Gary D Zhang, Daniel Johnstone, Michael F Leahy, John K Olynyk
{"title":"在澳大利亚红十字会生命之血对献血者进行常规铁蛋白检测的时代,更新铁缺乏症的诊断和管理。","authors":"Gary D Zhang, Daniel Johnstone, Michael F Leahy, John K Olynyk","doi":"10.5694/mja2.52429","DOIUrl":null,"url":null,"abstract":"<p>Iron deficiency is the most common micronutrient deficiency worldwide<span><sup>1</sup></span> and the predominant cause of anaemia, which affects one-quarter of the global population.<span><sup>2</sup></span></p><p>In Australia, 22.3% of women have depleted iron stores (serum ferritin level < 30 μg/L), with pre-menopausal women disproportionately affected.<span><sup>3</sup></span> In contrast, 3.5% of men are iron deficient.<span><sup>3</sup></span></p><p>The Australian Red Cross Lifeblood implemented routine ferritin level testing in August 2023 for new whole blood donors (105 069 in 2023),<span><sup>4</sup></span> with expanded testing to include returning blood donors in 2024.<span><sup>5</sup></span> Donors are formally advised if their ferritin result is outside the reference intervals of 15–400 μg/L for female donors and 30–500 μg/L for male donors.<span><sup>5</sup></span> This will identify a considerable number of iron deficient adults who will be directed to their primary care physician for management. In the context of this policy change and implications for primary care, this article provides a guide for investigating and managing absolute iron deficiency.</p><p>Iron stores inadequate to meet the demands of the body result in absolute iron deficiency, which is associated with a compensatory reduction in serum hepcidin concentration to stimulate an increase in gastrointestinal iron absorption and restore homeostasis.<span><sup>6-8</sup></span> Functional iron deficiency occurs when relatively normal iron stores are unable to be released for physiological requirements due to inappropriately elevated serum hepcidin levels, as may occur in chronic inflammatory conditions, including obesity, chronic disease and neoplasia.<span><sup>6-8</sup></span> Absolute and functional iron deficiency can also co-exist.<span><sup>7</sup></span> A ferritin level below the reference interval should always be interpreted as absolute iron deficiency.</p><p>The diagnosis of iron deficiency is based on routinely available blood biomarkers as described in Box 1. Serum ferritin level cut-offs to diagnose iron deficiency vary considerably,<span><sup>9</sup></span> from less than 15 μg/L used by the World Health Organization,<span><sup>10</sup></span> which predicts absent iron stores with very high specificity,<span><sup>7</sup></span> to less than 30 μg/L commonly used in Australia.<span><sup>7, 8, 11, 12</sup></span> Although the sex-based cut-offs adopted by the Australian Red Cross Lifeblood were reportedly derived from the Royal College of Pathologists of Australasia,<span><sup>12</sup></span> there is significant concern regarding inequalities using unconventional sex-based cut-offs, with underdiagnosis and undertreatment of iron deficient women. As an acute-phase reactant, ferritin may be falsely normal or elevated in iron deficient individuals when there is concurrent inflammation, obesity, steatotic liver disease, malignancy or other chronic disease.<span><sup>6, 7, 11</sup></span> Thus, a serum ferritin level less than 70 μg/L in an individual with a concurrent inflammatory condition may suggest iron deficiency.<span><sup>10</sup></span> Transferrin saturation values less than 20% indicate low serum iron bioavailability, consistent with absolute or functional iron deficiency. The mean cell volume and mean cell haemoglobin concentration are sensitive measures for iron deficiency anaemia (IDA) when B12 or folate deficiency are absent.<span><sup>6, 11</sup></span></p><p>Further assessment must be conducted to define the underlying aetiology of iron deficiency, which can be broadly categorised into physiological, inadequate intake or absorption, blood loss, and rare genetic causes (Box 2). Factors such as age, sex and ethnicity influence the probability of different aetiologies. Although physiological causes are commonly suspected in younger individuals, the incidence of pathological causes, such as colorectal malignancy, increases with age (Box 3). Risk stratification is necessary to guide appropriate investigations. A suggested approach to a low serum ferritin result is presented in Box 4.</p><p>Physiological causes of iron deficiency predominately affect pre-menopausal women, pregnant women and growing children. Menstrual blood loss contributes significantly to iron deficiency, with iron deficiency affecting around half of women with heavy menstrual bleeding.<span><sup>6-8, 11</sup></span></p><p>Iron uptake is affected by dietary intake and absorption. Haem iron is efficiently absorbed in the duodenum, whereas non-haem iron is less efficiently absorbed and influenced by dietary composition.<span><sup>13</sup></span> Several dietary factors inhibit non-haem iron absorption (Box 2).<span><sup>13</sup></span> The ingestion of ascorbic acid (vitamin C), lactic acid (found in fermented foods) and animal meat enhances the absorption of iron.<span><sup>13</sup></span> Gastric acid, which can be impaired by medications, aids in the conversion of insoluble ferric non-haem iron to the absorbable ferrous form.<span><sup>14</sup></span> Surgical resection or bypass involving the stomach or small intestine (or both) predisposes the patient to iron deficiency due to malabsorption and reduced food intake.<span><sup>15</sup></span></p><p>Coeliac disease has a global prevalence of 0.7–1.4% and accounts for about 3% of IDA in the general population.<span><sup>16</sup></span> Serological testing for coeliac disease using serum tissue transglutaminase IgA antibody levels should be undertaken for assessment of iron deficiency.<span><sup>6, 7</sup></span> In the 2–3% of coeliac patients with IgA deficiency, an IgA level or IgG-based assay, such as deamidated gliadin peptide, should be performed.<span><sup>6, 7</sup></span> Duodenal biopsies taken when the patient is on a gluten-containing diet remains the gold standard for diagnosis of coeliac disease in Australia.</p><p>Autoimmune gastritis, generally associated with pernicious anaemia, is commonly refractory to oral iron supplementation and reported in 27% of individuals with unexplained IDA.<span><sup>17</sup></span> <i>Helicobacter pylori</i> infection is associated with iron deficiency and eradication improves iron stores, especially in cases previously refractory to oral iron supplementation.<span><sup>17</sup></span></p><p>In obesity, iron deficiency can result from reduced iron absorption.<span><sup>7</sup></span></p><p>There are also rare genetic causes of unexplained iron deficiency.<span><sup>6, 7</sup></span></p><p>Blood loss is the most common and most significant pathological cause of iron deficiency, with aetiologies described in Box 2. Gastrointestinal blood loss accounts for most cases of iron deficiency,<span><sup>6, 7, 9, 11, 18</sup></span> with bidirectional endoscopic examination detecting a potential gastrointestinal bleeding cause in two-thirds of men and post-menopausal women with IDA. Bidirectional endoscopic examination should be routinely considered for all adults with iron deficiency as the technique shows a detection rate of 11% for gastrointestinal malignancy and 9% for colorectal malignancy.<span><sup>6-9</sup></span> Faecal occult blood testing is used for asymptomatic average-risk bowel cancer screening and should not guide iron deficiency investigations.<span><sup>6, 7</sup></span> Small intestine investigation, predominantly with capsule endoscopy, may be considered in recurrent or refractory IDA following unremarkable bidirectional endoscopy results.<span><sup>19</sup></span> When colonoscopy is contraindicated, computed tomography colonography can help rule out colorectal lesions larger than or equal to 6 mm, but cannot provide histopathological diagnosis.<span><sup>7, 20</sup></span> Medications can exacerbate blood loss, particularly non-steroidal anti-inflammatory drugs and anti-thrombotics.<span><sup>6-8</sup></span> Urinalysis is recommended to screen for microscopic haematuria, although this test is not sensitive for urological malignancies.<span><sup>6</sup></span> Stool investigations for intestinal parasitic infections can be done for at-risk individuals with exposure to endemic regions.<span><sup>8</sup></span> Frequent whole blood donation can result in iron deficiency.<span><sup>11</sup></span></p><p>Iron supplementation, available in oral or parenteral forms, is required for all individuals with IDA and should be started promptly to replace body iron stores and resolve symptoms. Iron replacement for non-anaemic iron deficiency improves symptoms and clinical outcomes.<span><sup>6, 7</sup></span> Iron-deplete women with serum ferritin levels of 15–30 μg/L will not be identified through the Australian Red Cross Lifeblood testing, although may benefit from iron replacement. Blood transfusion with restrictive targets should be reserved for severe symptomatic anaemia and symptoms of reduced oxygen-carrying capacity with cardiovascular compromise or ongoing blood loss, when iron replacement alone is insufficient.<span><sup>6</sup></span> Increasing dietary iron intake alone is insufficient for iron deficiency, although should be optimised for secondary prevention.</p><p>Oral iron supplementation is considered first-line therapy. Numerous formulations are available (Box 5). Multivitamins or supplements with low iron concentrations and modified-release formulations are ineffective. Ferrous iron taken on an empty stomach ensures optimal absorption. Oral iron polymaltose is not dependent on gastric acidity or vitamin C, is best taken with food, and represents an alternative preparation.<span><sup>7</sup></span> Elemental oral iron doses of larger than or equal to 60 mg reduce the absorption of subsequent oral doses.<span><sup>21</sup></span> A single 200 mg dose taken on alternate days results in about twice the absorption of a single 100 mg daily dose.<span><sup>22</sup></span> Twice-daily dosing has the lowest absorption.<span><sup>23</sup></span> Alternate day single doses are associated with significantly higher iron absorption and lower hepcidin induction compared with daily dosing,<span><sup>23</sup></span> and may have reduced gastrointestinal adverse events,<span><sup>24</sup></span> compliance concerns and therapy cessation.<span><sup>7</sup></span></p><p>Supplementation with intravenous iron results in a faster haemoglobin concentration increase compared with oral iron supplementation, although haemoglobin levels at 12 weeks are similar.<span><sup>6-8, 11</sup></span> The indications, available formulations, duration of administration and maximum dosage are described in Box 6. Current parenteral iron formulations are well tolerated and suitable for administration in primary care. Monitoring is generally advised despite no associations with serious infusion reactions.<span><sup>25</sup></span> Parenteral iron should be avoided in patients with active infection.<span><sup>25</sup></span> Skin staining can occur with extravasation. Hypophosphataemia is most common after ferric carboxymaltose, with the condition usually asymptomatic, and recovery expected over eight to ten weeks.<span><sup>7</sup></span> Routine measurement of phosphate is not recommended if asymptomatic. Intramuscular administration of iron is not routinely recommended.</p><p>After commencing iron therapy, haemoglobin levels should be checked within two to four weeks for an expected rise of more than or equal to 10 g/L.<span><sup>6</sup></span> Serum ferritin and haemoglobin levels should be measured monthly for the first three months, targeting serum ferritin normalisation or a haemoglobin increase of 20 g/L in IDA.<span><sup>6</sup></span> Oral iron should be continued for at least three months following an effective response; adherence and impaired iron uptake should be considered with inadequate responses. Thereafter, ferritin and haemoglobin levels should be monitored every three to six months for 12 months after treatment of iron deficiency and its underlying cause.<span><sup>6</sup></span> Iron supplementation should be restarted if levels are not maintained, and further investigations considered.</p><p>Implementation of routine ferritin testing by the Australian Red Cross Lifeblood will increase detection of iron deficiency among blood donors. Low serum ferritin levels are diagnostic of absolute iron deficiency and require clinical evaluation. The aetiologies of iron deficiency can be broadly categorised into physiological, inadequate dietary intake or absorption, blood loss, and rare genetic causes. Risk stratification of individuals should be considered to target investigations. Following the diagnosis of iron deficiency, iron replacement should be started early.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 7","pages":"360-364"},"PeriodicalIF":8.5000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52429","citationCount":"0","resultStr":"{\"title\":\"Updating the diagnosis and management of iron deficiency in the era of routine ferritin testing of blood donors by Australian Red Cross Lifeblood\",\"authors\":\"Gary D Zhang, Daniel Johnstone, Michael F Leahy, John K Olynyk\",\"doi\":\"10.5694/mja2.52429\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Iron deficiency is the most common micronutrient deficiency worldwide<span><sup>1</sup></span> and the predominant cause of anaemia, which affects one-quarter of the global population.<span><sup>2</sup></span></p><p>In Australia, 22.3% of women have depleted iron stores (serum ferritin level < 30 μg/L), with pre-menopausal women disproportionately affected.<span><sup>3</sup></span> In contrast, 3.5% of men are iron deficient.<span><sup>3</sup></span></p><p>The Australian Red Cross Lifeblood implemented routine ferritin level testing in August 2023 for new whole blood donors (105 069 in 2023),<span><sup>4</sup></span> with expanded testing to include returning blood donors in 2024.<span><sup>5</sup></span> Donors are formally advised if their ferritin result is outside the reference intervals of 15–400 μg/L for female donors and 30–500 μg/L for male donors.<span><sup>5</sup></span> This will identify a considerable number of iron deficient adults who will be directed to their primary care physician for management. In the context of this policy change and implications for primary care, this article provides a guide for investigating and managing absolute iron deficiency.</p><p>Iron stores inadequate to meet the demands of the body result in absolute iron deficiency, which is associated with a compensatory reduction in serum hepcidin concentration to stimulate an increase in gastrointestinal iron absorption and restore homeostasis.<span><sup>6-8</sup></span> Functional iron deficiency occurs when relatively normal iron stores are unable to be released for physiological requirements due to inappropriately elevated serum hepcidin levels, as may occur in chronic inflammatory conditions, including obesity, chronic disease and neoplasia.<span><sup>6-8</sup></span> Absolute and functional iron deficiency can also co-exist.<span><sup>7</sup></span> A ferritin level below the reference interval should always be interpreted as absolute iron deficiency.</p><p>The diagnosis of iron deficiency is based on routinely available blood biomarkers as described in Box 1. Serum ferritin level cut-offs to diagnose iron deficiency vary considerably,<span><sup>9</sup></span> from less than 15 μg/L used by the World Health Organization,<span><sup>10</sup></span> which predicts absent iron stores with very high specificity,<span><sup>7</sup></span> to less than 30 μg/L commonly used in Australia.<span><sup>7, 8, 11, 12</sup></span> Although the sex-based cut-offs adopted by the Australian Red Cross Lifeblood were reportedly derived from the Royal College of Pathologists of Australasia,<span><sup>12</sup></span> there is significant concern regarding inequalities using unconventional sex-based cut-offs, with underdiagnosis and undertreatment of iron deficient women. As an acute-phase reactant, ferritin may be falsely normal or elevated in iron deficient individuals when there is concurrent inflammation, obesity, steatotic liver disease, malignancy or other chronic disease.<span><sup>6, 7, 11</sup></span> Thus, a serum ferritin level less than 70 μg/L in an individual with a concurrent inflammatory condition may suggest iron deficiency.<span><sup>10</sup></span> Transferrin saturation values less than 20% indicate low serum iron bioavailability, consistent with absolute or functional iron deficiency. The mean cell volume and mean cell haemoglobin concentration are sensitive measures for iron deficiency anaemia (IDA) when B12 or folate deficiency are absent.<span><sup>6, 11</sup></span></p><p>Further assessment must be conducted to define the underlying aetiology of iron deficiency, which can be broadly categorised into physiological, inadequate intake or absorption, blood loss, and rare genetic causes (Box 2). Factors such as age, sex and ethnicity influence the probability of different aetiologies. Although physiological causes are commonly suspected in younger individuals, the incidence of pathological causes, such as colorectal malignancy, increases with age (Box 3). Risk stratification is necessary to guide appropriate investigations. A suggested approach to a low serum ferritin result is presented in Box 4.</p><p>Physiological causes of iron deficiency predominately affect pre-menopausal women, pregnant women and growing children. Menstrual blood loss contributes significantly to iron deficiency, with iron deficiency affecting around half of women with heavy menstrual bleeding.<span><sup>6-8, 11</sup></span></p><p>Iron uptake is affected by dietary intake and absorption. Haem iron is efficiently absorbed in the duodenum, whereas non-haem iron is less efficiently absorbed and influenced by dietary composition.<span><sup>13</sup></span> Several dietary factors inhibit non-haem iron absorption (Box 2).<span><sup>13</sup></span> The ingestion of ascorbic acid (vitamin C), lactic acid (found in fermented foods) and animal meat enhances the absorption of iron.<span><sup>13</sup></span> Gastric acid, which can be impaired by medications, aids in the conversion of insoluble ferric non-haem iron to the absorbable ferrous form.<span><sup>14</sup></span> Surgical resection or bypass involving the stomach or small intestine (or both) predisposes the patient to iron deficiency due to malabsorption and reduced food intake.<span><sup>15</sup></span></p><p>Coeliac disease has a global prevalence of 0.7–1.4% and accounts for about 3% of IDA in the general population.<span><sup>16</sup></span> Serological testing for coeliac disease using serum tissue transglutaminase IgA antibody levels should be undertaken for assessment of iron deficiency.<span><sup>6, 7</sup></span> In the 2–3% of coeliac patients with IgA deficiency, an IgA level or IgG-based assay, such as deamidated gliadin peptide, should be performed.<span><sup>6, 7</sup></span> Duodenal biopsies taken when the patient is on a gluten-containing diet remains the gold standard for diagnosis of coeliac disease in Australia.</p><p>Autoimmune gastritis, generally associated with pernicious anaemia, is commonly refractory to oral iron supplementation and reported in 27% of individuals with unexplained IDA.<span><sup>17</sup></span> <i>Helicobacter pylori</i> infection is associated with iron deficiency and eradication improves iron stores, especially in cases previously refractory to oral iron supplementation.<span><sup>17</sup></span></p><p>In obesity, iron deficiency can result from reduced iron absorption.<span><sup>7</sup></span></p><p>There are also rare genetic causes of unexplained iron deficiency.<span><sup>6, 7</sup></span></p><p>Blood loss is the most common and most significant pathological cause of iron deficiency, with aetiologies described in Box 2. Gastrointestinal blood loss accounts for most cases of iron deficiency,<span><sup>6, 7, 9, 11, 18</sup></span> with bidirectional endoscopic examination detecting a potential gastrointestinal bleeding cause in two-thirds of men and post-menopausal women with IDA. Bidirectional endoscopic examination should be routinely considered for all adults with iron deficiency as the technique shows a detection rate of 11% for gastrointestinal malignancy and 9% for colorectal malignancy.<span><sup>6-9</sup></span> Faecal occult blood testing is used for asymptomatic average-risk bowel cancer screening and should not guide iron deficiency investigations.<span><sup>6, 7</sup></span> Small intestine investigation, predominantly with capsule endoscopy, may be considered in recurrent or refractory IDA following unremarkable bidirectional endoscopy results.<span><sup>19</sup></span> When colonoscopy is contraindicated, computed tomography colonography can help rule out colorectal lesions larger than or equal to 6 mm, but cannot provide histopathological diagnosis.<span><sup>7, 20</sup></span> Medications can exacerbate blood loss, particularly non-steroidal anti-inflammatory drugs and anti-thrombotics.<span><sup>6-8</sup></span> Urinalysis is recommended to screen for microscopic haematuria, although this test is not sensitive for urological malignancies.<span><sup>6</sup></span> Stool investigations for intestinal parasitic infections can be done for at-risk individuals with exposure to endemic regions.<span><sup>8</sup></span> Frequent whole blood donation can result in iron deficiency.<span><sup>11</sup></span></p><p>Iron supplementation, available in oral or parenteral forms, is required for all individuals with IDA and should be started promptly to replace body iron stores and resolve symptoms. Iron replacement for non-anaemic iron deficiency improves symptoms and clinical outcomes.<span><sup>6, 7</sup></span> Iron-deplete women with serum ferritin levels of 15–30 μg/L will not be identified through the Australian Red Cross Lifeblood testing, although may benefit from iron replacement. Blood transfusion with restrictive targets should be reserved for severe symptomatic anaemia and symptoms of reduced oxygen-carrying capacity with cardiovascular compromise or ongoing blood loss, when iron replacement alone is insufficient.<span><sup>6</sup></span> Increasing dietary iron intake alone is insufficient for iron deficiency, although should be optimised for secondary prevention.</p><p>Oral iron supplementation is considered first-line therapy. Numerous formulations are available (Box 5). Multivitamins or supplements with low iron concentrations and modified-release formulations are ineffective. Ferrous iron taken on an empty stomach ensures optimal absorption. Oral iron polymaltose is not dependent on gastric acidity or vitamin C, is best taken with food, and represents an alternative preparation.<span><sup>7</sup></span> Elemental oral iron doses of larger than or equal to 60 mg reduce the absorption of subsequent oral doses.<span><sup>21</sup></span> A single 200 mg dose taken on alternate days results in about twice the absorption of a single 100 mg daily dose.<span><sup>22</sup></span> Twice-daily dosing has the lowest absorption.<span><sup>23</sup></span> Alternate day single doses are associated with significantly higher iron absorption and lower hepcidin induction compared with daily dosing,<span><sup>23</sup></span> and may have reduced gastrointestinal adverse events,<span><sup>24</sup></span> compliance concerns and therapy cessation.<span><sup>7</sup></span></p><p>Supplementation with intravenous iron results in a faster haemoglobin concentration increase compared with oral iron supplementation, although haemoglobin levels at 12 weeks are similar.<span><sup>6-8, 11</sup></span> The indications, available formulations, duration of administration and maximum dosage are described in Box 6. Current parenteral iron formulations are well tolerated and suitable for administration in primary care. Monitoring is generally advised despite no associations with serious infusion reactions.<span><sup>25</sup></span> Parenteral iron should be avoided in patients with active infection.<span><sup>25</sup></span> Skin staining can occur with extravasation. Hypophosphataemia is most common after ferric carboxymaltose, with the condition usually asymptomatic, and recovery expected over eight to ten weeks.<span><sup>7</sup></span> Routine measurement of phosphate is not recommended if asymptomatic. Intramuscular administration of iron is not routinely recommended.</p><p>After commencing iron therapy, haemoglobin levels should be checked within two to four weeks for an expected rise of more than or equal to 10 g/L.<span><sup>6</sup></span> Serum ferritin and haemoglobin levels should be measured monthly for the first three months, targeting serum ferritin normalisation or a haemoglobin increase of 20 g/L in IDA.<span><sup>6</sup></span> Oral iron should be continued for at least three months following an effective response; adherence and impaired iron uptake should be considered with inadequate responses. Thereafter, ferritin and haemoglobin levels should be monitored every three to six months for 12 months after treatment of iron deficiency and its underlying cause.<span><sup>6</sup></span> Iron supplementation should be restarted if levels are not maintained, and further investigations considered.</p><p>Implementation of routine ferritin testing by the Australian Red Cross Lifeblood will increase detection of iron deficiency among blood donors. Low serum ferritin levels are diagnostic of absolute iron deficiency and require clinical evaluation. The aetiologies of iron deficiency can be broadly categorised into physiological, inadequate dietary intake or absorption, blood loss, and rare genetic causes. Risk stratification of individuals should be considered to target investigations. Following the diagnosis of iron deficiency, iron replacement should be started early.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>\",\"PeriodicalId\":18214,\"journal\":{\"name\":\"Medical Journal of Australia\",\"volume\":\"221 7\",\"pages\":\"360-364\"},\"PeriodicalIF\":8.5000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52429\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Journal of Australia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52429\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52429","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Updating the diagnosis and management of iron deficiency in the era of routine ferritin testing of blood donors by Australian Red Cross Lifeblood
Iron deficiency is the most common micronutrient deficiency worldwide1 and the predominant cause of anaemia, which affects one-quarter of the global population.2
In Australia, 22.3% of women have depleted iron stores (serum ferritin level < 30 μg/L), with pre-menopausal women disproportionately affected.3 In contrast, 3.5% of men are iron deficient.3
The Australian Red Cross Lifeblood implemented routine ferritin level testing in August 2023 for new whole blood donors (105 069 in 2023),4 with expanded testing to include returning blood donors in 2024.5 Donors are formally advised if their ferritin result is outside the reference intervals of 15–400 μg/L for female donors and 30–500 μg/L for male donors.5 This will identify a considerable number of iron deficient adults who will be directed to their primary care physician for management. In the context of this policy change and implications for primary care, this article provides a guide for investigating and managing absolute iron deficiency.
Iron stores inadequate to meet the demands of the body result in absolute iron deficiency, which is associated with a compensatory reduction in serum hepcidin concentration to stimulate an increase in gastrointestinal iron absorption and restore homeostasis.6-8 Functional iron deficiency occurs when relatively normal iron stores are unable to be released for physiological requirements due to inappropriately elevated serum hepcidin levels, as may occur in chronic inflammatory conditions, including obesity, chronic disease and neoplasia.6-8 Absolute and functional iron deficiency can also co-exist.7 A ferritin level below the reference interval should always be interpreted as absolute iron deficiency.
The diagnosis of iron deficiency is based on routinely available blood biomarkers as described in Box 1. Serum ferritin level cut-offs to diagnose iron deficiency vary considerably,9 from less than 15 μg/L used by the World Health Organization,10 which predicts absent iron stores with very high specificity,7 to less than 30 μg/L commonly used in Australia.7, 8, 11, 12 Although the sex-based cut-offs adopted by the Australian Red Cross Lifeblood were reportedly derived from the Royal College of Pathologists of Australasia,12 there is significant concern regarding inequalities using unconventional sex-based cut-offs, with underdiagnosis and undertreatment of iron deficient women. As an acute-phase reactant, ferritin may be falsely normal or elevated in iron deficient individuals when there is concurrent inflammation, obesity, steatotic liver disease, malignancy or other chronic disease.6, 7, 11 Thus, a serum ferritin level less than 70 μg/L in an individual with a concurrent inflammatory condition may suggest iron deficiency.10 Transferrin saturation values less than 20% indicate low serum iron bioavailability, consistent with absolute or functional iron deficiency. The mean cell volume and mean cell haemoglobin concentration are sensitive measures for iron deficiency anaemia (IDA) when B12 or folate deficiency are absent.6, 11
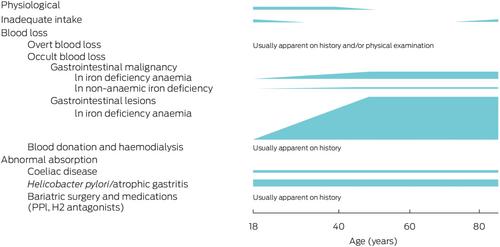
Further assessment must be conducted to define the underlying aetiology of iron deficiency, which can be broadly categorised into physiological, inadequate intake or absorption, blood loss, and rare genetic causes (Box 2). Factors such as age, sex and ethnicity influence the probability of different aetiologies. Although physiological causes are commonly suspected in younger individuals, the incidence of pathological causes, such as colorectal malignancy, increases with age (Box 3). Risk stratification is necessary to guide appropriate investigations. A suggested approach to a low serum ferritin result is presented in Box 4.
Physiological causes of iron deficiency predominately affect pre-menopausal women, pregnant women and growing children. Menstrual blood loss contributes significantly to iron deficiency, with iron deficiency affecting around half of women with heavy menstrual bleeding.6-8, 11
Iron uptake is affected by dietary intake and absorption. Haem iron is efficiently absorbed in the duodenum, whereas non-haem iron is less efficiently absorbed and influenced by dietary composition.13 Several dietary factors inhibit non-haem iron absorption (Box 2).13 The ingestion of ascorbic acid (vitamin C), lactic acid (found in fermented foods) and animal meat enhances the absorption of iron.13 Gastric acid, which can be impaired by medications, aids in the conversion of insoluble ferric non-haem iron to the absorbable ferrous form.14 Surgical resection or bypass involving the stomach or small intestine (or both) predisposes the patient to iron deficiency due to malabsorption and reduced food intake.15
Coeliac disease has a global prevalence of 0.7–1.4% and accounts for about 3% of IDA in the general population.16 Serological testing for coeliac disease using serum tissue transglutaminase IgA antibody levels should be undertaken for assessment of iron deficiency.6, 7 In the 2–3% of coeliac patients with IgA deficiency, an IgA level or IgG-based assay, such as deamidated gliadin peptide, should be performed.6, 7 Duodenal biopsies taken when the patient is on a gluten-containing diet remains the gold standard for diagnosis of coeliac disease in Australia.
Autoimmune gastritis, generally associated with pernicious anaemia, is commonly refractory to oral iron supplementation and reported in 27% of individuals with unexplained IDA.17Helicobacter pylori infection is associated with iron deficiency and eradication improves iron stores, especially in cases previously refractory to oral iron supplementation.17
In obesity, iron deficiency can result from reduced iron absorption.7
There are also rare genetic causes of unexplained iron deficiency.6, 7
Blood loss is the most common and most significant pathological cause of iron deficiency, with aetiologies described in Box 2. Gastrointestinal blood loss accounts for most cases of iron deficiency,6, 7, 9, 11, 18 with bidirectional endoscopic examination detecting a potential gastrointestinal bleeding cause in two-thirds of men and post-menopausal women with IDA. Bidirectional endoscopic examination should be routinely considered for all adults with iron deficiency as the technique shows a detection rate of 11% for gastrointestinal malignancy and 9% for colorectal malignancy.6-9 Faecal occult blood testing is used for asymptomatic average-risk bowel cancer screening and should not guide iron deficiency investigations.6, 7 Small intestine investigation, predominantly with capsule endoscopy, may be considered in recurrent or refractory IDA following unremarkable bidirectional endoscopy results.19 When colonoscopy is contraindicated, computed tomography colonography can help rule out colorectal lesions larger than or equal to 6 mm, but cannot provide histopathological diagnosis.7, 20 Medications can exacerbate blood loss, particularly non-steroidal anti-inflammatory drugs and anti-thrombotics.6-8 Urinalysis is recommended to screen for microscopic haematuria, although this test is not sensitive for urological malignancies.6 Stool investigations for intestinal parasitic infections can be done for at-risk individuals with exposure to endemic regions.8 Frequent whole blood donation can result in iron deficiency.11
Iron supplementation, available in oral or parenteral forms, is required for all individuals with IDA and should be started promptly to replace body iron stores and resolve symptoms. Iron replacement for non-anaemic iron deficiency improves symptoms and clinical outcomes.6, 7 Iron-deplete women with serum ferritin levels of 15–30 μg/L will not be identified through the Australian Red Cross Lifeblood testing, although may benefit from iron replacement. Blood transfusion with restrictive targets should be reserved for severe symptomatic anaemia and symptoms of reduced oxygen-carrying capacity with cardiovascular compromise or ongoing blood loss, when iron replacement alone is insufficient.6 Increasing dietary iron intake alone is insufficient for iron deficiency, although should be optimised for secondary prevention.
Oral iron supplementation is considered first-line therapy. Numerous formulations are available (Box 5). Multivitamins or supplements with low iron concentrations and modified-release formulations are ineffective. Ferrous iron taken on an empty stomach ensures optimal absorption. Oral iron polymaltose is not dependent on gastric acidity or vitamin C, is best taken with food, and represents an alternative preparation.7 Elemental oral iron doses of larger than or equal to 60 mg reduce the absorption of subsequent oral doses.21 A single 200 mg dose taken on alternate days results in about twice the absorption of a single 100 mg daily dose.22 Twice-daily dosing has the lowest absorption.23 Alternate day single doses are associated with significantly higher iron absorption and lower hepcidin induction compared with daily dosing,23 and may have reduced gastrointestinal adverse events,24 compliance concerns and therapy cessation.7
Supplementation with intravenous iron results in a faster haemoglobin concentration increase compared with oral iron supplementation, although haemoglobin levels at 12 weeks are similar.6-8, 11 The indications, available formulations, duration of administration and maximum dosage are described in Box 6. Current parenteral iron formulations are well tolerated and suitable for administration in primary care. Monitoring is generally advised despite no associations with serious infusion reactions.25 Parenteral iron should be avoided in patients with active infection.25 Skin staining can occur with extravasation. Hypophosphataemia is most common after ferric carboxymaltose, with the condition usually asymptomatic, and recovery expected over eight to ten weeks.7 Routine measurement of phosphate is not recommended if asymptomatic. Intramuscular administration of iron is not routinely recommended.
After commencing iron therapy, haemoglobin levels should be checked within two to four weeks for an expected rise of more than or equal to 10 g/L.6 Serum ferritin and haemoglobin levels should be measured monthly for the first three months, targeting serum ferritin normalisation or a haemoglobin increase of 20 g/L in IDA.6 Oral iron should be continued for at least three months following an effective response; adherence and impaired iron uptake should be considered with inadequate responses. Thereafter, ferritin and haemoglobin levels should be monitored every three to six months for 12 months after treatment of iron deficiency and its underlying cause.6 Iron supplementation should be restarted if levels are not maintained, and further investigations considered.
Implementation of routine ferritin testing by the Australian Red Cross Lifeblood will increase detection of iron deficiency among blood donors. Low serum ferritin levels are diagnostic of absolute iron deficiency and require clinical evaluation. The aetiologies of iron deficiency can be broadly categorised into physiological, inadequate dietary intake or absorption, blood loss, and rare genetic causes. Risk stratification of individuals should be considered to target investigations. Following the diagnosis of iron deficiency, iron replacement should be started early.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
