Jens Wretborn PhD, Samia Munir-Ehrlington MD, Erika Hörlin MSc, Daniel B. Wilhelms PhD
{"title":"在分诊工具和预警评分中加入临床虚弱量表可改善 30 天后的死亡率预测:前瞻性多中心观察研究","authors":"Jens Wretborn PhD, Samia Munir-Ehrlington MD, Erika Hörlin MSc, Daniel B. Wilhelms PhD","doi":"10.1002/emp2.13244","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>Frailty, assessed with clinical frailty scale (CFS), alone or in combination with aggregated vital signs, has been proposed as a measure to better predict mortality of older patients in the emergency department (ED), but the added predictive value to conventional triage is unclear.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a secondary analysis of a prospective observational study in three EDs in Sweden that evaluated the prognostic performance of the CFS alone or in combination with the national early warning score (NEWS), triage early warning score (TEWS) or the rapid emergency triage and treatment system (RETTS) triage tool using logistic regression. The primary outcome was 30-day mortality with 7- and 90-day mortality and admission as secondary outcomes reported as area under the receiver operating curve (AuROC) scores with 95% confidence intervals (CIs). The sensitivity, specificity, accuracy, predictive values, and likelihood ratios are reported for all models.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 1832 patients were included with 17 (0.9%), 57 (3.1%), and 121 (6.6%) patients dying within 7, 30, and 90 days, respectively. The admission rate was 43% (795/1832). Frailty (CFS > 4) was significantly associated with 30-day mortality (odds ratio 6, 95% CI 3‒12, <i>p</i> < 0.01). Prognostication of 30-day mortality was similar for all CFS-based models and better compared with models without CFS. The AuROC (95% CI) improved for RETTS from 0.67 (0.61‒0.74) to 0.83 (0.79‒0.88) (<i>p</i> = 0.008), for NEWS from 0.53 (0.45‒0.61) to 0.82 (0.77‒0.87) (<i>p</i> < 0.001), and for TEWS from 0.63 (0.55‒0.71) to 0.82 (0.77‒0.87) (<i>p</i> = 0.002).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Frailty measured with the CFS in combination with RETTS or structured vital sign assessment using NEWS or TEWS was better at prognosticating 30-day mortality compared to RETTS or early warnings score alone. Improved prognostication provides more realistic expectations and allows for informed discussions with patients and initiation of individualized treatment plans early in the ED process.</p>\n </section>\n </div>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13244","citationCount":"0","resultStr":"{\"title\":\"Addition of the clinical frailty scale to triage tools and early warning scores improves mortality prognostication at 30 days: A prospective observational multicenter study\",\"authors\":\"Jens Wretborn PhD, Samia Munir-Ehrlington MD, Erika Hörlin MSc, Daniel B. Wilhelms PhD\",\"doi\":\"10.1002/emp2.13244\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>Frailty, assessed with clinical frailty scale (CFS), alone or in combination with aggregated vital signs, has been proposed as a measure to better predict mortality of older patients in the emergency department (ED), but the added predictive value to conventional triage is unclear.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a secondary analysis of a prospective observational study in three EDs in Sweden that evaluated the prognostic performance of the CFS alone or in combination with the national early warning score (NEWS), triage early warning score (TEWS) or the rapid emergency triage and treatment system (RETTS) triage tool using logistic regression. The primary outcome was 30-day mortality with 7- and 90-day mortality and admission as secondary outcomes reported as area under the receiver operating curve (AuROC) scores with 95% confidence intervals (CIs). The sensitivity, specificity, accuracy, predictive values, and likelihood ratios are reported for all models.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 1832 patients were included with 17 (0.9%), 57 (3.1%), and 121 (6.6%) patients dying within 7, 30, and 90 days, respectively. The admission rate was 43% (795/1832). Frailty (CFS > 4) was significantly associated with 30-day mortality (odds ratio 6, 95% CI 3‒12, <i>p</i> < 0.01). Prognostication of 30-day mortality was similar for all CFS-based models and better compared with models without CFS. The AuROC (95% CI) improved for RETTS from 0.67 (0.61‒0.74) to 0.83 (0.79‒0.88) (<i>p</i> = 0.008), for NEWS from 0.53 (0.45‒0.61) to 0.82 (0.77‒0.87) (<i>p</i> < 0.001), and for TEWS from 0.63 (0.55‒0.71) to 0.82 (0.77‒0.87) (<i>p</i> = 0.002).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Frailty measured with the CFS in combination with RETTS or structured vital sign assessment using NEWS or TEWS was better at prognosticating 30-day mortality compared to RETTS or early warnings score alone. Improved prognostication provides more realistic expectations and allows for informed discussions with patients and initiation of individualized treatment plans early in the ED process.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 5\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13244\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13244\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13244","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Addition of the clinical frailty scale to triage tools and early warning scores improves mortality prognostication at 30 days: A prospective observational multicenter study
Objectives
Frailty, assessed with clinical frailty scale (CFS), alone or in combination with aggregated vital signs, has been proposed as a measure to better predict mortality of older patients in the emergency department (ED), but the added predictive value to conventional triage is unclear.
Methods
This was a secondary analysis of a prospective observational study in three EDs in Sweden that evaluated the prognostic performance of the CFS alone or in combination with the national early warning score (NEWS), triage early warning score (TEWS) or the rapid emergency triage and treatment system (RETTS) triage tool using logistic regression. The primary outcome was 30-day mortality with 7- and 90-day mortality and admission as secondary outcomes reported as area under the receiver operating curve (AuROC) scores with 95% confidence intervals (CIs). The sensitivity, specificity, accuracy, predictive values, and likelihood ratios are reported for all models.
Results
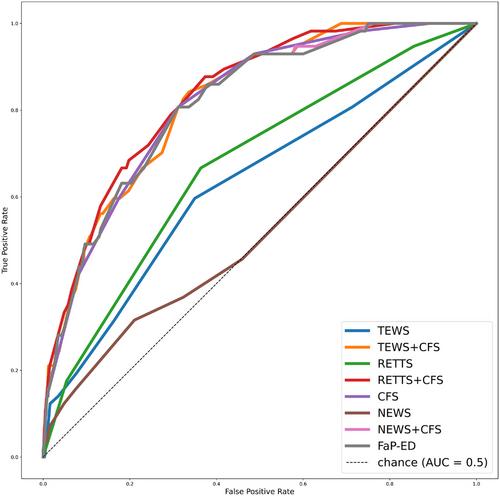
A total of 1832 patients were included with 17 (0.9%), 57 (3.1%), and 121 (6.6%) patients dying within 7, 30, and 90 days, respectively. The admission rate was 43% (795/1832). Frailty (CFS > 4) was significantly associated with 30-day mortality (odds ratio 6, 95% CI 3‒12, p < 0.01). Prognostication of 30-day mortality was similar for all CFS-based models and better compared with models without CFS. The AuROC (95% CI) improved for RETTS from 0.67 (0.61‒0.74) to 0.83 (0.79‒0.88) (p = 0.008), for NEWS from 0.53 (0.45‒0.61) to 0.82 (0.77‒0.87) (p < 0.001), and for TEWS from 0.63 (0.55‒0.71) to 0.82 (0.77‒0.87) (p = 0.002).
Conclusion
Frailty measured with the CFS in combination with RETTS or structured vital sign assessment using NEWS or TEWS was better at prognosticating 30-day mortality compared to RETTS or early warnings score alone. Improved prognostication provides more realistic expectations and allows for informed discussions with patients and initiation of individualized treatment plans early in the ED process.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
