2075-2076\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19222\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ANZ Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ans.19222\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ANZ Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ans.19222","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Management of ileoanal J-pouch bridge by transanal endoscopic assisted stapled septotomy
We demonstrate the technical details of transanal endoscopic assisted stapled division for a midpouch bridge diagnosed before ileostomy closure in patient with ulcerative colitis who underwent staged proctocolectomy with ileal pouch anal anastomosis (IPAA). The endoscopic assisted technique prevented pouch dysfunction following ileostomy closure with good postoperative outcomes.
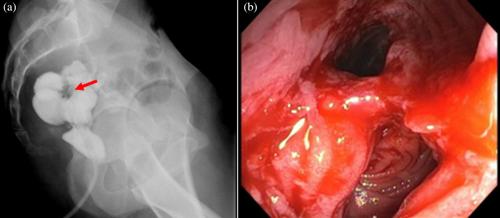
A 20-year-old male with 3-years history of medically refractory ulcerative colitis presented with pancolitis underwent 3-stages proctocolectomy with IPAA and diverting loop ileostomy. Postoperative pouchoscopy revealed longitudinal bridge dividing the mid-pouch body into two compartments. A pouchogram showed no evidence of leak nor stricture, Figure 1. A third-stage procedure was scheduled, with plan to divide the bridge, followed by simultaneous ileostomy closure. The patient was placed in lithotomy position under general anaesthesia. A paediatric colonoscope was introduced transanally and 1.5 cm bridge along the longitudinal axis of the pouch was identified. We fixed the scope in retroflexed position then introduced powered stapler with reinforced and articulating Tri-Staple™ 2.0, 30 mm in length transanally, Figure 2. The stapler was directed under endoscopic guidance, and we used one firing to complete transaction of the pouch bridge. Two endoscopic clips were used to control staple line bleeding, Figure 3. After successful division of the midpouch bridge, sutured closure of the loop ileostomy was performed. The patient tolerated the procedure well with an uneventful recovery. Follow-up visits showed no evidence of anal dysfunction, urgency, seepage, or faecal incontinence. The patient reported no social limitations due to bowel function imperfections.
To date, few reports in English literature document management of Apical pouch bridge (APB).1-3 APB syndrome is a structural complication with symptoms related to outlet obstruction, presenting up to 2.5 years after IPAA procedure, including difficulty in evacuation, tenesmus, anal bleeding, and perianal soreness. The original technique of the J-pouch, through creating enterotomies in the midportion of both ileal limbs then firing GIA stapler towards the apex and base of J-pouch, can leave approximately 1 cm length bridge of tissue near the apex of the pouch.3 Oresland et al.1 reported six of 100 J-pouch patients who experienced evacuation difficulties, with or without anal bleeding more than 6 months after pouch surgery. The bridge of the J-pouch was identified during anal examination and symptoms improved after severing the bridge by transanal division.3 Furthermore, inflammatory processes contribute to the development of pouch mucosal bridge that was not present during pouch construction.2 In the present case, we created the J-shaped ileal pouch through enterotomies at the apex of the ileal limbs ensuring there is no residual mucosal septum at time of pouch construction. Since the patient was diverted, he did not report functional or outlet obstruction symptoms. Evaluation of the pouch prior to ileostomy reversal is crucial to diagnose the pouch bridge. To our knowledge, this is the first report to demonstrate endoscopy-assisted transanal division of the midpouch bridge at time of ileostomy closure, preventing a decline in pouch function and quality of life after surgery.
Written informed consent was obtained from the patient for the publication.
Mohamed Elshawy: Formal analysis; investigation; methodology; writing – original draft. David Liska: Conceptualization; formal analysis; methodology; supervision. Joshua Sommovilla: Supervision. Sami Judeeba: Conceptualization; investigation; methodology; supervision.
期刊介绍:
ANZ Journal of Surgery is published by Wiley on behalf of the Royal Australasian College of Surgeons to provide a medium for the publication of peer-reviewed original contributions related to clinical practice and/or research in all fields of surgery and related disciplines. It also provides a programme of continuing education for surgeons. All articles are peer-reviewed by at least two researchers expert in the field of the submitted paper.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
