{"title":"急性冠状动脉综合征后常规β-受体阻滞剂治疗:一个时代的终结?","authors":"Nicolas Johner, Baris Gencer, Marco Roffi","doi":"10.1111/eci.14309","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Beta-blocker therapy, a treatment burdened by side effects including fatigue, erectile dysfunction and depression, was shown to reduce mortality and cardiovascular events after acute coronary syndromes (ACS) in the pre-coronary reperfusion era. Potential mechanisms include protection from ventricular arrhythmias, increased ischaemia threshold and prevention of left ventricular (LV) adverse remodelling. With the advent of early mechanical reperfusion and contemporary pharmacologic secondary prevention, the benefit of beta-blockers after ACS in the absence of LV dysfunction has been challenged.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The present narrative review discusses the contemporary evidence based on searching the PubMed database and references in identified articles.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Recently, the REDUCE-AMI trial—the first adequately powered randomized trial in the reperfusion era to test beta-blocker therapy after myocardial infarction with preserved left ventricular ejection fraction (LVEF)—showed no benefit on the composite of all-cause death or myocardial infarction over a median 3.5-year follow-up. While the benefit of beta-blockers in patients with reduced LVEF remains undisputed, their value in post-ACS patients with mildly reduced systolic function (LVEF 41%–49%) has not been studied in contemporary randomized trials; in this setting, observational studies have suggested a reduction in cardiovascular events with these agents. The adequate duration of beta-blocker therapy remains unknown, but observational data suggests that any mortality benefit may be lost beyond 1–12 months after ACS in patients with LVEF >40%.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>We believe that there is sufficient evidence to abandon routine beta-blocker prescription in post-ACS patients with preserved LV systolic function.</p>\n </section>\n </div>","PeriodicalId":12013,"journal":{"name":"European Journal of Clinical Investigation","volume":"54 12","pages":""},"PeriodicalIF":3.6000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14309","citationCount":"0","resultStr":"{\"title\":\"Routine beta-blocker therapy after acute coronary syndromes: The end of an era?\",\"authors\":\"Nicolas Johner, Baris Gencer, Marco Roffi\",\"doi\":\"10.1111/eci.14309\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Beta-blocker therapy, a treatment burdened by side effects including fatigue, erectile dysfunction and depression, was shown to reduce mortality and cardiovascular events after acute coronary syndromes (ACS) in the pre-coronary reperfusion era. Potential mechanisms include protection from ventricular arrhythmias, increased ischaemia threshold and prevention of left ventricular (LV) adverse remodelling. With the advent of early mechanical reperfusion and contemporary pharmacologic secondary prevention, the benefit of beta-blockers after ACS in the absence of LV dysfunction has been challenged.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>The present narrative review discusses the contemporary evidence based on searching the PubMed database and references in identified articles.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Recently, the REDUCE-AMI trial—the first adequately powered randomized trial in the reperfusion era to test beta-blocker therapy after myocardial infarction with preserved left ventricular ejection fraction (LVEF)—showed no benefit on the composite of all-cause death or myocardial infarction over a median 3.5-year follow-up. While the benefit of beta-blockers in patients with reduced LVEF remains undisputed, their value in post-ACS patients with mildly reduced systolic function (LVEF 41%–49%) has not been studied in contemporary randomized trials; in this setting, observational studies have suggested a reduction in cardiovascular events with these agents. The adequate duration of beta-blocker therapy remains unknown, but observational data suggests that any mortality benefit may be lost beyond 1–12 months after ACS in patients with LVEF >40%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>We believe that there is sufficient evidence to abandon routine beta-blocker prescription in post-ACS patients with preserved LV systolic function.</p>\\n </section>\\n </div>\",\"PeriodicalId\":12013,\"journal\":{\"name\":\"European Journal of Clinical Investigation\",\"volume\":\"54 12\",\"pages\":\"\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14309\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Clinical Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/eci.14309\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/eci.14309","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Routine beta-blocker therapy after acute coronary syndromes: The end of an era?
Background
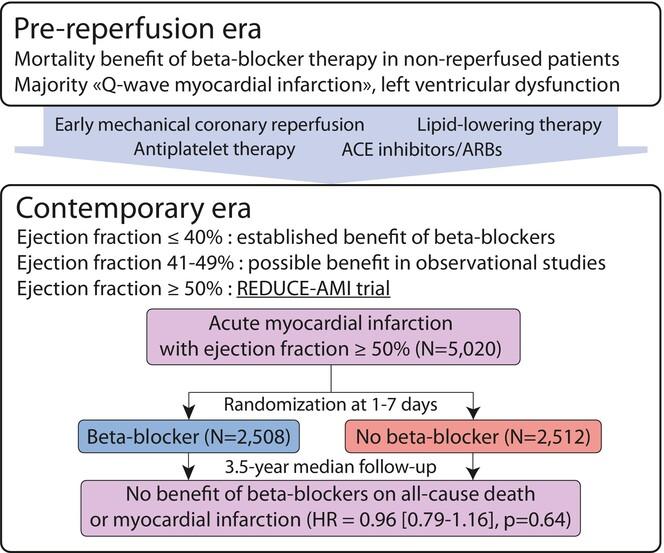
Beta-blocker therapy, a treatment burdened by side effects including fatigue, erectile dysfunction and depression, was shown to reduce mortality and cardiovascular events after acute coronary syndromes (ACS) in the pre-coronary reperfusion era. Potential mechanisms include protection from ventricular arrhythmias, increased ischaemia threshold and prevention of left ventricular (LV) adverse remodelling. With the advent of early mechanical reperfusion and contemporary pharmacologic secondary prevention, the benefit of beta-blockers after ACS in the absence of LV dysfunction has been challenged.
Methods
The present narrative review discusses the contemporary evidence based on searching the PubMed database and references in identified articles.
Results
Recently, the REDUCE-AMI trial—the first adequately powered randomized trial in the reperfusion era to test beta-blocker therapy after myocardial infarction with preserved left ventricular ejection fraction (LVEF)—showed no benefit on the composite of all-cause death or myocardial infarction over a median 3.5-year follow-up. While the benefit of beta-blockers in patients with reduced LVEF remains undisputed, their value in post-ACS patients with mildly reduced systolic function (LVEF 41%–49%) has not been studied in contemporary randomized trials; in this setting, observational studies have suggested a reduction in cardiovascular events with these agents. The adequate duration of beta-blocker therapy remains unknown, but observational data suggests that any mortality benefit may be lost beyond 1–12 months after ACS in patients with LVEF >40%.
Conclusion
We believe that there is sufficient evidence to abandon routine beta-blocker prescription in post-ACS patients with preserved LV systolic function.
期刊介绍:
EJCI considers any original contribution from the most sophisticated basic molecular sciences to applied clinical and translational research and evidence-based medicine across a broad range of subspecialties. The EJCI publishes reports of high-quality research that pertain to the genetic, molecular, cellular, or physiological basis of human biology and disease, as well as research that addresses prevalence, diagnosis, course, treatment, and prevention of disease. We are primarily interested in studies directly pertinent to humans, but submission of robust in vitro and animal work is also encouraged. Interdisciplinary work and research using innovative methods and combinations of laboratory, clinical, and epidemiological methodologies and techniques is of great interest to the journal. Several categories of manuscripts (for detailed description see below) are considered: editorials, original articles (also including randomized clinical trials, systematic reviews and meta-analyses), reviews (narrative reviews), opinion articles (including debates, perspectives and commentaries); and letters to the Editor.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
