{"title":"头痛的年轻女性","authors":"Megan Hoffer DO, Keith Boniface MD, RDMS","doi":"10.1002/emp2.13287","DOIUrl":null,"url":null,"abstract":"<p>A 42-year-old female presented to the emergency department (ED) with a headache of 2 days’ duration. She reported a low mechanism headstrike without loss of consciousness 2 days prior, as well as a history of idiopathic intracranial hypertension (IIH). She endorsed blurred vision but denied nausea, vomiting, fever, or use of anticoagulation. Point-of-care ultrasound revealed elevated optic discs with crescent signs bilaterally (Figure 1).</p><p> </p><p>A computed tomography scan of the brain was negative for intracranial hemorrhage or mass, but did show sequelae of IIH, including prominent optic nerve sheaths and an empty sella, which had been previously demonstrated on neuroimaging in the medical record. She was offered therapeutic lumbar puncture and neurology evaluation but declined as she was scheduled for ventriculoperitoneal shunt placement with neurosurgery for management.</p><p>Ocular ultrasound is an accessible and noninvasive tool for measuring intracranial pressure (ICP) in the ED, and has been shown to be 90% sensitive in detection of papilledema.<span><sup>1</sup></span> The optic nerve sheath is contiguous with the subarachnoid space and therefore the optic nerve sheath diameter fluctuates with changes in ICP.<span><sup>2-4</sup></span> Crescent sign on point-of-care ultrasound is a hypoechoic ring of subarachnoid fluid surrounding the optic nerve and the presence of a crescent sign has been found to be 92% sensitive for papilledema.<span><sup>5, 6</sup></span> When present, the crescent sign is highly indicative of elevated ICP and warrants neuroimaging and specialty consult to rule out space-occupying lesions or other emergent etiologies of elevated ICP Video 1</p><p>The authors declare no conflicts of interest.</p><p>This is a non-funded study, with no compensation or honoraria for conducting the study.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13287","citationCount":"0","resultStr":"{\"title\":\"Young woman with a headache\",\"authors\":\"Megan Hoffer DO, Keith Boniface MD, RDMS\",\"doi\":\"10.1002/emp2.13287\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 42-year-old female presented to the emergency department (ED) with a headache of 2 days’ duration. She reported a low mechanism headstrike without loss of consciousness 2 days prior, as well as a history of idiopathic intracranial hypertension (IIH). She endorsed blurred vision but denied nausea, vomiting, fever, or use of anticoagulation. Point-of-care ultrasound revealed elevated optic discs with crescent signs bilaterally (Figure 1).</p><p> </p><p>A computed tomography scan of the brain was negative for intracranial hemorrhage or mass, but did show sequelae of IIH, including prominent optic nerve sheaths and an empty sella, which had been previously demonstrated on neuroimaging in the medical record. She was offered therapeutic lumbar puncture and neurology evaluation but declined as she was scheduled for ventriculoperitoneal shunt placement with neurosurgery for management.</p><p>Ocular ultrasound is an accessible and noninvasive tool for measuring intracranial pressure (ICP) in the ED, and has been shown to be 90% sensitive in detection of papilledema.<span><sup>1</sup></span> The optic nerve sheath is contiguous with the subarachnoid space and therefore the optic nerve sheath diameter fluctuates with changes in ICP.<span><sup>2-4</sup></span> Crescent sign on point-of-care ultrasound is a hypoechoic ring of subarachnoid fluid surrounding the optic nerve and the presence of a crescent sign has been found to be 92% sensitive for papilledema.<span><sup>5, 6</sup></span> When present, the crescent sign is highly indicative of elevated ICP and warrants neuroimaging and specialty consult to rule out space-occupying lesions or other emergent etiologies of elevated ICP Video 1</p><p>The authors declare no conflicts of interest.</p><p>This is a non-funded study, with no compensation or honoraria for conducting the study.</p>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 5\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13287\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13287\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13287","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
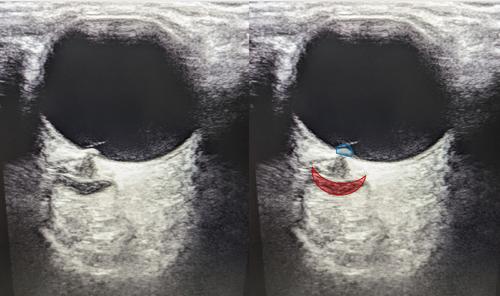
A 42-year-old female presented to the emergency department (ED) with a headache of 2 days’ duration. She reported a low mechanism headstrike without loss of consciousness 2 days prior, as well as a history of idiopathic intracranial hypertension (IIH). She endorsed blurred vision but denied nausea, vomiting, fever, or use of anticoagulation. Point-of-care ultrasound revealed elevated optic discs with crescent signs bilaterally (Figure 1).
A computed tomography scan of the brain was negative for intracranial hemorrhage or mass, but did show sequelae of IIH, including prominent optic nerve sheaths and an empty sella, which had been previously demonstrated on neuroimaging in the medical record. She was offered therapeutic lumbar puncture and neurology evaluation but declined as she was scheduled for ventriculoperitoneal shunt placement with neurosurgery for management.
Ocular ultrasound is an accessible and noninvasive tool for measuring intracranial pressure (ICP) in the ED, and has been shown to be 90% sensitive in detection of papilledema.1 The optic nerve sheath is contiguous with the subarachnoid space and therefore the optic nerve sheath diameter fluctuates with changes in ICP.2-4 Crescent sign on point-of-care ultrasound is a hypoechoic ring of subarachnoid fluid surrounding the optic nerve and the presence of a crescent sign has been found to be 92% sensitive for papilledema.5, 6 When present, the crescent sign is highly indicative of elevated ICP and warrants neuroimaging and specialty consult to rule out space-occupying lesions or other emergent etiologies of elevated ICP Video 1
The authors declare no conflicts of interest.
This is a non-funded study, with no compensation or honoraria for conducting the study.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
