{"title":"基于术前、术中和术后发现的乳头状癌和滤泡状癌预后因素。","authors":"Yasuhiro Ito, Akira Miyauchi","doi":"10.1530/ETJ-24-0196","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>Papillary and follicular thyroid carcinomas (PTC and FTC) are prominent malignancies that originate from thyroid follicular cells. PTC is usually diagnosed via preoperative cytology, and large tumor size, clinical node metastasis, and distant metastasis constitute preoperative prognostic factors. Gross extrathyroidal and extranodal tumor extensions have a significant prognostic impact, are evaluated intraoperatively, and are useful for determining the extent of surgery. Aggressive variants, such as tall cell and hobnail variants, a high Ki-67 labeling index (LI), and somatic gene mutations are prognostic factors in postoperative pathological and molecular examinations. In contrast, FTC is generally diagnosed based on postoperative pathology. Large tumor size and M factors have prognostic value; however, the findings of pathological examinations are very important. FTCs are classified as minimally invasive, encapsulated angioinvasive, and widely invasive FTCs. Widely invasive FTC with vascular invasion (VI) and encapsulated angioinvasive FTCs with extensive VI have a poor prognosis, whereas widely invasive FTC without VI has an excellent prognosis, which is similar to that of minimally invasive FTC. This indicates that VI is a considerably more important prognostic marker than capsular invasion. For postoperative follow-up, dynamic markers such as the thyroglobulin-doubling rate (DR), metastatic tumor volume-DR, and change in the neutrophil-to-lymphocyte ratio are important and are useful for evaluating the effectiveness of treatments, such as radioactive iodine therapy and molecular targeted therapy, for recurrent lesions. For clinicians, it is important to accurately evaluate prognostic markers of PTC and FTC in the pre-, intra-operative, and post-operative phases.</p>","PeriodicalId":12159,"journal":{"name":"European Thyroid Journal","volume":" ","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11466271/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic factors of papillary and follicular carcinomas based on pre-, intra-, and post-operative findings.\",\"authors\":\"Yasuhiro Ito, Akira Miyauchi\",\"doi\":\"10.1530/ETJ-24-0196\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>Papillary and follicular thyroid carcinomas (PTC and FTC) are prominent malignancies that originate from thyroid follicular cells. PTC is usually diagnosed via preoperative cytology, and large tumor size, clinical node metastasis, and distant metastasis constitute preoperative prognostic factors. Gross extrathyroidal and extranodal tumor extensions have a significant prognostic impact, are evaluated intraoperatively, and are useful for determining the extent of surgery. Aggressive variants, such as tall cell and hobnail variants, a high Ki-67 labeling index (LI), and somatic gene mutations are prognostic factors in postoperative pathological and molecular examinations. In contrast, FTC is generally diagnosed based on postoperative pathology. Large tumor size and M factors have prognostic value; however, the findings of pathological examinations are very important. FTCs are classified as minimally invasive, encapsulated angioinvasive, and widely invasive FTCs. Widely invasive FTC with vascular invasion (VI) and encapsulated angioinvasive FTCs with extensive VI have a poor prognosis, whereas widely invasive FTC without VI has an excellent prognosis, which is similar to that of minimally invasive FTC. This indicates that VI is a considerably more important prognostic marker than capsular invasion. For postoperative follow-up, dynamic markers such as the thyroglobulin-doubling rate (DR), metastatic tumor volume-DR, and change in the neutrophil-to-lymphocyte ratio are important and are useful for evaluating the effectiveness of treatments, such as radioactive iodine therapy and molecular targeted therapy, for recurrent lesions. For clinicians, it is important to accurately evaluate prognostic markers of PTC and FTC in the pre-, intra-operative, and post-operative phases.</p>\",\"PeriodicalId\":12159,\"journal\":{\"name\":\"European Thyroid Journal\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11466271/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Thyroid Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1530/ETJ-24-0196\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Thyroid Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/ETJ-24-0196","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
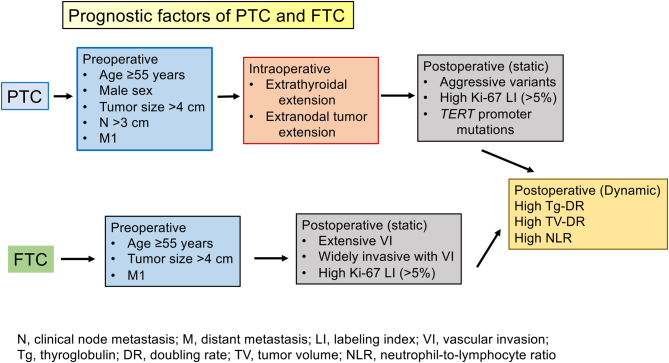
甲状腺乳头状癌和滤泡状癌(PTC和FTC)是起源于甲状腺滤泡细胞的常见恶性肿瘤。PTC通常通过术前细胞学检查确诊,肿瘤体积大、临床结节转移和远处转移是术前预后因素。甲状腺外和结节外肿瘤的粗大扩展对预后有重要影响,可在术中进行评估,并有助于确定手术范围。在术后病理和分子检查中,侵袭性变异(如高细胞和蹄甲变异)、高Ki-67标记指数(LI)和体细胞基因突变是预后因素。相比之下,FTC 一般根据术后病理诊断。肿瘤体积大和 M 因子具有预后价值,但病理检查结果非常重要。FTC 可分为微侵袭性 FTC、包裹性血管侵袭性 FTC 和广泛侵袭性 FTC。伴有血管侵犯(VI)的广泛浸润性 FTC 和伴有广泛 VI 的包裹性血管浸润性 FTC 预后较差,而不伴有 VI 的广泛浸润性 FTC 预后较好,与微创性 FTC 的预后相似。这表明,VI 是比囊肿侵犯更重要的预后指标。对于术后随访,甲状腺球蛋白倍增率(DR)、转移性肿瘤体积-DR、中性粒细胞与淋巴细胞比值变化等动态指标非常重要,有助于评估放射性碘治疗和分子靶向治疗等治疗方法对复发病灶的疗效。对于临床医生来说,在术前、术中和术后阶段准确评估 PTC 和 FTC 的预后指标非常重要。
Prognostic factors of papillary and follicular carcinomas based on pre-, intra-, and post-operative findings.
Abstract: Papillary and follicular thyroid carcinomas (PTC and FTC) are prominent malignancies that originate from thyroid follicular cells. PTC is usually diagnosed via preoperative cytology, and large tumor size, clinical node metastasis, and distant metastasis constitute preoperative prognostic factors. Gross extrathyroidal and extranodal tumor extensions have a significant prognostic impact, are evaluated intraoperatively, and are useful for determining the extent of surgery. Aggressive variants, such as tall cell and hobnail variants, a high Ki-67 labeling index (LI), and somatic gene mutations are prognostic factors in postoperative pathological and molecular examinations. In contrast, FTC is generally diagnosed based on postoperative pathology. Large tumor size and M factors have prognostic value; however, the findings of pathological examinations are very important. FTCs are classified as minimally invasive, encapsulated angioinvasive, and widely invasive FTCs. Widely invasive FTC with vascular invasion (VI) and encapsulated angioinvasive FTCs with extensive VI have a poor prognosis, whereas widely invasive FTC without VI has an excellent prognosis, which is similar to that of minimally invasive FTC. This indicates that VI is a considerably more important prognostic marker than capsular invasion. For postoperative follow-up, dynamic markers such as the thyroglobulin-doubling rate (DR), metastatic tumor volume-DR, and change in the neutrophil-to-lymphocyte ratio are important and are useful for evaluating the effectiveness of treatments, such as radioactive iodine therapy and molecular targeted therapy, for recurrent lesions. For clinicians, it is important to accurately evaluate prognostic markers of PTC and FTC in the pre-, intra-operative, and post-operative phases.
期刊介绍:
The ''European Thyroid Journal'' publishes papers reporting original research in basic, translational and clinical thyroidology. Original contributions cover all aspects of the field, from molecular and cellular biology to immunology and biochemistry, from physiology to pathology, and from pediatric to adult thyroid diseases with a special focus on thyroid cancer. Readers also benefit from reviews by noted experts, which highlight especially active areas of current research. The journal will further publish formal guidelines in the field, produced and endorsed by the European Thyroid Association.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
