Hailey Tyndall, Lawrence Worobetz, Matthew Nicholson
{"title":"一例伴有自身免疫性肝炎的自身免疫性骨髓纤维化病例","authors":"Hailey Tyndall, Lawrence Worobetz, Matthew Nicholson","doi":"10.14740/jh1297","DOIUrl":null,"url":null,"abstract":"<p><p>Autoimmune myelofibrosis (AIMF) is a distinct, underrecognized, and rare cause of bone marrow fibrosis. It carries a favorable outcome and responds well to immunosuppression. Systemic lupus erythematosus is the most common association with AIMF, but there are other cases of associated autoimmune disorders defined in the literature. A 44-year-old female presented to hospital with a 1-month history of fatigue, malaise, and jaundice. She was found to be pancytopenic with elevated liver enzymes. Tests for Janus kinase 2, myeloproliferative leukemia, and calreticulin mutations were negative. Extensive investigations for hemolytic anemia including direct antiglobulin test, flow cytometry for paroxysmal nocturnal hemoglobinuria, testing for hereditary hemoglobinopathies, and hereditary red cell membrane disorders were non-contributory. Antinuclear antibody was positive at > 1,280, immunoglobulin G was 17.04 g/L, and anti-smooth muscle antibody (ASMA) was positive at 1:40. Characteristic features of AIMF on bone marrow biopsy led to the diagnosis of AIMF. The patient was started on prednisone 1 mg/kg with prolonged taper. Fibroscan and liver biopsy were consistent with cirrhosis and workups for other causes of liver dysfunction were unremarkable. She met criteria for diagnosis of autoimmune hepatitis (AIH). The pancytopenia and liver enzymes improved with prednisone. After 1 year of clinical stability, the patient had relapse of disease with pancytopenia, elevated liver enzymes, and similar fibrosis on repeat bone marrow biopsy. Prednisone was reinitiated at 1 mg/kg, and she was started on mycophenolate mofetil (MMF). Prednisone was tapered, and she continues to have an excellent response on MMF alone. We report a case of AIMF associated with AIH, complicated by non-immune hemolysis. AIMF is rare, and its association with AIH is described in only four other cases in the English-language literature. Overlapping biochemical features of AIH and non-immune hemolysis, which has not been well described in AIMF, lead to significant diagnostic complexity and delay. Despite this, a rapid response to corticosteroids was observed including reversal of profound transfusion dependence, normalization of hemoglobin, and reversal of biochemical evidence of hepatic inflammation. A shared pathogenesis of autoimmune fibrosis in both the bone marrow and liver is speculative but suggested by the temporal association in this case.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"13 4","pages":"158-163"},"PeriodicalIF":1.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379051/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Case of Autoimmune Myelofibrosis Associated With Autoimmune Hepatitis.\",\"authors\":\"Hailey Tyndall, Lawrence Worobetz, Matthew Nicholson\",\"doi\":\"10.14740/jh1297\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Autoimmune myelofibrosis (AIMF) is a distinct, underrecognized, and rare cause of bone marrow fibrosis. It carries a favorable outcome and responds well to immunosuppression. Systemic lupus erythematosus is the most common association with AIMF, but there are other cases of associated autoimmune disorders defined in the literature. A 44-year-old female presented to hospital with a 1-month history of fatigue, malaise, and jaundice. She was found to be pancytopenic with elevated liver enzymes. Tests for Janus kinase 2, myeloproliferative leukemia, and calreticulin mutations were negative. Extensive investigations for hemolytic anemia including direct antiglobulin test, flow cytometry for paroxysmal nocturnal hemoglobinuria, testing for hereditary hemoglobinopathies, and hereditary red cell membrane disorders were non-contributory. Antinuclear antibody was positive at > 1,280, immunoglobulin G was 17.04 g/L, and anti-smooth muscle antibody (ASMA) was positive at 1:40. Characteristic features of AIMF on bone marrow biopsy led to the diagnosis of AIMF. The patient was started on prednisone 1 mg/kg with prolonged taper. Fibroscan and liver biopsy were consistent with cirrhosis and workups for other causes of liver dysfunction were unremarkable. She met criteria for diagnosis of autoimmune hepatitis (AIH). The pancytopenia and liver enzymes improved with prednisone. After 1 year of clinical stability, the patient had relapse of disease with pancytopenia, elevated liver enzymes, and similar fibrosis on repeat bone marrow biopsy. Prednisone was reinitiated at 1 mg/kg, and she was started on mycophenolate mofetil (MMF). Prednisone was tapered, and she continues to have an excellent response on MMF alone. We report a case of AIMF associated with AIH, complicated by non-immune hemolysis. AIMF is rare, and its association with AIH is described in only four other cases in the English-language literature. Overlapping biochemical features of AIH and non-immune hemolysis, which has not been well described in AIMF, lead to significant diagnostic complexity and delay. Despite this, a rapid response to corticosteroids was observed including reversal of profound transfusion dependence, normalization of hemoglobin, and reversal of biochemical evidence of hepatic inflammation. A shared pathogenesis of autoimmune fibrosis in both the bone marrow and liver is speculative but suggested by the temporal association in this case.</p>\",\"PeriodicalId\":15964,\"journal\":{\"name\":\"Journal of hematology\",\"volume\":\"13 4\",\"pages\":\"158-163\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379051/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jh1297\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1297","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
A Case of Autoimmune Myelofibrosis Associated With Autoimmune Hepatitis.
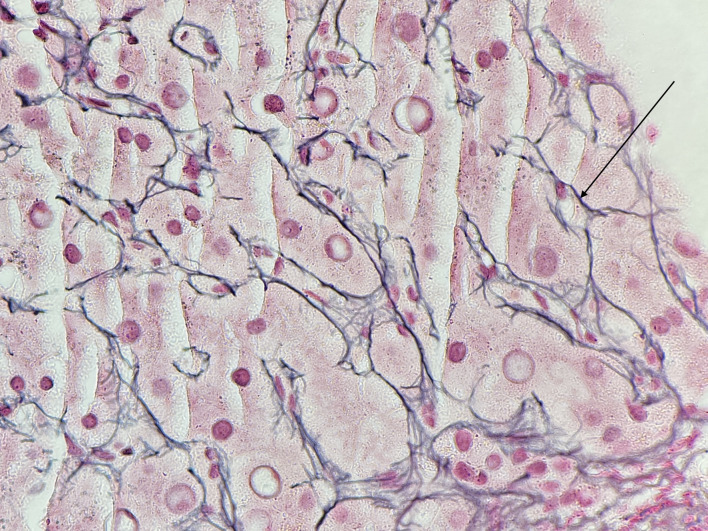
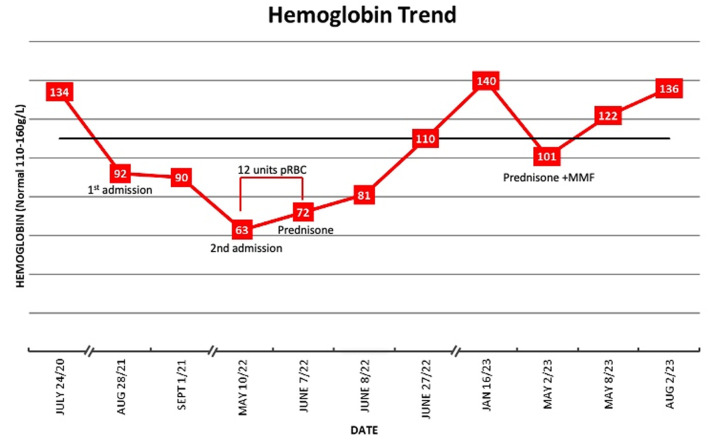
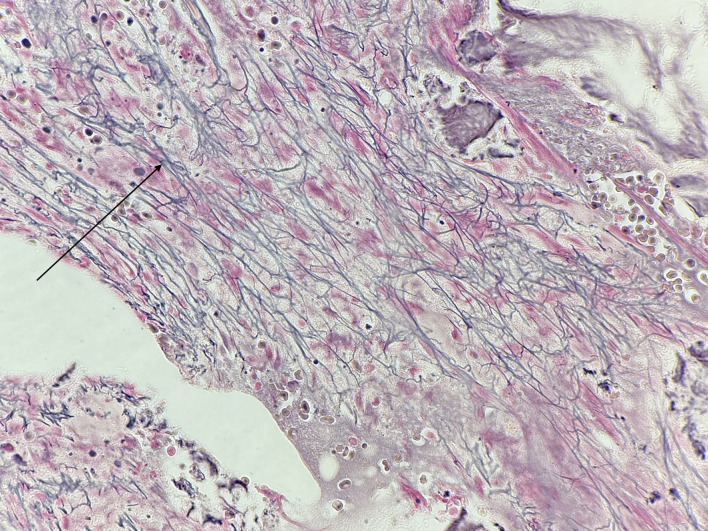
Autoimmune myelofibrosis (AIMF) is a distinct, underrecognized, and rare cause of bone marrow fibrosis. It carries a favorable outcome and responds well to immunosuppression. Systemic lupus erythematosus is the most common association with AIMF, but there are other cases of associated autoimmune disorders defined in the literature. A 44-year-old female presented to hospital with a 1-month history of fatigue, malaise, and jaundice. She was found to be pancytopenic with elevated liver enzymes. Tests for Janus kinase 2, myeloproliferative leukemia, and calreticulin mutations were negative. Extensive investigations for hemolytic anemia including direct antiglobulin test, flow cytometry for paroxysmal nocturnal hemoglobinuria, testing for hereditary hemoglobinopathies, and hereditary red cell membrane disorders were non-contributory. Antinuclear antibody was positive at > 1,280, immunoglobulin G was 17.04 g/L, and anti-smooth muscle antibody (ASMA) was positive at 1:40. Characteristic features of AIMF on bone marrow biopsy led to the diagnosis of AIMF. The patient was started on prednisone 1 mg/kg with prolonged taper. Fibroscan and liver biopsy were consistent with cirrhosis and workups for other causes of liver dysfunction were unremarkable. She met criteria for diagnosis of autoimmune hepatitis (AIH). The pancytopenia and liver enzymes improved with prednisone. After 1 year of clinical stability, the patient had relapse of disease with pancytopenia, elevated liver enzymes, and similar fibrosis on repeat bone marrow biopsy. Prednisone was reinitiated at 1 mg/kg, and she was started on mycophenolate mofetil (MMF). Prednisone was tapered, and she continues to have an excellent response on MMF alone. We report a case of AIMF associated with AIH, complicated by non-immune hemolysis. AIMF is rare, and its association with AIH is described in only four other cases in the English-language literature. Overlapping biochemical features of AIH and non-immune hemolysis, which has not been well described in AIMF, lead to significant diagnostic complexity and delay. Despite this, a rapid response to corticosteroids was observed including reversal of profound transfusion dependence, normalization of hemoglobin, and reversal of biochemical evidence of hepatic inflammation. A shared pathogenesis of autoimmune fibrosis in both the bone marrow and liver is speculative but suggested by the temporal association in this case.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
