Johanna Papanikolla, Melissa McGowan, Mythili Chunduru, Holli Winters, Todd Pesavento, Rachel Smith, Navdeep Singh, Michael Wellner, Lindsay Sobotka, Annelise Nolan
{"title":"肾移植受者使用延迟启动、缩短疗程的 glecaprevir/pibrentasvir 与标准疗法治疗供体源性丙型肝炎病毒的实际经验。","authors":"Johanna Papanikolla, Melissa McGowan, Mythili Chunduru, Holli Winters, Todd Pesavento, Rachel Smith, Navdeep Singh, Michael Wellner, Lindsay Sobotka, Annelise Nolan","doi":"10.1111/tid.14366","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is limited literature describing the real-world practice of delayed initiation and shortened duration direct-acting antiviral (DAA) in kidney transplant recipients. We compared Hepatitis C virus (HCV) cure rates among kidney transplant recipients who received an HCV nucleic acid test positive (NAT +) kidney and were treated with sofosbuvir/velpatasvir (SOF/VEL) for 12 weeks or glecaprevir/pibrentasvir (G/P) for 8 weeks, a duration that is 4 weeks shorter than the guideline recommendation for treatment delay beyond 1-week post-transplant.</p><p><strong>Methods: </strong>Retrospective study of HCV-negative adult patients who received a kidney transplant from an HCV NAT+ donor between April 2019 and April 2022 treated with either SOF/VEL for 12 weeks or G/P for 8 weeks. The primary outcome was sustained virologic response 12 weeks after completion of therapy (SVR12). Secondary outcomes included time to DAA initiation, renal function, graft loss, patient death, liver function tests, and opportunistic infections.</p><p><strong>Results: </strong>102 kidney transplant recipients were included with 36 treated with G/P and 66 treated with SOF/VEL. All 36 (100%) treated with G/P achieved SVR12. One patient in the SOF/VEL group failed to achieve SVR12 but received additional therapy and was cured. Time to DAA initiation was similar with a mean of 4 weeks. There was no difference in AST/ALT > 3x ULN or renal function. One rejection occurred in each group. No patient death or graft loss was observed. There was no difference in cytomegalovirus and BK viremia between groups. CONCLUSION: Delayed initiation of DAA therapy with 12 weeks of SOF/VEL or 8 weeks of G/P achieves SVR12 in kidney transplant recipients without significant adverse effects.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e14366"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666865/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world experience in treatment of donor-derived Hepatitis C virus in kidney transplant recipients with delayed initiation, shortened course glecaprevir/pibrentasvir versus standard of care.\",\"authors\":\"Johanna Papanikolla, Melissa McGowan, Mythili Chunduru, Holli Winters, Todd Pesavento, Rachel Smith, Navdeep Singh, Michael Wellner, Lindsay Sobotka, Annelise Nolan\",\"doi\":\"10.1111/tid.14366\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is limited literature describing the real-world practice of delayed initiation and shortened duration direct-acting antiviral (DAA) in kidney transplant recipients. We compared Hepatitis C virus (HCV) cure rates among kidney transplant recipients who received an HCV nucleic acid test positive (NAT +) kidney and were treated with sofosbuvir/velpatasvir (SOF/VEL) for 12 weeks or glecaprevir/pibrentasvir (G/P) for 8 weeks, a duration that is 4 weeks shorter than the guideline recommendation for treatment delay beyond 1-week post-transplant.</p><p><strong>Methods: </strong>Retrospective study of HCV-negative adult patients who received a kidney transplant from an HCV NAT+ donor between April 2019 and April 2022 treated with either SOF/VEL for 12 weeks or G/P for 8 weeks. The primary outcome was sustained virologic response 12 weeks after completion of therapy (SVR12). Secondary outcomes included time to DAA initiation, renal function, graft loss, patient death, liver function tests, and opportunistic infections.</p><p><strong>Results: </strong>102 kidney transplant recipients were included with 36 treated with G/P and 66 treated with SOF/VEL. All 36 (100%) treated with G/P achieved SVR12. One patient in the SOF/VEL group failed to achieve SVR12 but received additional therapy and was cured. Time to DAA initiation was similar with a mean of 4 weeks. There was no difference in AST/ALT > 3x ULN or renal function. One rejection occurred in each group. No patient death or graft loss was observed. There was no difference in cytomegalovirus and BK viremia between groups. CONCLUSION: Delayed initiation of DAA therapy with 12 weeks of SOF/VEL or 8 weeks of G/P achieves SVR12 in kidney transplant recipients without significant adverse effects.</p>\",\"PeriodicalId\":23318,\"journal\":{\"name\":\"Transplant Infectious Disease\",\"volume\":\" \",\"pages\":\"e14366\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666865/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant Infectious Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/tid.14366\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.14366","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Real-world experience in treatment of donor-derived Hepatitis C virus in kidney transplant recipients with delayed initiation, shortened course glecaprevir/pibrentasvir versus standard of care.
Background: There is limited literature describing the real-world practice of delayed initiation and shortened duration direct-acting antiviral (DAA) in kidney transplant recipients. We compared Hepatitis C virus (HCV) cure rates among kidney transplant recipients who received an HCV nucleic acid test positive (NAT +) kidney and were treated with sofosbuvir/velpatasvir (SOF/VEL) for 12 weeks or glecaprevir/pibrentasvir (G/P) for 8 weeks, a duration that is 4 weeks shorter than the guideline recommendation for treatment delay beyond 1-week post-transplant.
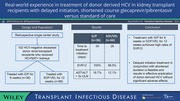
Methods: Retrospective study of HCV-negative adult patients who received a kidney transplant from an HCV NAT+ donor between April 2019 and April 2022 treated with either SOF/VEL for 12 weeks or G/P for 8 weeks. The primary outcome was sustained virologic response 12 weeks after completion of therapy (SVR12). Secondary outcomes included time to DAA initiation, renal function, graft loss, patient death, liver function tests, and opportunistic infections.
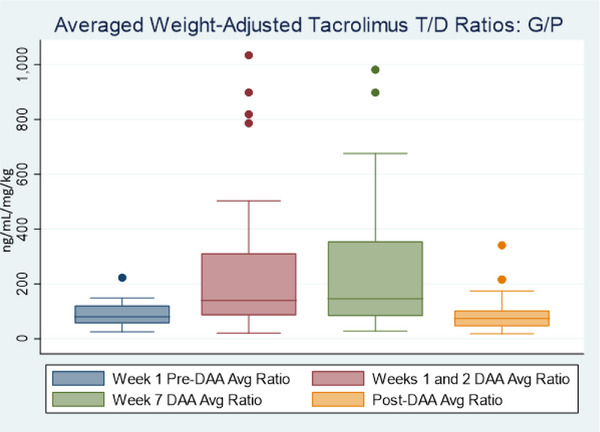
Results: 102 kidney transplant recipients were included with 36 treated with G/P and 66 treated with SOF/VEL. All 36 (100%) treated with G/P achieved SVR12. One patient in the SOF/VEL group failed to achieve SVR12 but received additional therapy and was cured. Time to DAA initiation was similar with a mean of 4 weeks. There was no difference in AST/ALT > 3x ULN or renal function. One rejection occurred in each group. No patient death or graft loss was observed. There was no difference in cytomegalovirus and BK viremia between groups. CONCLUSION: Delayed initiation of DAA therapy with 12 weeks of SOF/VEL or 8 weeks of G/P achieves SVR12 in kidney transplant recipients without significant adverse effects.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
