Sheldon E. Litwin MD , Jan Komtebedde DVM , Barry A. Borlaug MD , David M. Kaye MD, PhD , Gerd Hasenfuβ MD , Rami Kawash MD , Elke Hoendermis MD, PhD , Scott L. Hummel MD , Maja Cikes MD, PhD , Finn Gustafsson MD, PhD , Eugene S. Chung MD , Rajeev C. Mohan MD , Aaron L. Sverdlov MBBS, PhD , Vijendra Swarup MD , Sebastian Winkler MD , Christopher S. Hayward MD , Martin W. Bergmann MD , Heiko Bugger MD , Scott McKenzie MD , Ajith Nair MD , Sanjiv J. Shah MD
{"title":"射血分数保留或轻度降低的心力衰竭患者进行心房分流术后的长期安全性和疗效:REDUCE LAP-HF I 和 II 试验的 5 年和 3 年随访。","authors":"Sheldon E. Litwin MD , Jan Komtebedde DVM , Barry A. Borlaug MD , David M. Kaye MD, PhD , Gerd Hasenfuβ MD , Rami Kawash MD , Elke Hoendermis MD, PhD , Scott L. Hummel MD , Maja Cikes MD, PhD , Finn Gustafsson MD, PhD , Eugene S. Chung MD , Rajeev C. Mohan MD , Aaron L. Sverdlov MBBS, PhD , Vijendra Swarup MD , Sebastian Winkler MD , Christopher S. Hayward MD , Martin W. Bergmann MD , Heiko Bugger MD , Scott McKenzie MD , Ajith Nair MD , Sanjiv J. Shah MD","doi":"10.1016/j.ahj.2024.08.014","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>There is a little evidence regarding long-term safety and efficacy for atrial shunt devices in heart failure (HF).</div></div><div><h3>Methods</h3><div>The REDUCE LAP-HF I (n = 44) and II (n = 621) trials (RCT-I and -II) were multicenter, randomized, sham-controlled trials of patients with HF and ejection fraction >40%. Outcome data were analyzed from RCT-I, a mechanistic trial with 5-year follow-up, and RCT-II, a pivotal trial identifying a responder group (n = 313) defined by exercise PVR <1.74 WU and no cardiac rhythm management device with 3-year follow-up.</div></div><div><h3>Results</h3><div>At 5 years in RCT I, there were no differences in cardiovascular (CV) mortality, HF events, embolic stroke, or new-onset atrial fibrillation between groups. After 3 years in RCT II, there was no difference in the primary outcome (hierarchical composite of CV mortality, stroke, HF events, and KCCQ) between shunt and sham in the overall trial. Compared to sham, those with responder characteristics in RCT-II had a better outcome with shunt (win ratio 1.6 [95% CI 1.2-2.2], <em>P</em> = .006; 44% reduction in HF events [shunt 9 vs. control 16 per 100 patient-years], <em>P</em> = .005; and greater improvement in KCCQ overall summary score [+17.9 ± 20.0 vs. +7.6 ± 20.4], <em>P</em> < .001), while nonresponders had significantly more HF events. Shunt treatment at 3 years was associated with a higher rate of ischemic stroke (3.2% vs. 0%, 95% CI 2%-6.1%, <em>P</em> = .032) and lower incidence of worsening kidney dysfunction (10.7% vs. 19.3%, <em>P</em> = .041).</div></div><div><h3>Conclusions</h3><div>With up to 5 years of follow up, adverse events were low in patients receiving atrial shunts. In the responder group, atrial shunt treatment was associated with a significantly lower HF event rate and improved KCCQ compared to sham through 3 years of follow-up.</div></div><div><h3>Clinicaltrials.gov registration:</h3><div>NCT02600234, NCT03088033.</div></div>","PeriodicalId":7868,"journal":{"name":"American heart journal","volume":"278 ","pages":"Pages 106-116"},"PeriodicalIF":3.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Long term safety and outcomes after atrial shunting for heart failure with preserved or mildly reduced ejection fraction: 5-year and 3-year follow-up in the REDUCE LAP-HF I and II trials\",\"authors\":\"Sheldon E. Litwin MD , Jan Komtebedde DVM , Barry A. Borlaug MD , David M. Kaye MD, PhD , Gerd Hasenfuβ MD , Rami Kawash MD , Elke Hoendermis MD, PhD , Scott L. Hummel MD , Maja Cikes MD, PhD , Finn Gustafsson MD, PhD , Eugene S. Chung MD , Rajeev C. Mohan MD , Aaron L. Sverdlov MBBS, PhD , Vijendra Swarup MD , Sebastian Winkler MD , Christopher S. Hayward MD , Martin W. Bergmann MD , Heiko Bugger MD , Scott McKenzie MD , Ajith Nair MD , Sanjiv J. Shah MD\",\"doi\":\"10.1016/j.ahj.2024.08.014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><div>There is a little evidence regarding long-term safety and efficacy for atrial shunt devices in heart failure (HF).</div></div><div><h3>Methods</h3><div>The REDUCE LAP-HF I (n = 44) and II (n = 621) trials (RCT-I and -II) were multicenter, randomized, sham-controlled trials of patients with HF and ejection fraction >40%. Outcome data were analyzed from RCT-I, a mechanistic trial with 5-year follow-up, and RCT-II, a pivotal trial identifying a responder group (n = 313) defined by exercise PVR <1.74 WU and no cardiac rhythm management device with 3-year follow-up.</div></div><div><h3>Results</h3><div>At 5 years in RCT I, there were no differences in cardiovascular (CV) mortality, HF events, embolic stroke, or new-onset atrial fibrillation between groups. After 3 years in RCT II, there was no difference in the primary outcome (hierarchical composite of CV mortality, stroke, HF events, and KCCQ) between shunt and sham in the overall trial. Compared to sham, those with responder characteristics in RCT-II had a better outcome with shunt (win ratio 1.6 [95% CI 1.2-2.2], <em>P</em> = .006; 44% reduction in HF events [shunt 9 vs. control 16 per 100 patient-years], <em>P</em> = .005; and greater improvement in KCCQ overall summary score [+17.9 ± 20.0 vs. +7.6 ± 20.4], <em>P</em> < .001), while nonresponders had significantly more HF events. Shunt treatment at 3 years was associated with a higher rate of ischemic stroke (3.2% vs. 0%, 95% CI 2%-6.1%, <em>P</em> = .032) and lower incidence of worsening kidney dysfunction (10.7% vs. 19.3%, <em>P</em> = .041).</div></div><div><h3>Conclusions</h3><div>With up to 5 years of follow up, adverse events were low in patients receiving atrial shunts. In the responder group, atrial shunt treatment was associated with a significantly lower HF event rate and improved KCCQ compared to sham through 3 years of follow-up.</div></div><div><h3>Clinicaltrials.gov registration:</h3><div>NCT02600234, NCT03088033.</div></div>\",\"PeriodicalId\":7868,\"journal\":{\"name\":\"American heart journal\",\"volume\":\"278 \",\"pages\":\"Pages 106-116\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American heart journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0002870324002163\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American heart journal","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0002870324002163","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Long term safety and outcomes after atrial shunting for heart failure with preserved or mildly reduced ejection fraction: 5-year and 3-year follow-up in the REDUCE LAP-HF I and II trials
Background
There is a little evidence regarding long-term safety and efficacy for atrial shunt devices in heart failure (HF).
Methods
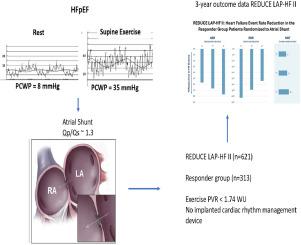
The REDUCE LAP-HF I (n = 44) and II (n = 621) trials (RCT-I and -II) were multicenter, randomized, sham-controlled trials of patients with HF and ejection fraction >40%. Outcome data were analyzed from RCT-I, a mechanistic trial with 5-year follow-up, and RCT-II, a pivotal trial identifying a responder group (n = 313) defined by exercise PVR <1.74 WU and no cardiac rhythm management device with 3-year follow-up.
Results
At 5 years in RCT I, there were no differences in cardiovascular (CV) mortality, HF events, embolic stroke, or new-onset atrial fibrillation between groups. After 3 years in RCT II, there was no difference in the primary outcome (hierarchical composite of CV mortality, stroke, HF events, and KCCQ) between shunt and sham in the overall trial. Compared to sham, those with responder characteristics in RCT-II had a better outcome with shunt (win ratio 1.6 [95% CI 1.2-2.2], P = .006; 44% reduction in HF events [shunt 9 vs. control 16 per 100 patient-years], P = .005; and greater improvement in KCCQ overall summary score [+17.9 ± 20.0 vs. +7.6 ± 20.4], P < .001), while nonresponders had significantly more HF events. Shunt treatment at 3 years was associated with a higher rate of ischemic stroke (3.2% vs. 0%, 95% CI 2%-6.1%, P = .032) and lower incidence of worsening kidney dysfunction (10.7% vs. 19.3%, P = .041).
Conclusions
With up to 5 years of follow up, adverse events were low in patients receiving atrial shunts. In the responder group, atrial shunt treatment was associated with a significantly lower HF event rate and improved KCCQ compared to sham through 3 years of follow-up.
期刊介绍:
The American Heart Journal will consider for publication suitable articles on topics pertaining to the broad discipline of cardiovascular disease. Our goal is to provide the reader primary investigation, scholarly review, and opinion concerning the practice of cardiovascular medicine. We especially encourage submission of 3 types of reports that are not frequently seen in cardiovascular journals: negative clinical studies, reports on study designs, and studies involving the organization of medical care. The Journal does not accept individual case reports or original articles involving bench laboratory or animal research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
