Melanie M Randall, Tristen Burt, Scott Cruise, Michael K Mesisca, Thomas Minahan
{"title":"在急诊科使用腺苷治疗小儿快速性心律失常的安全性:一项为期 10 年的跨医院横断面研究。","authors":"Melanie M Randall, Tristen Burt, Scott Cruise, Michael K Mesisca, Thomas Minahan","doi":"10.1186/s12245-024-00683-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Supraventricular tachycardia is the most common dysrhythmia in children. Initial vagal maneuvers are successful less than half of the time. Adenosine, a potent AV nodal blocker with a short half-life, is recommended as first line pharmacotherapy. Minor side effects from adenosine are common, but report of serious side effects such as sustained ventricular tachycardia, torsades de pointes, syncope or hypotension are confined to small case series or studies greater than 20 years old. We aimed to specifically identify the incidence of serious side effects of adenosine in children in the emergency department.</p><p><strong>Methods: </strong>Between 2002 and 2022, all children less than 18 years old who received adenosine for tachyarrhythmia treatment in two emergency departments were included. The electronic record was reviewed for demographic information, patient history, treatments given, and side effects or complications were observed. Electrocardiograms before, during and after adenosine administration were reviewed.</p><p><strong>Results: </strong>77 patients met inclusion criteria. There were 74 patients with an initial rhythm of typical SVT. The other three patients included one with a junctional rhythm, one with atrial fibrillation, and one with an undetermined narrow complex tachycardia. 49 patients had cardiac rhythm monitoring during adenosine administration. 17 of these patients had three or more consecutive ventricular beats following adenosine, however no patients required treatment. No patients had syncope. One patient had brief hypotension after adenosine that normalized without intervention. Four patients were electrically cardioverted after adenosine, all for persistent dysrhythmias: two for persistent SVT with hypotension, one for atrial fibrillation and one for an undetermined rhythm. Twelve patients were placed on continuous antiarrhythmic medication for persistent SVT. Age, gender, prior SVT history, initial adenosine dose, and need for additional doses were not significant risk factors for a prolonged sinus pause or greater than two ventricular beats.</p><p><strong>Conclusions: </strong>Adenosine treatment in typical supraventricular tachycardia in pediatric patients is safe.</p>","PeriodicalId":13967,"journal":{"name":"International Journal of Emergency Medicine","volume":"17 1","pages":"103"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11363447/pdf/","citationCount":"0","resultStr":"{\"title\":\"Safety of adenosine for pediatric tachyarrhythmia treatment in the emergency department: a multi-hospital 10-year cross-sectional study.\",\"authors\":\"Melanie M Randall, Tristen Burt, Scott Cruise, Michael K Mesisca, Thomas Minahan\",\"doi\":\"10.1186/s12245-024-00683-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Supraventricular tachycardia is the most common dysrhythmia in children. Initial vagal maneuvers are successful less than half of the time. Adenosine, a potent AV nodal blocker with a short half-life, is recommended as first line pharmacotherapy. Minor side effects from adenosine are common, but report of serious side effects such as sustained ventricular tachycardia, torsades de pointes, syncope or hypotension are confined to small case series or studies greater than 20 years old. We aimed to specifically identify the incidence of serious side effects of adenosine in children in the emergency department.</p><p><strong>Methods: </strong>Between 2002 and 2022, all children less than 18 years old who received adenosine for tachyarrhythmia treatment in two emergency departments were included. The electronic record was reviewed for demographic information, patient history, treatments given, and side effects or complications were observed. Electrocardiograms before, during and after adenosine administration were reviewed.</p><p><strong>Results: </strong>77 patients met inclusion criteria. There were 74 patients with an initial rhythm of typical SVT. The other three patients included one with a junctional rhythm, one with atrial fibrillation, and one with an undetermined narrow complex tachycardia. 49 patients had cardiac rhythm monitoring during adenosine administration. 17 of these patients had three or more consecutive ventricular beats following adenosine, however no patients required treatment. No patients had syncope. One patient had brief hypotension after adenosine that normalized without intervention. Four patients were electrically cardioverted after adenosine, all for persistent dysrhythmias: two for persistent SVT with hypotension, one for atrial fibrillation and one for an undetermined rhythm. Twelve patients were placed on continuous antiarrhythmic medication for persistent SVT. Age, gender, prior SVT history, initial adenosine dose, and need for additional doses were not significant risk factors for a prolonged sinus pause or greater than two ventricular beats.</p><p><strong>Conclusions: </strong>Adenosine treatment in typical supraventricular tachycardia in pediatric patients is safe.</p>\",\"PeriodicalId\":13967,\"journal\":{\"name\":\"International Journal of Emergency Medicine\",\"volume\":\"17 1\",\"pages\":\"103\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11363447/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s12245-024-00683-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12245-024-00683-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Safety of adenosine for pediatric tachyarrhythmia treatment in the emergency department: a multi-hospital 10-year cross-sectional study.
Background: Supraventricular tachycardia is the most common dysrhythmia in children. Initial vagal maneuvers are successful less than half of the time. Adenosine, a potent AV nodal blocker with a short half-life, is recommended as first line pharmacotherapy. Minor side effects from adenosine are common, but report of serious side effects such as sustained ventricular tachycardia, torsades de pointes, syncope or hypotension are confined to small case series or studies greater than 20 years old. We aimed to specifically identify the incidence of serious side effects of adenosine in children in the emergency department.
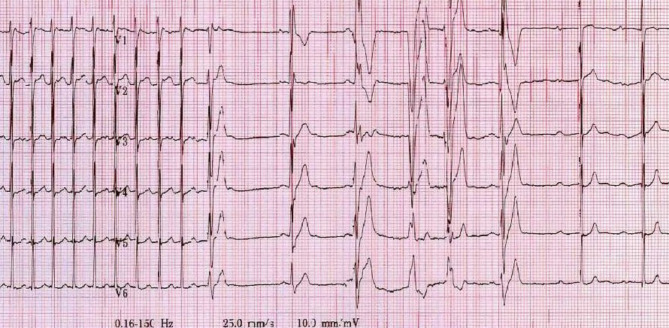
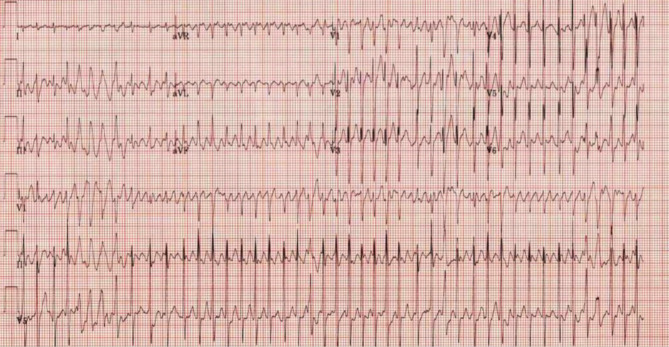
Methods: Between 2002 and 2022, all children less than 18 years old who received adenosine for tachyarrhythmia treatment in two emergency departments were included. The electronic record was reviewed for demographic information, patient history, treatments given, and side effects or complications were observed. Electrocardiograms before, during and after adenosine administration were reviewed.
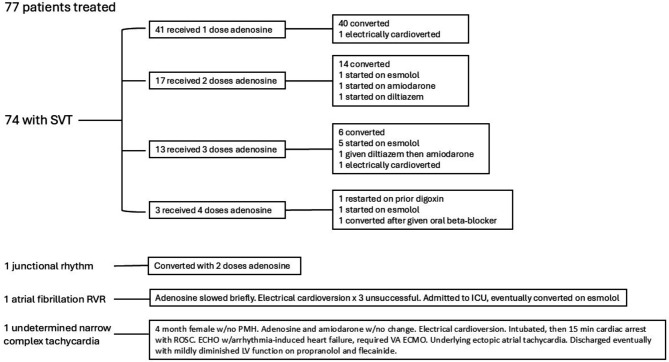
Results: 77 patients met inclusion criteria. There were 74 patients with an initial rhythm of typical SVT. The other three patients included one with a junctional rhythm, one with atrial fibrillation, and one with an undetermined narrow complex tachycardia. 49 patients had cardiac rhythm monitoring during adenosine administration. 17 of these patients had three or more consecutive ventricular beats following adenosine, however no patients required treatment. No patients had syncope. One patient had brief hypotension after adenosine that normalized without intervention. Four patients were electrically cardioverted after adenosine, all for persistent dysrhythmias: two for persistent SVT with hypotension, one for atrial fibrillation and one for an undetermined rhythm. Twelve patients were placed on continuous antiarrhythmic medication for persistent SVT. Age, gender, prior SVT history, initial adenosine dose, and need for additional doses were not significant risk factors for a prolonged sinus pause or greater than two ventricular beats.
Conclusions: Adenosine treatment in typical supraventricular tachycardia in pediatric patients is safe.
期刊介绍:
The aim of the journal is to bring to light the various clinical advancements and research developments attained over the world and thus help the specialty forge ahead. It is directed towards physicians and medical personnel undergoing training or working within the field of Emergency Medicine. Medical students who are interested in pursuing a career in Emergency Medicine will also benefit from the journal. This is particularly useful for trainees in countries where the specialty is still in its infancy. Disciplines covered will include interesting clinical cases, the latest evidence-based practice and research developments in Emergency medicine including emergency pediatrics.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
