Fotini Iatridi, Marieta P. Theodorakopoulou, Areti Georgiou, Artemios G. Karagiannidis, Nasra Haddad, Nikolaos Devrikis, Christopher C. Mayer, Vasileios Kamperidis, Vasileios Anastasiou, Antonios Karpetas, Pantelis Sarafidis
{"title":"透析患者流动血压的性别差异与心血管事件和死亡率的关系","authors":"Fotini Iatridi, Marieta P. Theodorakopoulou, Areti Georgiou, Artemios G. Karagiannidis, Nasra Haddad, Nikolaos Devrikis, Christopher C. Mayer, Vasileios Kamperidis, Vasileios Anastasiou, Antonios Karpetas, Pantelis Sarafidis","doi":"10.1038/s41371-024-00952-z","DOIUrl":null,"url":null,"abstract":"Male patients with pre-dialysis chronic kidney disease (CKD) have worse ambulatory blood pressure (BP) control than females; this is associated with higher mortality. Male hemodialysis patients have higher ambulatory BP levels than females. This analysis aimed to investigate the association of sex differences in ambulatory BP with cardiovascular events and mortality in hemodialysis individuals. 129 male and 91 female hemodialysis patients with valid 48-h BP monitoring were followed for 53.4 ± 31.1 months. The primary endpoint was cardiovascular mortality; the secondary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, resuscitation after cardiac arrest, heart failure-hospitalization, coronary or peripheral revascularization. Cumulative freedom from the primary endpoint was lower for women (logrank-p = 0.032), while cumulative-freedom from the secondary endpoint did not differ significantly between-groups (logrank-p = 0.644). The crude risk for cardiovascular mortality was significantly higher in women (HR = 1.613, 95% CI [1.037, 2.509]). The crude risk for the combined endpoint was not different between the two groups (HR = 0.918, 95% CI [0.638, 1.320]). After adjusting for major risk factors (age, diabetes, dialysis vintage, coronary disease and hemoglobin) no significant differences in the risk for both the primary and the secondary endpoint were observed between women and men (primary: HR = 1.295 (95% CI [0.808, 2.078]), secondary: HR = 0.763 (95% CI [0.521, 1.118])). After additional adjustment for 44-h systolic BP the above relationships did not alter (primary: HR = 1.329 (95% CI [0.826, 2.137]), secondary: HR = 0.808 (95% CI [0.551, 1.184])). In conclusion, female hemodialysis patients have higher crude but similar adjusted cardiovascular mortality rates compared to male counterparts. In contrast to pre-dialysis CKD, the neutral relationship between gender and adverse cardiovascular outcomes in hemodialysis is not further affected by ambulatory BP.","PeriodicalId":16070,"journal":{"name":"Journal of Human Hypertension","volume":"38 12","pages":"789-795"},"PeriodicalIF":3.4000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41371-024-00952-z.pdf","citationCount":"0","resultStr":"{\"title\":\"The association of sex differences in ambulatory blood pressure with cardiovascular events and mortality in dialysis patients\",\"authors\":\"Fotini Iatridi, Marieta P. Theodorakopoulou, Areti Georgiou, Artemios G. Karagiannidis, Nasra Haddad, Nikolaos Devrikis, Christopher C. Mayer, Vasileios Kamperidis, Vasileios Anastasiou, Antonios Karpetas, Pantelis Sarafidis\",\"doi\":\"10.1038/s41371-024-00952-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Male patients with pre-dialysis chronic kidney disease (CKD) have worse ambulatory blood pressure (BP) control than females; this is associated with higher mortality. Male hemodialysis patients have higher ambulatory BP levels than females. This analysis aimed to investigate the association of sex differences in ambulatory BP with cardiovascular events and mortality in hemodialysis individuals. 129 male and 91 female hemodialysis patients with valid 48-h BP monitoring were followed for 53.4 ± 31.1 months. The primary endpoint was cardiovascular mortality; the secondary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, resuscitation after cardiac arrest, heart failure-hospitalization, coronary or peripheral revascularization. Cumulative freedom from the primary endpoint was lower for women (logrank-p = 0.032), while cumulative-freedom from the secondary endpoint did not differ significantly between-groups (logrank-p = 0.644). The crude risk for cardiovascular mortality was significantly higher in women (HR = 1.613, 95% CI [1.037, 2.509]). The crude risk for the combined endpoint was not different between the two groups (HR = 0.918, 95% CI [0.638, 1.320]). After adjusting for major risk factors (age, diabetes, dialysis vintage, coronary disease and hemoglobin) no significant differences in the risk for both the primary and the secondary endpoint were observed between women and men (primary: HR = 1.295 (95% CI [0.808, 2.078]), secondary: HR = 0.763 (95% CI [0.521, 1.118])). After additional adjustment for 44-h systolic BP the above relationships did not alter (primary: HR = 1.329 (95% CI [0.826, 2.137]), secondary: HR = 0.808 (95% CI [0.551, 1.184])). In conclusion, female hemodialysis patients have higher crude but similar adjusted cardiovascular mortality rates compared to male counterparts. In contrast to pre-dialysis CKD, the neutral relationship between gender and adverse cardiovascular outcomes in hemodialysis is not further affected by ambulatory BP.\",\"PeriodicalId\":16070,\"journal\":{\"name\":\"Journal of Human Hypertension\",\"volume\":\"38 12\",\"pages\":\"789-795\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.nature.com/articles/s41371-024-00952-z.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Human Hypertension\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.nature.com/articles/s41371-024-00952-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Human Hypertension","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41371-024-00952-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
摘要
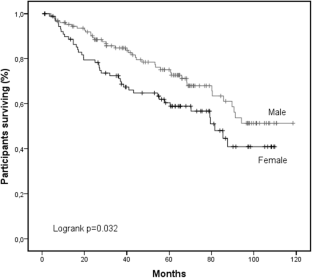
透析前慢性肾病(CKD)男性患者的动态血压(BP)控制比女性患者差;这与死亡率较高有关。男性血液透析患者的动态血压水平高于女性。这项分析旨在研究血液透析患者流动血压的性别差异与心血管事件和死亡率的关系。对 129 名男性和 91 名女性血液透析患者进行了为期 53.4 ± 31.1 个月的有效 48 小时血压监测。主要终点是心血管死亡率;次要终点是心血管死亡、非致死性心肌梗死、非致死性中风、心脏骤停后复苏、心力衰竭住院、冠状动脉或外周血管再通术的复合终点。女性的主要终点累积自由度较低(logrank-p = 0.032),而次要终点累积自由度在组间无显著差异(logrank-p = 0.644)。女性的心血管死亡粗风险明显更高(HR = 1.613,95% CI [1.037,2.509])。综合终点的粗风险在两组之间没有差异(HR = 0.918,95% CI [0.638,1.320])。在对主要风险因素(年龄、糖尿病、透析年限、冠心病和血红蛋白)进行调整后,未观察到女性和男性在一级和二级终点风险方面存在显著差异(一级:HR = 1.295 (95% CI [0.808, 2.078]),二级:HR = 0.763 (95% CI [0.521, 1.118]))。在对 44 h 收缩压进行额外调整后,上述关系没有改变(一级:HR = 1.329 (95% CI [0.826, 2.137]),二级:HR = 0.808 (95% CI [0.551, 1.184]))。总之,女性血液透析患者的粗略心血管死亡率高于男性患者,但调整后的心血管死亡率与男性患者相似。与透析前慢性肾脏病相比,血液透析患者的性别与不良心血管预后之间的中性关系不会受到流动血压的进一步影响。
The association of sex differences in ambulatory blood pressure with cardiovascular events and mortality in dialysis patients
Male patients with pre-dialysis chronic kidney disease (CKD) have worse ambulatory blood pressure (BP) control than females; this is associated with higher mortality. Male hemodialysis patients have higher ambulatory BP levels than females. This analysis aimed to investigate the association of sex differences in ambulatory BP with cardiovascular events and mortality in hemodialysis individuals. 129 male and 91 female hemodialysis patients with valid 48-h BP monitoring were followed for 53.4 ± 31.1 months. The primary endpoint was cardiovascular mortality; the secondary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, resuscitation after cardiac arrest, heart failure-hospitalization, coronary or peripheral revascularization. Cumulative freedom from the primary endpoint was lower for women (logrank-p = 0.032), while cumulative-freedom from the secondary endpoint did not differ significantly between-groups (logrank-p = 0.644). The crude risk for cardiovascular mortality was significantly higher in women (HR = 1.613, 95% CI [1.037, 2.509]). The crude risk for the combined endpoint was not different between the two groups (HR = 0.918, 95% CI [0.638, 1.320]). After adjusting for major risk factors (age, diabetes, dialysis vintage, coronary disease and hemoglobin) no significant differences in the risk for both the primary and the secondary endpoint were observed between women and men (primary: HR = 1.295 (95% CI [0.808, 2.078]), secondary: HR = 0.763 (95% CI [0.521, 1.118])). After additional adjustment for 44-h systolic BP the above relationships did not alter (primary: HR = 1.329 (95% CI [0.826, 2.137]), secondary: HR = 0.808 (95% CI [0.551, 1.184])). In conclusion, female hemodialysis patients have higher crude but similar adjusted cardiovascular mortality rates compared to male counterparts. In contrast to pre-dialysis CKD, the neutral relationship between gender and adverse cardiovascular outcomes in hemodialysis is not further affected by ambulatory BP.
期刊介绍:
Journal of Human Hypertension is published monthly and is of interest to health care professionals who deal with hypertension (specialists, internists, primary care physicians) and public health workers. We believe that our patients benefit from robust scientific data that are based on well conducted clinical trials. We also believe that basic sciences are the foundations on which we build our knowledge of clinical conditions and their management. Towards this end, although we are primarily a clinical based journal, we also welcome suitable basic sciences studies that promote our understanding of human hypertension.
The journal aims to perform the dual role of increasing knowledge in the field of high blood pressure as well as improving the standard of care of patients. The editors will consider for publication all suitable papers dealing directly or indirectly with clinical aspects of hypertension, including but not limited to epidemiology, pathophysiology, therapeutics and basic sciences involving human subjects or tissues. We also consider papers from all specialties such as ophthalmology, cardiology, nephrology, obstetrics and stroke medicine that deal with the various aspects of hypertension and its complications.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
