{"title":"营养学","authors":"","doi":"10.1111/jgh.16706","DOIUrl":null,"url":null,"abstract":"<p><b>20</b></p><p><b>Risk factors for central line-associated bloodstream infections in home parenteral nutrition patients: an observational cohort study</b></p><p>Paris Hoey<sup>1</sup>, Douglas Roche<sup>1</sup>, Paul Chapman<sup>2</sup>, Vishal Kaushik<sup>1</sup>, Stacey Llewellyn<sup>3</sup> and Niwansa Adris<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Department of Infectious Disease, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>QIMR Berghofer Medical Research Institute, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> A central line-associated bloodstream infection (CLABSI) is a common and potentially life-threatening complication for patients with intestinal failure (IF) receiving home parenteral nutrition (HPN). In uncomplicated infections, The European Society for Clinical Nutrition and Metabolism guidelines advocate for central venous access (CVC) salvage for venous access preservation. Existing knowledge regarding the risk factors of HPN-related CLABSIs have been extrapolated from European and North American studies, and the effects of tropical climates and its potentially higher support requirements on the incidence of infection has not yet been studied. We sought to analyse the risk factors of developing HPN-related CLABSI, and assess CLABSI management, in a large Australian state with a highly dispersed population.</p><p><b><i>Methods:</i></b> A retrospective observational cohort study was conducted on 34 adult patients receiving HPN via a CVC at a Queensland tertiary referral centre, between 2016 and 2023. Patient charts were reviewed, and a univariate cox regression analysis model was used to identify predictors of CLABSI in the first CVC. Kaplan-Meier analysis was employed to build survival curves of time to CLABSI, and log-rank tests analysed survival between characteristics.</p><p><b><i>Results:</i></b> Nineteen patients had ≥1 CLABSI(s), accounting for a total of 39 episodes. Patients with ≥1 CLABSI(s) used regular opioids more than those who did not develop CLABSI (p=0.016). Fourteen patients (41%, n=14/34) developed a CLABSI in their first CVC. No patient or line characteristics, including tropical climate, were found to be predictive of CLABSI in their first CVC. The overall infection rate was 1.02 per 1000 catheter days. Most CLABSIs were caused by <i>Enterobacterales</i> (22%, n=12/55), followed by coagulase-negative <i>Staphylococcus</i> (18%, n=10/55). Administration of empiric antimicrobials within the standardised 3-hour sepsis timeframe was inadequate (50%, n=14/28), with only 25% (n=7/28) providing adequate cover of causative pathogens. The median time to effective antibiotic therapy was 22.7 hours (IQR 4.8-29.8). There were 3 CVC salvages (8%, n=3/39), all of which were successful.</p><p><i><b>Conclusion:</b></i> In this cohort of patients, regular opioid use was associated with an increased risk of developing CLABSI which is consistent with international studies. We also found a low CVC salvage rate in our cohort, representing potential missed opportunities for venous access preservation. Based on our findings, an empiric antimicrobial regime of vancomycin, cefepime and caspofungin for all HPN-related CLABSI cases would be expected to be effective for 84.6%. We recommend that Australian IF units with a similar antimicrobial distribution and resistance pattern adopt this regime.</p><p><b>28</b></p><p><b>Evaluating quality of life in patients who use home enteral nutrition in Australia/New Zealand</b></p><p><b>Mercedez Hinchcliff</b> and <b>Sarah Gray</b></p><p><i>University Of Wollongong, Wollongong, Australia</i></p><p><b><i>Background and Aim:</i></b> Home enteral nutrition (HEN) involves providing nutritional support to a person at home, orally or via a feeding tube into their stomach or intestines (1). While existing research primarily focuses on the clinical aspects of HEN (2, 3), there is a gap in the research from the patient perspective. The study aims to delve into various facets of HEN via tube feeding, with a particular emphasis on the financial and psychological burdens from a patient/carer perspective. We also aim to evaluate the societal stigma associated with tube feeding and its impact on patient experience.</p><p><b><i>Methods:</i></b> We adopted a mixed-method approach, disseminating an online anonymous questionnaire to patients and carers across Australia and New Zealand via collaborations with various support organizations. The questionnaire was formulated and adapted from NutriQol and HRQoL scales, supplemented with items to assess community and family support and open-ended questions to identify gaps in care.</p><p><b><i>Results:</i></b> The survey yielded 158 responses, comprising 91 from carers (both paediatric and adult) and 67 from adults who use HEN. Among the respondents, 47% reported receiving no government financial support (e.g., carer’s payment, health care cards), while 41% spent over $200 monthly on supplies. Most patients reported co-morbid conditions necessitating HEN, with the most prevalent diagnoses including dysphagia, failure to thrive (paediatric), gastroparesis, GERD/reflux, oral aversions, and eosinophilic oesophagitis (EoE). The beneficial implications of tube feeding are noteworthy, with 73% of adults reporting an enhanced sense of health and 80% feeling well-nourished. However, social concerns were evident, with numerous respondents limiting social engagements involving food. For paediatric respondents or their carers, the results were more positive, suggesting a higher level of acceptance of tube feeding among children and adolescents compared to adults. The majority did not attempt to hide their feeding tubes from friends nor feeling excluded. Only 22% of paediatric respondents experienced anxiety or depression, significantly lower than adults, potentially attributable to robust parental support. Despite these positive outcomes, both paediatric and adult respondents experienced physical discomfort (71%) and skin irritation (60%) from tube feeding.</p><p><b>79</b></p><p><b>Has ulcerative colitis been forgotten: what are the energy and protein requirements of adults with ulcerative colitis? A systematic scoping review</b></p><p><b>Samantha Plush</b><sup>1,2,3</sup>, Robert Bryant<sup>1,2,3</sup>, Rachel Davis<sup>1,2,3</sup>, Saravana Kumar<sup>4</sup> and Alice Day<sup>1,2,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>2</sup><i>The School of Medicine, University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>The Basil Hetzel Institute, Adelaide, Australia;</i> <sup>4</sup><i>Allied Health and Health Services, University of South Australia, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Ulcerative colitis (UC) affects only the colonic mucosa whereas Crohn’s disease (CD) is transmural and can involve any gastrointestinal segment. Nutritional requirements for these distinct diseases likely differ depending on location, inflammatory burden, and catabolism. Yet, energy and protein prescription recommendations for UC are largely extrapolated from CD studies. The aim of this scoping review was to evaluate the evidence for energy and protein prescription in adults with UC.</p><p><b><i>Methods:</i></b> Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews methodology was used. The search strategy identified key words including ulcerative colitis, inflammatory bowel disease, nutrition requirements, energy expenditure, indirect calorimetry, protein, and nitrogen balance. The search was conducted until April 2024 from EMBASE, EMCARE, MEDLINE and CINAHL databases. Full text citations were assessed against predefined inclusion and exclusion criteria by two reviewers. Data extraction was completed into predefined data extraction tables.</p><p><b><i>Results:</i></b> Of 9730 studies, 236 studies were eligible for full text screening. Thirteen studies evaluating 150 patients (92 male) were included. Measuring resting energy expenditure (mREE) via indirect calorimetry identified requirements increased in quiescent disease compared with active disease (Table 1). Doubly labelled water investigations found a difference between resting and total energy expenditure of 19.9 ± 7.27 kcal/kg/day in UC in clinical remission. Protein requirements of 1.24-1.4 g/kg/day in acute severe UC were needed to achieve nitrogen balance (Kjeldahl method) (Table 1). There were no data informing protein requirements in quiescent or mild to moderate UC.</p><p><b>98</b></p><p><b>Roux en Y jejunostomy in gastroparesis: insight into patient perspectives and outcomes</b></p><p><b>Omar Salehi</b><sup>1</sup>, Weilun Gao<sup>1</sup>, Christian Kenfield<sup>2</sup> and Geoffrey Hebbard<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Royal Melbourne Hospital, Parkville, Australia;</i> <sup>2</sup><i>Department of General Surgery, Melbourne Private Hospital, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastroparesis is a debilitating condition with patients sometimes requiring long-term enteral nutrition. Leakage, pain and social stigma may negatively impact quality of life in this patient cohort. This study aimed to explore patient experience post insertion of a jejunostomy with a Roux-en-Y anastomosis, a laparoscopic technique previously described in the pediatric population to reduce leakage and improve enteral feed tolerability, in 7 adult patients with idiopathic gastroparesis.</p><p><i><b>Methods:</b></i> Seven patients (6 female, 1 male) were interviewed about their experiences pre-and post-procedure up to 2 years. All had previously used other feeding tubes including nasogastric, nasojejunal and percutaneous endoscopic gastrostomy tubes. The patients were retrospectively surveyed for symptoms, nutrition, complications, day-to-day life, and satisfaction with the Roux en Y jejunostomy compared to previous feeding tubes.</p><p><b><i>Results:</i></b> Post-procedure, patients reported improvements in nausea (7/7; 100%), vomiting (6/7; 85.7%), and abdominal pain (6/7; 85.7%). Weight stabilized and oral intake improved in 57.1% (4/7) of patients. Most (6/7; 85.7%) described improved social confidence, increased energy, and better work/school functioning. One patient (1/7; 14.3%) experienced severe abdominal pain post-procedure, leading to jejunostomy removal. Minor leakage occurred in 42.9% (3/7) of cases. Despite challenges, most (6/7; 85.7%) patients preferred the Roux en Y jejunostomy over previous feeding tubes and stated they would undergo the procedure again.</p><p><b>140</b></p><p><b>Additive content of Australian oral nutrition supplements</b></p><p><b>Emily Monro</b><sup>1</sup>, <b>Erin Russell</b><sup>2,3</sup> and Jessica Fitzpatrick<sup>4</sup></p><p><sup>1</sup><i>NSW Health, Australia;</i> <sup>2</sup><i>St Vincent's Hospital Melbourne, Australia;</i> <sup>3</sup><i>University of Melbourne, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, School of Translational Medicine, Monash University</i></p><p><b><i>Background and Aim:</i></b> Pre-clinical and some observational studies have implicated ultra-processed foods (UPF), specific emulsifiers, thickeners, and artificial sweeteners in the pathogenesis of inflammatory bowel disease (IBD). Oral nutrition supplements (ONS) are UPFs, and commonly utilised in IBD for nutritional support, exclusive enteral nutrition (EEN) or the Crohn’s disease exclusion diet (CDED). With this paradox, we examine the reported deleterious food additive composition of ONS currently available in Australia.</p><p><b><i>Methods:</i></b> Current ingredient composition was sourced from all national suppliers (Nutricia, Fresenius Kabi, Nestle and Abbott). Standard adult and paediatric formulas were included and disease specific formulations were excluded. All additives were classed according to the Food Standards Australia New Zealand E numbers. Additives of interest were those reported to be deleterious to gut health including artificial sweeteners, maltodextrins, sulphites, titanium dioxide, and emulsifiers/thickeners (namely lecithin, gums, polysorbate 80, polyphosphates, carboxymethylcellulose, carrageenan, other mono and diglycerides of fatty acids) as these have been implicated in preclinical studies. Results are presented as mean ± standard deviation.</p><p><b><i>Results:</i></b> Forty-six oral supplements were reviewed. All products contained additives (any E number), with a minimum 5 and maximum 21 additives per supplement (Mean 12.8 ± 3.4). Of note, some of these appear to be for micronutrient provision. Specific to additives considered deleterious to gut health (listed above), the ONS had a mean 2.37 ± 1.39 additives per supplement (Figure 1). Maltodextrin was in 64% of products, with 40% (n=18) using maltodextrin as the primary carbohydrate source. Artificial sweeteners were in 6% (n=3), which were all milk-based products. Titanium dioxide, sulphites and polysorbate 80 were not found in any product. In terms of emulsifiers of interest, the supplements contained a mean 1.95 ± 1.0 per product. Specifically, 21% (n=10) contained carboxymethylcellulose, 15% (n=7) contained carrageenan and 72% (n=33) contained lecithin.</p><p><b>142</b></p><p><b>An exploration of nutrition and metabolic risk factors in non-alcoholic fatty liver disease and related cirrhosis</b></p><p><b>Catherine Stankevicius</b><sup>1,2,4</sup>, Rachel Davis<sup>2,4</sup>, Alison Yaxley<sup>1</sup>, Dep Huynh<sup>3</sup>, Martine Hatzi<sup>2</sup> and Alice Day<sup>2,4</sup></p><p><sup>1</sup><i>College of Nursing and Health Sciences, Flinders University, Bedford Park, Australia;</i> <sup>2</sup><i>Nutrition and Dietetics Department, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>3</sup><i>Gastroenterology and Hepatology Department, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>4</sup><i>Basil Hetzel Institute for Translational Health Research, Woodville South, Australia</i></p><p><b><i>Background and Aim:</i></b> Incidence of non-alcoholic fatty liver disease (NAFLD) is rising. Risk factors for progression to cirrhosis include obesity (over nutrition), type 2 diabetes (T2DM), and westernised diets. Paradoxically, sarcopenia and malnutrition (under nutrition), accelerate disease progression. Clinical guidelines for liver disease recommend early allied health intervention to slow disease progression. This study aimed to determine modifiable nutrition and metabolic risk prevalence in a South Australian outpatient hepatology service without allied health integration for NAFLD and related cirrhosis.</p><p><b><i>Methods:</i></b> This cross-sectional study used convenience sampling between July and November 2023. Malnutrition universal screening tool score (MUST ≥2) defined risk while subjective global assessment (SGA, scores of B or C) diagnosed malnutrition. Sarcopenia risk was defined by the SARC-F questionnaire (score of ≥4). Anthropometrics included waist circumference and body mass index (BMI). Previous allied health interventions were assessed. Habitual diet was scored against a Mediterranean diet index (MED-Score).</p><p><b><i>Results:</i></b> Thirty-two participants consented to participate (median age 63 (Interquartile range (IQR) 55.5-70.8) years; 44% male). Table 1 summarises the cardiometabolic and nutrition risks. Prevalence of sarcopenia and malnutrition risk was low (median SARC-F scores=1 (IQR 0-2), and all had MUST >2. Three (9.4%) participants were malnourished (SGA B). Fifteen participants (46%) had been referred to a dietitian previously.</p><p><i><b>Conclusion:</b></i> Modifiable nutrition or metabolic risk factors in NAFLD and associated cirrhosis were prevalent, but can be optimised with diet and lifestyle intervention. Establishing tertiary referral pathways from Hepatology services to allied health is essential to manage modifiable risk factors to improve patient outcomes.</p><p><b>190</b></p><p><b>High Mediterranean diet adherence reduces risk of cancer and improves cancer survivorship</b></p><p><b>Daniel Clayton-chubb</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>1,2</sup>, Andrew T Chan<sup>3</sup>, Elena George<sup>4</sup>, Alex Boussioutas<sup>1,2</sup>, John McNeil<sup>2</sup>, Robyn Woods<sup>2</sup>, Alice Owen<sup>2</sup>, William Kemp<sup>1,2</sup>, Ammar Majeed<sup>1,2</sup> and Stuart Roberts<sup>1,2</sup></p><p><sup>1</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>2</sup><i>Monash University, Melbourne, Australia;</i> <sup>3</sup><i>Harvard Medical School, Boston, USA;</i> <sup>4</sup><i>Deakin University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> While a Mediterranean diet (MedDiet) is commonly recommended in primary and specialist care, yet its role in reducing the risk of cancer, gastrointestinal (GI) cancer and improving cancer survivorship is understudied especially in older adults. As such, we aimed to determine whether MedDiet adherence (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with incident cancer, incident GI cancer, and survivorship in older Australian adults.</p><p><b><i>Methods:</i></b> This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, which enrolled 12,581 participants. A MedDiet Score (MDS) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 18. Higher scores indicate greater adherence to a MedDiet style dietary pattern. Cancer incidence and sub-type were adjudicated by investigators based on medical records. Participants with cancer diagnosed during ASPREE prior to completion of the FFQ were excluded. GI cancer was defined as colorectal, gastric, gastro-oesophageal, liver, or pancreatic in origin. MDS was analysed in quartiles due to its non-linear association with incident GI cancer. Both unadjusted and adjusted cox regression were used in these analyses.</p><p><b><i>Results:</i></b> We included the 12,394 participants (median 76.8 [IQR 74.6 – 80.3] years) who answered a semi-quantitative FFQ while living at home/with family during ALSOP. Of these, 563 (4.5%) developed cancer during ASPREE but pre-questionnaire and were excluded and 10 had incomplete data. The remaining 11,831 were subsequently followed up for a median of 5.8 (IQR 4.6 – 6.5) years. Of these 11,4831, 1629 (13.8%) developed cancer, of which 344 (2.9% overall) were GI cancers. The mean (± SD) MDS was 11.1 (± 2.0). Univariate analysis showed higher adherence to a MedDiet was associated with a reduced hazard of all cancer (Q4 vs Q1 HR 0.71 [95% CI 0.62 – 0.81]) and GI cancer specifically (Q4 vs Q1 HR 0.70 [95% CI 0.51 – 0.95]) (Figure 1). Results remained significant for all cancer when adjusting for age, sex, BMI, alcohol and smoking status, ethnicity, diabetes, aspirin use, education, and participant history of cancer pre-dating ASPREE (all cancer Q1 vs Q4 aHR 0.85 [95% CI 0.74 – 0.99] but not GI cancer Q1 vs Q4 aHR 0.82 [95% CI 0.60 – 1.13]). In those who developed cancer, higher MDS was associated with reduced all-cause mortality (Q4 vs Q1 aHR 0.73 [95% CI 0.56 – 0.96]), though not in the GI cancer subgroup (Q4 vs Q1 aHR 0.87 [95% CI 0.53 – 1.43]).</p><p><b>191</b></p><p><b>Ultra-processed food is associated with death and dementia in older Australian adults</b></p><p><b>Daniel Clayton-chubb</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>1,2</sup>, Priscila Machado<sup>4</sup>, William Kemp<sup>1,2</sup>, Alice Owen<sup>2</sup>, John McNeil<sup>2</sup>, Robyn Woods<sup>1,2</sup>, Joanne Ryan<sup>1,2</sup>, Ammar Majeed<sup>1,2</sup>, Andrew T Chan<sup>3</sup> and Stuart Roberts<sup>1,2</sup></p><p><sup>1</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>2</sup><i>Monash University, Melbourne, Australia;</i> <sup>3</sup><i>Harvard Medical School, Boston, USA;</i> <sup>4</sup><i>Deakin University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> There is a growing body of evidence linking high Ultra-Processed Foods (UPFs) intake with deleterious health outcomes, including mortality and cognitive dysfunction. However, there are less data on the risks of high UPF intake in older adults. As such, we aimed to determine whether a high UPF diet (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with mortality or incident dementia in older Australian adults.</p><p><b><i>Methods:</i></b> This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, with 12,581 respondents. A UPF Diet Score (UPFQ) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 25. Higher scores indicate greater exposure to UPFs. Mortality and incident dementia were adjudicated by investigators based on medical records. Participants with dementia diagnosed during ASPREE prior to completion of the FFQ were excluded in dementia analyses, as were those with more than 20% missing UPF FFQ data. UPFQ was analysed in quartiles due to its non-linear association with all-cause mortality, and linearly for incident dementia. The nadir quartile was used as the reference for Cox models.</p><p><b><i>Results:</i></b> We included the 11,962 participants living home alone or with family (median [IQR] 76.8 [74.6 – 80.2] years) who adequately answered the FFQ during ALSOP. This group was followed up for a median of 5.9 (IQR 4.7 – 6.6) years. Of the included participants, 1,349 (11.3%) died. Sixty-six developed dementia pre-FFQ (0.6%) and were excluded from dementia analyses. The median (IQR) UPFQ was 6 (4.9 – 7.3). Univariate Cox Proportional Hazards Models showed higher UPF intake was associated with an increased hazard of all-cause mortality (Q4 vs Q2 HR 1.47 [95% CI 1.26 – 1.71]) and dementia (HR 1.09 [95% CI 1.04 – 1.14]). Results remained significant for mortality when adjusting for sex, BMI, age, smoking status, diabetes, renal function, cognitive function, depression, education, grip strength and gait speed (Q4 vs Q2 aHR 1.31 [95% CI 1.12 – 1.55]). Similarly, when fully adjusted, for every one-point increase in UPFQ there was an increased risk of dementia (aHR 1.08 [95% CI 1.03 – 1.14]). The increase in mortality impacted cardiovascular death (including stroke), cancer death, and other causes similarly (χ2 <i>p</i>-value = 0.687). Results remained significant when excluding those with less than 12 months of follow-up.</p><p><b>195</b></p><p><b>Quality over quantity: How can the quality of therapeutic diets be assessed for inflammatory bowel disease in Australia?</b></p><p><b>Laura Portmann</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>3,4</sup>, Emma Halmos<sup>3,4</sup>, Robert Bryant<sup>1,2,5</sup> and Alice Day<sup>1,2,5</sup></p><p><sup>1</sup><i>The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>2</sup><i>Basil Hetzel Institute, Woodville South, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia;</i> <sup>4</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>5</sup><i>The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Examining the quality of diets used to treat inflammatory bowel disease (IBD) is challenging as traditional dietary analysis methods are used to quantitatively assess food group and nutrient intakes, not overall diet quality. Yet, evidence is suggesting dietary patterns of differing quality such as ultra-processed foods or the Mediterranean diet (MED), rather than specific food components may be more predictive of disease onset and course. An IBD-specific diet quality index (DQI) does not exist. It is therefore unknown which DQI is most suitable to use in therapeutic IBD diet trials. This review aimed to identify current DQIs and assess their suitability for use on therapeutic diets in an Australian IBD population.</p><p><b><i>Methods:</i></b> Electronic databases, MEDLINE and EmCare, were systematically searched for a-priori, food-based DQI reflecting national dietary guidelines and/or latest nutrition science for adults published 2013 to 2023, in English language. Excluded were DQI that were posteriori or for specific, non-IBD diseases (e.g., diabetes). Data extracted were adapted from optimal DQI criteria described by Burggraf et al.,<sup>1</sup> which include quality measures of adequacy, moderation, variety and balance for food and nutrient components and DQI evaluation, as well as its use, if any, for IBD health outcomes.</p><p><b><i>Results:</i></b> Twenty-five articles describing 25 DQI were included in final analysis. Sixteen DQI were adapted from existing DQI. Dietary guidelines were used to develop 19/25 (76%) DQI, while the remaining six were developed from dietary patterns (e.g., MED, EAT-Lancet Diet). Whole food groups were assessed by all DQI, but assessment of individual foods within groups varied. Ultra-processed foods were assessed in 16/25 (64%) DQI. No DQI included all optimal DQI criteria<sup>1</sup>. The Dietary Guideline Index 2013 (DGI-2013) most closely met DQI criteria, followed by the Healthy Eating Index for Australian Adults-2013 (HEIFA-2013) (Table 1). Seven of 25 DQI were Australian population specific. All Australian DQI evaluated adequacy, however assessment of other quality dimensions and scoring methods varied as outlined in Table 1. All except one Australian DQI were applied to food frequency questionnaires (FFQ). Eleven of 25 (44%) DQI, yet only two Australian DQI were not weighted equally to account for different weighted contributions of foods and nutrients to established health and disease outcomes. Seventeen of 25 (68%) DQI were validated, however few were evaluated for reproducibility (2/25) or reliability (7/25). No DQI was validated to assess gut-specific health outcomes. Two DQI (Dietary Diversity Score and Australian Recommended Food Score (ARFS)) were used to assess against gut microbiota. The DGI-2013 and Dutch Healthy Diet index-2015 were applied to FFQ from various IBD participants.</p><p><b>Reference</b></p><p>\n 1. <span>Burggraf, C.</span>, <span>Teuber, R.</span>, <span>Brosig, S.</span>, & <span>Meier, T.</span> (<span>2018</span>). <span>Review of a priori dietary quality indices in relation to their construction criteria</span>. <i>Nutrition reviews</i>, <span>76</span>(<span>10</span>), <span>747</span>-<span>764</span>.</p><p><b>206</b></p><p><b>Systematic scoping review: dietary interventions for the treatment of primary sclerosing cholangitis</b></p><p><b>Caitlin Theron</b><sup>1,2</sup>, Robert Bryant<sup>1,2</sup>, Damjana Bogatic<sup>1,2</sup> and Alice Day<sup>1,2</sup></p><p><sup>1</sup><i>The Queen Elizabeth Hospital Gastroenterology Department, Adelaide, Australia;</i> <sup>2</sup><i>Basil Hetzel Institute, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Primary sclerosing cholangitis (PSC), is a rare autoimmune liver disease with no effective medical therapies. The etiopathogenesis of PSC is incompletely understood, however evolving evidence suggests dysbiosis of the gut microbiota may play a key role. Diet is an important fertiliser of gut microbiota and has potential to be a modifiable risk factor in PSC. This review aims to scope available evidence of dietary factors that may influence PSC disease course.</p><p><b><i>Methods:</i></b> A systematic scoping search of electronic databases EMBASE, EMCARE, MEDLINE and CINAL was carried out. Key search terms included primary sclerosing cholangitis, diet, nutrition, therapy, and gut microbial diversity. Included articles were original, peer-reviewed research and case reports, both human and pre-clinical models, that produced evidence of a diet or nutrient that contributed any effect to disease stabilisation, progression, symptoms, gut microbes, or survival rate associated with PSC.</p><p><b><i>Results:</i></b> Of 1466 articles screened, 15 were included for review including four pre-clinical PSC models and 13 in humans. Outcome measures varied across studies, however most (8/15, 53%) assessed a change in biochemical parameters associated with poor patient outcomes, as outlined in Table 1. In human studies, the addition of retinoic acid for patient’s taking ursodeoxycholic acid (UDCA) was the only intervention found to significantly change one of the liver function tests, causing a reduction in alanine transferase (ALT). In mouse models of PSC, geniposide and berberine significantly reduced alkaline phosphatase (ALP), aspartate aminotransferase (AST) and ALT. No other interventions were found to significantly alter biochemical parameters. Survival rates were increased by coffee in patients with PSC (p=0.02), and by vitamin D in a PSC mouse model (p=0.01). Regarding symptoms, pruritis and abdominal pain were improved by N-acetylcysteine (p value not reported), while dietary fiber had no significant effect on pruritus (p value not reported). Only one article examined the effect of the intervention on the gut microbiome, finding that berberine reduced gut permeability (p<0.001), increased <i>Bacteroidetes</i> and decreased <i>Firmicutes</i> (p values not reported).</p><p><b><i>Conclusion:</i></b> There are limited well designed clinical trials and data evaluating diet in PSC disease course. Of existing evidence, few dietary interventions significantly altered biochemical parameters associated with disease progression, including retinoic acid, geniposide and berberine. Only one article provided data on the relationship between the dietary factor, the gut microbiome and PSC disease course. Further research should include well-designed clinical trials that investigate the role of dietary factors in disease progression and the role of diet as a microbial restoration therapy.</p><p>\n \n </p><p><b>223</b></p><p><b>Practical application of evidence-based dietary therapy into inflammatory bowel disease care shows high patient satisfaction and compliance, and improved disease activity: The DELECTABLE program</b></p><p><b>Gina Trakman</b><sup>1,2,3</sup>, Erin Russell<sup>1,2</sup>, Amy Hamilton<sup>1,2</sup>, Amy Wilson-o'brien<sup>1,2</sup>, Emily Thompson<sup>1</sup>, Natalie Simmance<sup>1</sup>, Ola Niewiadomski<sup>1</sup> and Michael Kamm<sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>La Trobe University, Melbourne, Australia</i></p><p><b><i>Background and aims:</i></b> A range of diets have been shown in controlled trials to be therapeutically effective in Inflammatory Bowel Diseases (IBD). Exclusive enteral nutrition (EEN) and the Crohn’s Disease Exclusion Diet (CDED) have confirmed efficacy in inducing remission in Crohn’s disease (CD). Low sulphur and plant-based diets are being investigated in ulcerative colitis (UC). Reducing ultra-processed, additive-containing food intake is emerging as important, given its role in initiating and perpetuating disease. IBD patients believe in the value of modifying diet to improve disease control. Yet there is no evidence for diet tolerability and benefit outside clinical trials. The DELECTABLE program, a dietitian-led telehealth service, aimed to evaluate the patient acceptability, compliance, and benefit of structured, evidence-based dietary therapy as part of routine clinical care.</p><p><i><b>Methods</b>:</i> In this open-label, prospective, interventional cohort program, patients with Crohn’s disease or an ileo-anal pouch were offered the CDED or a wholefood additive-free diet (WFD), patients with ulcerative colitis were offered a low-sulphur plant-based diet (UCD) or WFD, and patients with microscopic colitis were offered the WFD. The primary outcomes were diet satisfaction (modified DSAT-28: range 27 to 135), dietitian-rated compliance (range 1-6), and patient-rated compliance (range 1 -5). Secondary outcomes were the amount of food additive intake (validated food frequency questionnaire), quality of life (IBDQ9; range 7-49), disease activity score (CDAI in CD, partial Mayo score in UC), CRP, and faecal calprotectin. Baseline to Week 12 differences were assessed for the CDED and wholefood diet using the Paired T-test or Wilcoxon-sign-test. Inferential statistics were not conducted for disease activity on the UCD due to sample size.</p><p><b><i>Results:</i></b> Of 165 patients referred, 76 enrolled in the program. Sixty-four (82%) (mean age 36; 53% male) of enrolled patients completed 12 weeks of diet therapy, with 15, 42 and 7 participants completing the CDED, WFD, and UCD, respectively. Diet satisfaction was high at Week 1 on CDED (median 79 out of 135) and did not significantly change at Week 12 (median 83 out of 135, P=0.212). Diet satisfaction improved on the WFD from Week 1 to 12 (84.1 vs 86.9, P = 0.03) (Figure 1, Panel B). Median dietitian-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/6 v 4/6, P=0.682; WFD: 3/5 vs 3/5, P=0.165; UCD: 4/6 vs 4/6, P=0.233). Likewise, median patient-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/5 v 4/5, P=0.565; WFD: 4/5 vs 4/5, P=0.348; UCD: 4.5/5 vs 4/5, P=0.368) (Figure 1, Panel B). Quality of life increased from Week 1 to Week 12 on the CDED (35 vs 51, P<0.001) and the WFD (37.1 vs 48.3, P<0.001). With regard to food additive ingestion: on the WFD, there was a significant reduction in carboxymethylcellulose (P=0.02), carrageenan (P=0.013), sucralose (P=0.018) and sulphites (P=0.007) ingestion. On the UCD there was a significant reduction in daily intake of all food additives (aspartame P=0.043; others P <0.028). On the CDED, from baseline to Week 12, there was a reduction in CRP (7.5 vs 4.6, P=0.034), calprotectin (195 vs 62, P=0.045) and CDAI (153 vs 43, P=0.023). On the WFD from baseline to Week 12, there was a significant reduction in CDAI (50 vs 32, P= 0.027) and partial Mayo score (2 vs 0, P=0.004). On the UCD, there was no change from baseline to Week 12 CRP (0 vs 1), partial Mayo score (3 vs 3) or calprotectin (112 vs 174).</p><p><b><i>Conclusion:</i></b> Implementation of well-balanced, effective diet therapies is feasible and well-accepted by patients with IBD, with a promising impact on disease activity.</p><p><b>255</b></p><p><b>Peripheral parenteral nutrition: an evaluation of utility and complications</b></p><p><b>Emma Bidgood</b><sup>1</sup>, Joanna Huang<sup>2</sup>, Elise Murphy<sup>3</sup>, Ralley Prentice<sup>4</sup>, Beth Hede<sup>2</sup> and David Russell<sup>2,5</sup></p><p><sup>1</sup><i>Department of Allied Health (Clinical Nutrition), The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>2</sup><i>Department of Gastroenterology, The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>3</sup><i>Pharmacy Department, The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Monash Medical Centre, Clayton, Australia;</i> <sup>5</sup><i>Department of Medicine, Melbourne Medical School, The University of Melbourne, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Peripheral parenteral nutrition (PPN) provides an alternative nutrition support strategy to centrally administered parenteral nutrition (PN) for specific patients requiring short-term PN. Previous studies have demonstrated limited utilization of PPN and variations in complication rates. This study aimed to evaluate PPN complications and usage at this center.</p><p><b><i>Methods:</i></b> This was a single-center retrospective observational study of all adult patients who received at least 1 day of PPN from June 2018 to December 2023. Demographic and clinical data were collected including, complications, indications for PN and reason for PPN, duration of therapy, reason for cessation of PPN, nutritional status, energy and protein provision and central line insertion rates.</p><p><b><i>Results:</i></b> A total of 381 patients were included, median age 62 [IQR 28-74] years, 235 males (61.7%). The most common indication for PN was ileus (n=153, 40%), followed by gastrointestinal obstruction (n=93, 24%). The median time on PPN was 3 [2-4] days. Patients received a median of 65% [55-75] of energy and 58% [50-69] of protein requirements with PPN. Malnutrition was diagnosed in 47.5% (n=181) of this cohort. Total complication rates were 8.7% (n=33) with cannula infiltration being the most common complication (6.6%, n=25). 213 (56%) patients proceeded to central line insertion.</p><p><b><i>Conclusion</i></b>: PPN proved to be a safe and effective therapy for short-term PN when managed by a nutrition support team. PPN has the potential to attenuate short-term nutritional deficits and prevent CVAD insertion in selected patients, making it a valuable therapy in type 1 intestinal failure.</p><p><b>260</b></p><p><b>Low salt diet modifiers may not be necessary for all inpatients with liver cirrhosis</b></p><p><b>Annie Shanahan</b><sup>1</sup>, Stacey Sayers<sup>1</sup>, Nicole Barna<sup>1</sup>, Alison Stewart<sup>1</sup>, Kelly Ho<sup>2</sup>, Georgina Petrusma<sup>2</sup>, Veronika Pudikova<sup>2</sup>, Angela Taylor<sup>2</sup>, Qinfang Yang<sup>2</sup>, Han Yu<sup>2</sup> and Erin Russell<sup>1</sup></p><p><sup>1</sup><i>Department of Nutrition and Dietetics, Monash Health, Australia;</i> <sup>2</sup><i>Department of Nutrition, Dietetics and Food, Monash University, Australia</i></p><p><b><i>Background:</i></b> An order for a high energy, high protein, low salt (HEHPLS) diet is common practice to support inpatients with liver cirrhosis. However, evidence suggests that a low salt (LS) diet can reduce palatability and hinder energy and protein intake in this patient group with increased nutrient needs. International guidelines recommend a ‘moderate’ daily salt restriction (1840-2760mg) for these patients. Clinicians were concerned that the LS diet modifier was unnecessarily limiting meal options. Automated oral nutrition supplements (ONS) are being considered. Therefore, a review of the energy, protein and sodium content of diet codes HEHPLS and high energy, high protein (HEHP) was conducted and compared with established clinical guideline reference ranges.</p><p><b><i>Methods:</i></b> In September 2023, six dietetics students undertook a detailed menu review. Both the 28-day cycle cook-chill and the 7-day frozen meal ‘Smart Pack’ menus at our hospital network were reviewed. To ensure all menu options were captured, the full menu cycle was analysed on the online menu system by selecting three main meals and two snacks per day. A variety of meals and snacks were selected to reflect a typical choice of a patient across the days of the menus. Energy, protein and sodium content was then averaged. Results therefore reflect nutrition provision to patients, rather than actual patient consumption. Requirements of a ‘reference patient’ with BMI 25 and decompensated liver cirrhosis was utilised for comparison.</p><p><b><i>Results:</i></b> The HEHPLS and the HEHP diets for both the cook-chill and frozen Smart Pack menus provided mean sodium levels within the reference range. The LS diet code modifier reduced average sodium level in the menus by 925mg for cook-chill and 539mg for the Smart pack menus (Figure 1). However, the LS diet code modifier also decreased weekly main meal options by 33% and 50% for the two menus, respectively (Table 1). The HEHPLS smart-pack had the highest protein provision (105g) and met reference requirements. There was a varied provision from the other diet codes, ranging from average 86-98g protein and 8.6-10.3 MJ, under the requirements of the reference patient (Table 1) without ONS.</p><p><b>308</b></p><p><b>Effects of an anti inflammatory diet on hepatic fibrosis and inflammation in patients with metabolic dysfunction- associated steatotic liver disease</b></p><p><b>Wai See Ma</b></p><p><i>Blacktown Hospital, Blacktown, Australia</i></p><p><b><i>Background:</i></b> Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) is closely related with obesity, metabolic syndrome, and diabetes. Its prevalence is on the rise, affecting approximately 25% of the world’s population and 5.6M Australians adults (age ≥18). Limited therapeutic options exist for the condition, and the mainstay of treatment remains as lifestyle modification through diet and exercise. Whilst weight loss has a definite role to play in this condition, recent studies have suggested that inflammation also has a role in the pathogenesis of MASLD. An anti-inflammatory diet may be an additional therapeutic option, as the Mediterranean diet, a component in the anti-inflammatory diet, has been recommended as dietary intervention for MASLD.</p><p><b><i>Methods:</i></b> A literature search on MEDLINE, EMBASE, SCOPUS and Cochrane Library was conducted in March 2023, using search terms “anti-inflammatory diet”, “Mediterranean diet”, or “Okinawan diet”, and “metabolic associated fatty liver disease”. Original research and review articles were summarised.</p><p><b><i>Results:</i></b> Positive outcomes have been noted with the anti-inflammatory diet on MASLD, including anthroprometric measurements, Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), hepatic fibrosis, and inflammatory markers.</p><p><b><i>Conclusion:</i></b> Our review indicated that an anti-inflammatory diet, such as the Mediterranean diet, is a useful therapeutic option in the management of MASLD. Whilst only limited cohort studies are available, with this positive relationship, further research in this field is required to draw more solid conclusions on the feasibility and utility of the anti-inflammatory diet on MASLD. It would be interesting and important to devise a diet which is not solely focused on weight loss, but rather combats the inflammatory pathway in the pathogesis of MASLD.</p><p><b>311</b></p><p><b>Nutritional assessment of patients with liver cirrhosis in the outpatient setting: a narrative review</b></p><p><b>Tsz Hong Yiu</b><sup>2</sup>, <b>Stuart Bartlett</b><sup>1</sup> and Zina Valaydon<sup>2</sup></p><p><sup>1</sup><i>University Of Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>Western Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Malnutrition in patients with Liver Cirrhosis (LC) is common and associated with increased rates of liver-related complications and overall mortality. Currently, consensus guidelines for assessment of malnutrition in LC are lacking, and many clinicians are unaware of the available nutritional assessment tools. This leads to underdiagnosis of malnutrition and suboptimal management of these patients. This narrative review evaluates existing nutritional assessment tools, with the aim of providing recommendations on suitable tools for implantation in the outpatient setting.</p><p><b><i>Methods:</i></b> We reviewed 60 articles sourced from Ovid Medline, PubMed, Web of Science and CINAHL databases that met our inclusion criteria. These articles evaluated nutritional assessment tools in patients with LC attributed to alcohol-related liver disease, viral hepatitis and metabolic fatty liver disease.</p><p><b><i>Results:</i></b> Our findings favor Royal Free Hospital-Nutritional Prioritising Tool as a screening tool for its ease of administration showing high sensitivity, specificity and prognostic value. Liver-Disease Undernutrition Screening Tool offers self-administration benefits and high sensitivity but may be inaccurate with variable specificity. Mini Nutritional Assessment-Short Form showed high-sensitivity and specificity but has limited studies investigating it. When malnutrition is suspected, anthropometric tools and body composition analysis can be employed. Easily conducted anthropometric tools of Triceps Skinfold Thickness assessing fat mass and Mid-Arm Muscle Circumference assessing muscle mass are recommended and utilising both of these account for the differing malnutrition pattern in males and females. While Body Mass Index shows low sensitivity, potentially due to fluid retention in LC. For Body composition analysis, bioelectrical Impedance analysis is cost-effective and shows reasonable sensitivity, specificity and reproducibility and thus is recommended. Similarly, Dual X-ray Absorptiometry is recommended due to consistent validity and relatively low cost with minimal radiation exposure while Computer Tomography is not recommended with low sensitivity and greater radiation exposure. Biochemical parameters albumin, Skin-Prick Hypersensitivity and Leucocyte count are not recommended due to correlation with severity of liver disease rather than malnutrition. While leptin shows promise, further investigation establishing specific cut-off values is required. Functional assessment using Hand grip strength is a simple measure for assessing sarcopenia, although its variable specificity requires further validation.</p><p><i><b>Conclusion</b>:</i> Recommended tools are Royal Free Hospital-Nutritional Prioritising Tool, Triceps Skinfold Thickness in females and Mid-Arm Muscle Circumference in males, Bioelectrical impedance Analysis and Dual-energy X-ray Absorptiometry. Further research should focus on developing tailored nutritional assessment tools accounting for the characteristics and unique challenges of liver cirrhosis to enhance diagnosis, management and outcomes.</p><p><b>312</b></p><p><b>Healthier dietary intake is positively associated with disease activity and inflammation in Australian adults with inflammatory bowel disease</b></p><p><b>Denelle Cosier</b><sup>1</sup>, Karen Charlton<sup>1</sup>, Kelly Lambert<sup>1</sup>, Julianna Lys de Sousa Alves Neri<sup>1</sup>, Marijka Batterham<sup>2</sup>, Sabrina Koentgen<sup>3</sup>, Nan Wu<sup>3</sup>, Paris Tavakoli<sup>3</sup>, Andrew Chung<sup>3</sup>, Anson Ho<sup>3</sup>, Simon Ghaly<sup>4</sup>, Susan J Connor<sup>5</sup>, Rupert Leong<sup>6</sup>, Nick J Talley<sup>7</sup>, Steven Leach<sup>8</sup>, Daniel Lemberg<sup>9</sup>, Shoma Dutt<sup>10</sup> and Georgina Hold<sup>3</sup></p><p><sup>1</sup><i>School of Medical, Indigenous and Health Sciences, University of Wollongong, Wollongong, Country;</i> <sup>2</sup><i>Statistical Consulting Centre, National Institute for Applied Statistical Research Australia, Wollongong, Australia;</i> <sup>3</sup><i>Microbiome Research Centre, Faculty of Medicine and Health, University of New South Wales, Sydney, Australia;</i> <sup>4</sup><i>Department of Gastroenterology and Hepatology, St Vincent’s Hospital Sydney and St Vincent’s Clinical School, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;</i> <sup>5</sup><i>Department of Gastroenterology, Liverpool Hospital and South West Sydney Clinical Campuses, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;</i> <sup>6</sup><i>Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;</i> <sup>7</sup><i>School of Medicine and Public Health, University of Newcastle, Newcastle, Australia;</i> <sup>8</sup><i>Discipline of Paediatrics, School of Clinical Medicine UNSW, Sydney, Australia;</i> <sup>9</sup><i>Department of Gastroenterology, Sydney Children's Hospital, Sydney, Australia;</i> <sup>10</sup><i>Department of Gastroenterology, The Sydney Children’s Hospital Network Randwick and Westmead, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Diet has been considered as one driving factor in the onset of Inflammatory Bowel Disease (IBD), however the mechanisms of interplay between diet, inflammation and disease activity are unclear. Given people living with IBD perceive diet to be an important modifiable factor in their disease management, ongoing research is needed to provide specific dietary recommendations. We explored the relationship between dietary intake, disease activity and intestinal inflammation in an Australian adult cohort with and without IBD.</p><p><b><i>Methods:</i></b> We analysed baseline dietary and clinical data from the Australian IBD Microbiome (AIM) study. AIM is a prospective longitudinal cohort study of adults and children with Crohn’s Disease (CD), Ulcerative colitis (UC) as well as healthy controls. Habitual dietary patterns were explored using Principal Component Analysis (PCA) from Food Frequency Questionnaire data (80-item validated tool; Cancer Council Victoria). The Dietary Inflammatory Index (DII) was computed from 3-day food records. Associations between diet, clinical disease activity from CD Activity Index (CDAI) or Partial Mayo scores (categorised as remission or active), and faecal calprotectin (FCP) were explored in adult participants.</p><p><b><i>Results:</i></b> 412 adults (CD = 117, UC = 106, Healthy = 189) were included. FCP data was available for 211 participants (HC = 100, CD = 49, UC = 62). Median (IQR) FCP at baseline was 0 (0-0) μg/g for HC and 33 (0-147) μg/g for IBD (p<0.001), indicating no intestinal inflammation. Median (IQR) partial Mayo at baseline was 1 (0-1) and median CDAI at baseline was 92 (48 – 168), indicating clinical remission in UC and CD. A dietary pattern comprising of high plant diversity was positively associated with active CD (CDAI 159.3 [84.9-204.0], p 0.004), and a ‘Prudent’ dietary pattern (characterised by high intake of plant milk and nuts) was positively associated with high FCP levels in the combined IBD cohort (>150 μg/g, p=0.015). Mean DII score was pro-inflammatory (1.01 ± 1.65) across all cohorts, with no significant differences between healthy vs IBD, CD vs UC or active vs remission cohorts. In UC, a pro-inflammatory diet was associated with a reduced likelihood of having active disease (OR = 0.76, 95% CI [0.58-0.98]) and was associated with no intestinal inflammation (p=0.032).</p><p><i><b>Conclusion:</b></i> Unexpectedly, healthier dietary patterns were positively associated with disease activity and higher FCP in Australian adults with IBD. Similarly, a pro-inflammatory diet was associated with disease remission in the UC cohort. Reverse causality cannot be ruled out, therefore, dietary modifications to manage active disease may explain the inverse association between healthier dietary intake and disease activity. Further longitudinal and clinical studies are needed to expand upon the findings.</p><p><b>400</b></p><p><b>A dietitian-led IBD clinic model is effective and efficient, with high patient satisfaction</b></p><p><b>Sarah Melton</b>, Miles Sparrow, Kate Norton, Alex Boussioutas and Jessica Fitzpatrick</p><p><i>Alfred Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Dietary management plays a critical role in the management of IBD, including using diet to treat active disease, management of non-inflammatory symptoms, prevention and management of complications, identification and treatment of malnutrition and perioperative nutritional optimisation; yet many patients lack access to specialised dietetic care. This audit describes the evaluation and impact of a pilot dietitian-led IBD clinic model in a tertiary IBD centre.</p><p><b><i>Methods:</i></b> A dietitian-led IBD clinic (0.4 dietetic EFT) was established and piloted for 6 months as part of a Nursing and Allied Health Lead Service model of care initiative. The clinic was designed to facilitate more rapid access to dietetic care for patients requiring priority assessment, with intervention frequency in line with best practice. This allowed diversion of stable patients from the regular IBD clinic to reduce frequency of medical review. Audit data was collected at each appointment by the clinic dietitian. Malnutrition was diagnosed according to GLIM<sup>1</sup> criteria. Priority of referrals was determined by Dietitian Crohn’s Colitis Australian Network (DECCAN) triage tool and best practice. Redcap surveys were used to measure patient satisfaction with dietetic care. Patient information was obtained from medical records. Descriptive statistics were used to describe data.</p><p><b><i>Results:</i></b> Seventy patients were referred to the dietitian, of whom 66 attended an initial appointment. A total of 165 appointments (162 TeleHealth, 3 face-to-face) were conducted in 6 months. Referrals were received from the standard IBD clinic and ward dietitians (47%), gastroenterologists (31%), IBD nurses (14%) or other/unknown sources (7%). Reasons for referral are presented in Figure 1. Median time from referral to assessment was 1 day (range 0-36 days) for urgent priority (within 7 days) patients (n=19), 3.5 days (range 1-36 days) for high (within 14 days) priority patients (n=6), 21 days (1-100 days) for moderate (within 30 days) priority patients (n=33) and 25.5 days (range 7-84 days) for low (within 90 days) priority patients (n=6). Eight patients (11%) were escalated to the gastroenterologist (IBD Fellow) due to suspected worsening disease activity, or other clinical concerns. Five patients (7%) were diagnosed with malnutrition as per GLIM criteria however the majority of appointments were conducted via Telehealth and physical assessments were not possible, therefore this is likely an under reporting. Of the patients discharged from the dietitian-led IBD service at the time of the audit, 79% achieved the goal of nutrition intervention. Patient engagement was high, with 90% of scheduled appointments attended. Patient satisfaction (15% survey response rate) was overwhelmingly high with 100% of patients reporting that the dietitian informed them adequately about nutrition and IBD, allowed for regular consultation, gave them confidence in the dietitian and felt that they were always taken seriously.</p><p><i><b>Conclusion</b>:</i> The dietitian-led IBD clinic model demonstrated effective specialised nutritional care within a multidisciplinary framework for IBD management. This approach led to dietetic assessment and intervention within desired and best practice timeframes (particularly for urgent and high priority patients), high patient engagement and satisfaction. Future studies should explore the impact of this model of care on clinical and nutritional outcomes, the scalability and long-term sustainability of this model, as well as financial analysis.</p><p><b>443</b></p><p><b>Dietary intake and nutrition interventions in pregnant women with inflammatory bowel disease: A systematic review</b></p><p><b>Emily Thompson</b><sup>1,2</sup>, Adrienne Forsyth<sup>2</sup> and Adam Walsh<sup>2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>Australian Catholic University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Dietary intake during pregnancy influences maternal health and the health of future generations, including the risk of developing chronic diseases later in life. The prevalence of inflammatory bowel disease (IBD), a condition affecting women of reproductive age, is increasing worldwide. IBD is associated with nutrient deficiencies and malnutrition due to reduced nutrition intake, restrictive diets, impaired nutrient absorption and chronic inflammation. This review aimed to identify studies reporting on dietary intake, quality and patterns of pregnant women with IBD and to evaluate the scope and implementation of nutrition interventions.</p><p><b><i>Methods:</i></b> Four electronic databases, Medline, CINAHL, Embase and Scopus, were systematically searched using the key terms “inflammatory bowel disease”, “pregnancy” and “dietary intake” in September 2023. Primary studies were included investigating food and nutrient intake, diet quality, dietary patterns, or the use of nutrition interventions in pregnant women aged 18 years or older with IBD. The risk of bias was assessed using the Joanna Briggs Institute checklists.</p><p><b><i>Results:</i></b> 12 studies were included. Three studies reported on dietary intake, quality or dietary patterns in pregnant women with Crohn’s disease (CD) and Ulcerative Colitis (UC). Pregnant women with IBD did not meet food and nutrient intake targets recommended by national dietary guidelines. They were more likely to follow a dietary pattern resembling a Western diet and had lower protein intakes from dairy sources compared to pregnant women without IBD. Nine studies, eight of which were case reports or case series, reported on the use of nutrition interventions in women with CD including parenteral nutrition (PN) (n=5), elemental diet (n=2), peptide-based formula therapy (n=1), and the Crohn’s Disease Exclusion Diet (n=1). These interventions were found to be safe and well-tolerated.</p><p><i><b>Conclusion</b>:</i> This review highlights a scarcity of data on the dietary intake of pregnant women with IBD. The evidence supporting the use of nutrition interventions, including therapeutic diets during pregnancy, is primarily derived from a limited number of case reports and case series, with even less data available for UC than CD. Larger scale, high-quality studies are needed to improve nutrition management and support for pregnant women with IBD, addressing their nutritional risks and challenges, and optimising maternal health and the intergenerational transfer of health.</p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":"39 S1","pages":"309-320"},"PeriodicalIF":3.4000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16706","citationCount":"0","resultStr":"{\"title\":\"Nutrition\",\"authors\":\"\",\"doi\":\"10.1111/jgh.16706\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>20</b></p><p><b>Risk factors for central line-associated bloodstream infections in home parenteral nutrition patients: an observational cohort study</b></p><p>Paris Hoey<sup>1</sup>, Douglas Roche<sup>1</sup>, Paul Chapman<sup>2</sup>, Vishal Kaushik<sup>1</sup>, Stacey Llewellyn<sup>3</sup> and Niwansa Adris<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Department of Infectious Disease, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>QIMR Berghofer Medical Research Institute, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> A central line-associated bloodstream infection (CLABSI) is a common and potentially life-threatening complication for patients with intestinal failure (IF) receiving home parenteral nutrition (HPN). In uncomplicated infections, The European Society for Clinical Nutrition and Metabolism guidelines advocate for central venous access (CVC) salvage for venous access preservation. Existing knowledge regarding the risk factors of HPN-related CLABSIs have been extrapolated from European and North American studies, and the effects of tropical climates and its potentially higher support requirements on the incidence of infection has not yet been studied. We sought to analyse the risk factors of developing HPN-related CLABSI, and assess CLABSI management, in a large Australian state with a highly dispersed population.</p><p><b><i>Methods:</i></b> A retrospective observational cohort study was conducted on 34 adult patients receiving HPN via a CVC at a Queensland tertiary referral centre, between 2016 and 2023. Patient charts were reviewed, and a univariate cox regression analysis model was used to identify predictors of CLABSI in the first CVC. Kaplan-Meier analysis was employed to build survival curves of time to CLABSI, and log-rank tests analysed survival between characteristics.</p><p><b><i>Results:</i></b> Nineteen patients had ≥1 CLABSI(s), accounting for a total of 39 episodes. Patients with ≥1 CLABSI(s) used regular opioids more than those who did not develop CLABSI (p=0.016). Fourteen patients (41%, n=14/34) developed a CLABSI in their first CVC. No patient or line characteristics, including tropical climate, were found to be predictive of CLABSI in their first CVC. The overall infection rate was 1.02 per 1000 catheter days. Most CLABSIs were caused by <i>Enterobacterales</i> (22%, n=12/55), followed by coagulase-negative <i>Staphylococcus</i> (18%, n=10/55). Administration of empiric antimicrobials within the standardised 3-hour sepsis timeframe was inadequate (50%, n=14/28), with only 25% (n=7/28) providing adequate cover of causative pathogens. The median time to effective antibiotic therapy was 22.7 hours (IQR 4.8-29.8). There were 3 CVC salvages (8%, n=3/39), all of which were successful.</p><p><i><b>Conclusion:</b></i> In this cohort of patients, regular opioid use was associated with an increased risk of developing CLABSI which is consistent with international studies. We also found a low CVC salvage rate in our cohort, representing potential missed opportunities for venous access preservation. Based on our findings, an empiric antimicrobial regime of vancomycin, cefepime and caspofungin for all HPN-related CLABSI cases would be expected to be effective for 84.6%. We recommend that Australian IF units with a similar antimicrobial distribution and resistance pattern adopt this regime.</p><p><b>28</b></p><p><b>Evaluating quality of life in patients who use home enteral nutrition in Australia/New Zealand</b></p><p><b>Mercedez Hinchcliff</b> and <b>Sarah Gray</b></p><p><i>University Of Wollongong, Wollongong, Australia</i></p><p><b><i>Background and Aim:</i></b> Home enteral nutrition (HEN) involves providing nutritional support to a person at home, orally or via a feeding tube into their stomach or intestines (1). While existing research primarily focuses on the clinical aspects of HEN (2, 3), there is a gap in the research from the patient perspective. The study aims to delve into various facets of HEN via tube feeding, with a particular emphasis on the financial and psychological burdens from a patient/carer perspective. We also aim to evaluate the societal stigma associated with tube feeding and its impact on patient experience.</p><p><b><i>Methods:</i></b> We adopted a mixed-method approach, disseminating an online anonymous questionnaire to patients and carers across Australia and New Zealand via collaborations with various support organizations. The questionnaire was formulated and adapted from NutriQol and HRQoL scales, supplemented with items to assess community and family support and open-ended questions to identify gaps in care.</p><p><b><i>Results:</i></b> The survey yielded 158 responses, comprising 91 from carers (both paediatric and adult) and 67 from adults who use HEN. Among the respondents, 47% reported receiving no government financial support (e.g., carer’s payment, health care cards), while 41% spent over $200 monthly on supplies. Most patients reported co-morbid conditions necessitating HEN, with the most prevalent diagnoses including dysphagia, failure to thrive (paediatric), gastroparesis, GERD/reflux, oral aversions, and eosinophilic oesophagitis (EoE). The beneficial implications of tube feeding are noteworthy, with 73% of adults reporting an enhanced sense of health and 80% feeling well-nourished. However, social concerns were evident, with numerous respondents limiting social engagements involving food. For paediatric respondents or their carers, the results were more positive, suggesting a higher level of acceptance of tube feeding among children and adolescents compared to adults. The majority did not attempt to hide their feeding tubes from friends nor feeling excluded. Only 22% of paediatric respondents experienced anxiety or depression, significantly lower than adults, potentially attributable to robust parental support. Despite these positive outcomes, both paediatric and adult respondents experienced physical discomfort (71%) and skin irritation (60%) from tube feeding.</p><p><b>79</b></p><p><b>Has ulcerative colitis been forgotten: what are the energy and protein requirements of adults with ulcerative colitis? A systematic scoping review</b></p><p><b>Samantha Plush</b><sup>1,2,3</sup>, Robert Bryant<sup>1,2,3</sup>, Rachel Davis<sup>1,2,3</sup>, Saravana Kumar<sup>4</sup> and Alice Day<sup>1,2,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>2</sup><i>The School of Medicine, University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>The Basil Hetzel Institute, Adelaide, Australia;</i> <sup>4</sup><i>Allied Health and Health Services, University of South Australia, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Ulcerative colitis (UC) affects only the colonic mucosa whereas Crohn’s disease (CD) is transmural and can involve any gastrointestinal segment. Nutritional requirements for these distinct diseases likely differ depending on location, inflammatory burden, and catabolism. Yet, energy and protein prescription recommendations for UC are largely extrapolated from CD studies. The aim of this scoping review was to evaluate the evidence for energy and protein prescription in adults with UC.</p><p><b><i>Methods:</i></b> Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews methodology was used. The search strategy identified key words including ulcerative colitis, inflammatory bowel disease, nutrition requirements, energy expenditure, indirect calorimetry, protein, and nitrogen balance. The search was conducted until April 2024 from EMBASE, EMCARE, MEDLINE and CINAHL databases. Full text citations were assessed against predefined inclusion and exclusion criteria by two reviewers. Data extraction was completed into predefined data extraction tables.</p><p><b><i>Results:</i></b> Of 9730 studies, 236 studies were eligible for full text screening. Thirteen studies evaluating 150 patients (92 male) were included. Measuring resting energy expenditure (mREE) via indirect calorimetry identified requirements increased in quiescent disease compared with active disease (Table 1). Doubly labelled water investigations found a difference between resting and total energy expenditure of 19.9 ± 7.27 kcal/kg/day in UC in clinical remission. Protein requirements of 1.24-1.4 g/kg/day in acute severe UC were needed to achieve nitrogen balance (Kjeldahl method) (Table 1). There were no data informing protein requirements in quiescent or mild to moderate UC.</p><p><b>98</b></p><p><b>Roux en Y jejunostomy in gastroparesis: insight into patient perspectives and outcomes</b></p><p><b>Omar Salehi</b><sup>1</sup>, Weilun Gao<sup>1</sup>, Christian Kenfield<sup>2</sup> and Geoffrey Hebbard<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Royal Melbourne Hospital, Parkville, Australia;</i> <sup>2</sup><i>Department of General Surgery, Melbourne Private Hospital, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastroparesis is a debilitating condition with patients sometimes requiring long-term enteral nutrition. Leakage, pain and social stigma may negatively impact quality of life in this patient cohort. This study aimed to explore patient experience post insertion of a jejunostomy with a Roux-en-Y anastomosis, a laparoscopic technique previously described in the pediatric population to reduce leakage and improve enteral feed tolerability, in 7 adult patients with idiopathic gastroparesis.</p><p><i><b>Methods:</b></i> Seven patients (6 female, 1 male) were interviewed about their experiences pre-and post-procedure up to 2 years. All had previously used other feeding tubes including nasogastric, nasojejunal and percutaneous endoscopic gastrostomy tubes. The patients were retrospectively surveyed for symptoms, nutrition, complications, day-to-day life, and satisfaction with the Roux en Y jejunostomy compared to previous feeding tubes.</p><p><b><i>Results:</i></b> Post-procedure, patients reported improvements in nausea (7/7; 100%), vomiting (6/7; 85.7%), and abdominal pain (6/7; 85.7%). Weight stabilized and oral intake improved in 57.1% (4/7) of patients. Most (6/7; 85.7%) described improved social confidence, increased energy, and better work/school functioning. One patient (1/7; 14.3%) experienced severe abdominal pain post-procedure, leading to jejunostomy removal. Minor leakage occurred in 42.9% (3/7) of cases. Despite challenges, most (6/7; 85.7%) patients preferred the Roux en Y jejunostomy over previous feeding tubes and stated they would undergo the procedure again.</p><p><b>140</b></p><p><b>Additive content of Australian oral nutrition supplements</b></p><p><b>Emily Monro</b><sup>1</sup>, <b>Erin Russell</b><sup>2,3</sup> and Jessica Fitzpatrick<sup>4</sup></p><p><sup>1</sup><i>NSW Health, Australia;</i> <sup>2</sup><i>St Vincent's Hospital Melbourne, Australia;</i> <sup>3</sup><i>University of Melbourne, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, School of Translational Medicine, Monash University</i></p><p><b><i>Background and Aim:</i></b> Pre-clinical and some observational studies have implicated ultra-processed foods (UPF), specific emulsifiers, thickeners, and artificial sweeteners in the pathogenesis of inflammatory bowel disease (IBD). Oral nutrition supplements (ONS) are UPFs, and commonly utilised in IBD for nutritional support, exclusive enteral nutrition (EEN) or the Crohn’s disease exclusion diet (CDED). With this paradox, we examine the reported deleterious food additive composition of ONS currently available in Australia.</p><p><b><i>Methods:</i></b> Current ingredient composition was sourced from all national suppliers (Nutricia, Fresenius Kabi, Nestle and Abbott). Standard adult and paediatric formulas were included and disease specific formulations were excluded. All additives were classed according to the Food Standards Australia New Zealand E numbers. Additives of interest were those reported to be deleterious to gut health including artificial sweeteners, maltodextrins, sulphites, titanium dioxide, and emulsifiers/thickeners (namely lecithin, gums, polysorbate 80, polyphosphates, carboxymethylcellulose, carrageenan, other mono and diglycerides of fatty acids) as these have been implicated in preclinical studies. Results are presented as mean ± standard deviation.</p><p><b><i>Results:</i></b> Forty-six oral supplements were reviewed. All products contained additives (any E number), with a minimum 5 and maximum 21 additives per supplement (Mean 12.8 ± 3.4). Of note, some of these appear to be for micronutrient provision. Specific to additives considered deleterious to gut health (listed above), the ONS had a mean 2.37 ± 1.39 additives per supplement (Figure 1). Maltodextrin was in 64% of products, with 40% (n=18) using maltodextrin as the primary carbohydrate source. Artificial sweeteners were in 6% (n=3), which were all milk-based products. Titanium dioxide, sulphites and polysorbate 80 were not found in any product. In terms of emulsifiers of interest, the supplements contained a mean 1.95 ± 1.0 per product. Specifically, 21% (n=10) contained carboxymethylcellulose, 15% (n=7) contained carrageenan and 72% (n=33) contained lecithin.</p><p><b>142</b></p><p><b>An exploration of nutrition and metabolic risk factors in non-alcoholic fatty liver disease and related cirrhosis</b></p><p><b>Catherine Stankevicius</b><sup>1,2,4</sup>, Rachel Davis<sup>2,4</sup>, Alison Yaxley<sup>1</sup>, Dep Huynh<sup>3</sup>, Martine Hatzi<sup>2</sup> and Alice Day<sup>2,4</sup></p><p><sup>1</sup><i>College of Nursing and Health Sciences, Flinders University, Bedford Park, Australia;</i> <sup>2</sup><i>Nutrition and Dietetics Department, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>3</sup><i>Gastroenterology and Hepatology Department, The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>4</sup><i>Basil Hetzel Institute for Translational Health Research, Woodville South, Australia</i></p><p><b><i>Background and Aim:</i></b> Incidence of non-alcoholic fatty liver disease (NAFLD) is rising. Risk factors for progression to cirrhosis include obesity (over nutrition), type 2 diabetes (T2DM), and westernised diets. Paradoxically, sarcopenia and malnutrition (under nutrition), accelerate disease progression. Clinical guidelines for liver disease recommend early allied health intervention to slow disease progression. This study aimed to determine modifiable nutrition and metabolic risk prevalence in a South Australian outpatient hepatology service without allied health integration for NAFLD and related cirrhosis.</p><p><b><i>Methods:</i></b> This cross-sectional study used convenience sampling between July and November 2023. Malnutrition universal screening tool score (MUST ≥2) defined risk while subjective global assessment (SGA, scores of B or C) diagnosed malnutrition. Sarcopenia risk was defined by the SARC-F questionnaire (score of ≥4). Anthropometrics included waist circumference and body mass index (BMI). Previous allied health interventions were assessed. Habitual diet was scored against a Mediterranean diet index (MED-Score).</p><p><b><i>Results:</i></b> Thirty-two participants consented to participate (median age 63 (Interquartile range (IQR) 55.5-70.8) years; 44% male). Table 1 summarises the cardiometabolic and nutrition risks. Prevalence of sarcopenia and malnutrition risk was low (median SARC-F scores=1 (IQR 0-2), and all had MUST >2. Three (9.4%) participants were malnourished (SGA B). Fifteen participants (46%) had been referred to a dietitian previously.</p><p><i><b>Conclusion:</b></i> Modifiable nutrition or metabolic risk factors in NAFLD and associated cirrhosis were prevalent, but can be optimised with diet and lifestyle intervention. Establishing tertiary referral pathways from Hepatology services to allied health is essential to manage modifiable risk factors to improve patient outcomes.</p><p><b>190</b></p><p><b>High Mediterranean diet adherence reduces risk of cancer and improves cancer survivorship</b></p><p><b>Daniel Clayton-chubb</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>1,2</sup>, Andrew T Chan<sup>3</sup>, Elena George<sup>4</sup>, Alex Boussioutas<sup>1,2</sup>, John McNeil<sup>2</sup>, Robyn Woods<sup>2</sup>, Alice Owen<sup>2</sup>, William Kemp<sup>1,2</sup>, Ammar Majeed<sup>1,2</sup> and Stuart Roberts<sup>1,2</sup></p><p><sup>1</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>2</sup><i>Monash University, Melbourne, Australia;</i> <sup>3</sup><i>Harvard Medical School, Boston, USA;</i> <sup>4</sup><i>Deakin University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> While a Mediterranean diet (MedDiet) is commonly recommended in primary and specialist care, yet its role in reducing the risk of cancer, gastrointestinal (GI) cancer and improving cancer survivorship is understudied especially in older adults. As such, we aimed to determine whether MedDiet adherence (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with incident cancer, incident GI cancer, and survivorship in older Australian adults.</p><p><b><i>Methods:</i></b> This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, which enrolled 12,581 participants. A MedDiet Score (MDS) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 18. Higher scores indicate greater adherence to a MedDiet style dietary pattern. Cancer incidence and sub-type were adjudicated by investigators based on medical records. Participants with cancer diagnosed during ASPREE prior to completion of the FFQ were excluded. GI cancer was defined as colorectal, gastric, gastro-oesophageal, liver, or pancreatic in origin. MDS was analysed in quartiles due to its non-linear association with incident GI cancer. Both unadjusted and adjusted cox regression were used in these analyses.</p><p><b><i>Results:</i></b> We included the 12,394 participants (median 76.8 [IQR 74.6 – 80.3] years) who answered a semi-quantitative FFQ while living at home/with family during ALSOP. Of these, 563 (4.5%) developed cancer during ASPREE but pre-questionnaire and were excluded and 10 had incomplete data. The remaining 11,831 were subsequently followed up for a median of 5.8 (IQR 4.6 – 6.5) years. Of these 11,4831, 1629 (13.8%) developed cancer, of which 344 (2.9% overall) were GI cancers. The mean (± SD) MDS was 11.1 (± 2.0). Univariate analysis showed higher adherence to a MedDiet was associated with a reduced hazard of all cancer (Q4 vs Q1 HR 0.71 [95% CI 0.62 – 0.81]) and GI cancer specifically (Q4 vs Q1 HR 0.70 [95% CI 0.51 – 0.95]) (Figure 1). Results remained significant for all cancer when adjusting for age, sex, BMI, alcohol and smoking status, ethnicity, diabetes, aspirin use, education, and participant history of cancer pre-dating ASPREE (all cancer Q1 vs Q4 aHR 0.85 [95% CI 0.74 – 0.99] but not GI cancer Q1 vs Q4 aHR 0.82 [95% CI 0.60 – 1.13]). In those who developed cancer, higher MDS was associated with reduced all-cause mortality (Q4 vs Q1 aHR 0.73 [95% CI 0.56 – 0.96]), though not in the GI cancer subgroup (Q4 vs Q1 aHR 0.87 [95% CI 0.53 – 1.43]).</p><p><b>191</b></p><p><b>Ultra-processed food is associated with death and dementia in older Australian adults</b></p><p><b>Daniel Clayton-chubb</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>1,2</sup>, Priscila Machado<sup>4</sup>, William Kemp<sup>1,2</sup>, Alice Owen<sup>2</sup>, John McNeil<sup>2</sup>, Robyn Woods<sup>1,2</sup>, Joanne Ryan<sup>1,2</sup>, Ammar Majeed<sup>1,2</sup>, Andrew T Chan<sup>3</sup> and Stuart Roberts<sup>1,2</sup></p><p><sup>1</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>2</sup><i>Monash University, Melbourne, Australia;</i> <sup>3</sup><i>Harvard Medical School, Boston, USA;</i> <sup>4</sup><i>Deakin University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> There is a growing body of evidence linking high Ultra-Processed Foods (UPFs) intake with deleterious health outcomes, including mortality and cognitive dysfunction. However, there are less data on the risks of high UPF intake in older adults. As such, we aimed to determine whether a high UPF diet (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with mortality or incident dementia in older Australian adults.</p><p><b><i>Methods:</i></b> This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, with 12,581 respondents. A UPF Diet Score (UPFQ) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 25. Higher scores indicate greater exposure to UPFs. Mortality and incident dementia were adjudicated by investigators based on medical records. Participants with dementia diagnosed during ASPREE prior to completion of the FFQ were excluded in dementia analyses, as were those with more than 20% missing UPF FFQ data. UPFQ was analysed in quartiles due to its non-linear association with all-cause mortality, and linearly for incident dementia. The nadir quartile was used as the reference for Cox models.</p><p><b><i>Results:</i></b> We included the 11,962 participants living home alone or with family (median [IQR] 76.8 [74.6 – 80.2] years) who adequately answered the FFQ during ALSOP. This group was followed up for a median of 5.9 (IQR 4.7 – 6.6) years. Of the included participants, 1,349 (11.3%) died. Sixty-six developed dementia pre-FFQ (0.6%) and were excluded from dementia analyses. The median (IQR) UPFQ was 6 (4.9 – 7.3). Univariate Cox Proportional Hazards Models showed higher UPF intake was associated with an increased hazard of all-cause mortality (Q4 vs Q2 HR 1.47 [95% CI 1.26 – 1.71]) and dementia (HR 1.09 [95% CI 1.04 – 1.14]). Results remained significant for mortality when adjusting for sex, BMI, age, smoking status, diabetes, renal function, cognitive function, depression, education, grip strength and gait speed (Q4 vs Q2 aHR 1.31 [95% CI 1.12 – 1.55]). Similarly, when fully adjusted, for every one-point increase in UPFQ there was an increased risk of dementia (aHR 1.08 [95% CI 1.03 – 1.14]). The increase in mortality impacted cardiovascular death (including stroke), cancer death, and other causes similarly (χ2 <i>p</i>-value = 0.687). Results remained significant when excluding those with less than 12 months of follow-up.</p><p><b>195</b></p><p><b>Quality over quantity: How can the quality of therapeutic diets be assessed for inflammatory bowel disease in Australia?</b></p><p><b>Laura Portmann</b><sup>1,2</sup>, Jessica Fitzpatrick<sup>3,4</sup>, Emma Halmos<sup>3,4</sup>, Robert Bryant<sup>1,2,5</sup> and Alice Day<sup>1,2,5</sup></p><p><sup>1</sup><i>The Queen Elizabeth Hospital, Woodville South, Australia;</i> <sup>2</sup><i>Basil Hetzel Institute, Woodville South, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia;</i> <sup>4</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>5</sup><i>The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Examining the quality of diets used to treat inflammatory bowel disease (IBD) is challenging as traditional dietary analysis methods are used to quantitatively assess food group and nutrient intakes, not overall diet quality. Yet, evidence is suggesting dietary patterns of differing quality such as ultra-processed foods or the Mediterranean diet (MED), rather than specific food components may be more predictive of disease onset and course. An IBD-specific diet quality index (DQI) does not exist. It is therefore unknown which DQI is most suitable to use in therapeutic IBD diet trials. This review aimed to identify current DQIs and assess their suitability for use on therapeutic diets in an Australian IBD population.</p><p><b><i>Methods:</i></b> Electronic databases, MEDLINE and EmCare, were systematically searched for a-priori, food-based DQI reflecting national dietary guidelines and/or latest nutrition science for adults published 2013 to 2023, in English language. Excluded were DQI that were posteriori or for specific, non-IBD diseases (e.g., diabetes). Data extracted were adapted from optimal DQI criteria described by Burggraf et al.,<sup>1</sup> which include quality measures of adequacy, moderation, variety and balance for food and nutrient components and DQI evaluation, as well as its use, if any, for IBD health outcomes.</p><p><b><i>Results:</i></b> Twenty-five articles describing 25 DQI were included in final analysis. Sixteen DQI were adapted from existing DQI. Dietary guidelines were used to develop 19/25 (76%) DQI, while the remaining six were developed from dietary patterns (e.g., MED, EAT-Lancet Diet). Whole food groups were assessed by all DQI, but assessment of individual foods within groups varied. Ultra-processed foods were assessed in 16/25 (64%) DQI. No DQI included all optimal DQI criteria<sup>1</sup>. The Dietary Guideline Index 2013 (DGI-2013) most closely met DQI criteria, followed by the Healthy Eating Index for Australian Adults-2013 (HEIFA-2013) (Table 1). Seven of 25 DQI were Australian population specific. All Australian DQI evaluated adequacy, however assessment of other quality dimensions and scoring methods varied as outlined in Table 1. All except one Australian DQI were applied to food frequency questionnaires (FFQ). Eleven of 25 (44%) DQI, yet only two Australian DQI were not weighted equally to account for different weighted contributions of foods and nutrients to established health and disease outcomes. Seventeen of 25 (68%) DQI were validated, however few were evaluated for reproducibility (2/25) or reliability (7/25). No DQI was validated to assess gut-specific health outcomes. Two DQI (Dietary Diversity Score and Australian Recommended Food Score (ARFS)) were used to assess against gut microbiota. The DGI-2013 and Dutch Healthy Diet index-2015 were applied to FFQ from various IBD participants.</p><p><b>Reference</b></p><p>\\n 1. <span>Burggraf, C.</span>, <span>Teuber, R.</span>, <span>Brosig, S.</span>, & <span>Meier, T.</span> (<span>2018</span>). <span>Review of a priori dietary quality indices in relation to their construction criteria</span>. <i>Nutrition reviews</i>, <span>76</span>(<span>10</span>), <span>747</span>-<span>764</span>.</p><p><b>206</b></p><p><b>Systematic scoping review: dietary interventions for the treatment of primary sclerosing cholangitis</b></p><p><b>Caitlin Theron</b><sup>1,2</sup>, Robert Bryant<sup>1,2</sup>, Damjana Bogatic<sup>1,2</sup> and Alice Day<sup>1,2</sup></p><p><sup>1</sup><i>The Queen Elizabeth Hospital Gastroenterology Department, Adelaide, Australia;</i> <sup>2</sup><i>Basil Hetzel Institute, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Primary sclerosing cholangitis (PSC), is a rare autoimmune liver disease with no effective medical therapies. The etiopathogenesis of PSC is incompletely understood, however evolving evidence suggests dysbiosis of the gut microbiota may play a key role. Diet is an important fertiliser of gut microbiota and has potential to be a modifiable risk factor in PSC. This review aims to scope available evidence of dietary factors that may influence PSC disease course.</p><p><b><i>Methods:</i></b> A systematic scoping search of electronic databases EMBASE, EMCARE, MEDLINE and CINAL was carried out. Key search terms included primary sclerosing cholangitis, diet, nutrition, therapy, and gut microbial diversity. Included articles were original, peer-reviewed research and case reports, both human and pre-clinical models, that produced evidence of a diet or nutrient that contributed any effect to disease stabilisation, progression, symptoms, gut microbes, or survival rate associated with PSC.</p><p><b><i>Results:</i></b> Of 1466 articles screened, 15 were included for review including four pre-clinical PSC models and 13 in humans. Outcome measures varied across studies, however most (8/15, 53%) assessed a change in biochemical parameters associated with poor patient outcomes, as outlined in Table 1. In human studies, the addition of retinoic acid for patient’s taking ursodeoxycholic acid (UDCA) was the only intervention found to significantly change one of the liver function tests, causing a reduction in alanine transferase (ALT). In mouse models of PSC, geniposide and berberine significantly reduced alkaline phosphatase (ALP), aspartate aminotransferase (AST) and ALT. No other interventions were found to significantly alter biochemical parameters. Survival rates were increased by coffee in patients with PSC (p=0.02), and by vitamin D in a PSC mouse model (p=0.01). Regarding symptoms, pruritis and abdominal pain were improved by N-acetylcysteine (p value not reported), while dietary fiber had no significant effect on pruritus (p value not reported). Only one article examined the effect of the intervention on the gut microbiome, finding that berberine reduced gut permeability (p<0.001), increased <i>Bacteroidetes</i> and decreased <i>Firmicutes</i> (p values not reported).</p><p><b><i>Conclusion:</i></b> There are limited well designed clinical trials and data evaluating diet in PSC disease course. Of existing evidence, few dietary interventions significantly altered biochemical parameters associated with disease progression, including retinoic acid, geniposide and berberine. Only one article provided data on the relationship between the dietary factor, the gut microbiome and PSC disease course. Further research should include well-designed clinical trials that investigate the role of dietary factors in disease progression and the role of diet as a microbial restoration therapy.</p><p>\\n \\n </p><p><b>223</b></p><p><b>Practical application of evidence-based dietary therapy into inflammatory bowel disease care shows high patient satisfaction and compliance, and improved disease activity: The DELECTABLE program</b></p><p><b>Gina Trakman</b><sup>1,2,3</sup>, Erin Russell<sup>1,2</sup>, Amy Hamilton<sup>1,2</sup>, Amy Wilson-o'brien<sup>1,2</sup>, Emily Thompson<sup>1</sup>, Natalie Simmance<sup>1</sup>, Ola Niewiadomski<sup>1</sup> and Michael Kamm<sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>La Trobe University, Melbourne, Australia</i></p><p><b><i>Background and aims:</i></b> A range of diets have been shown in controlled trials to be therapeutically effective in Inflammatory Bowel Diseases (IBD). Exclusive enteral nutrition (EEN) and the Crohn’s Disease Exclusion Diet (CDED) have confirmed efficacy in inducing remission in Crohn’s disease (CD). Low sulphur and plant-based diets are being investigated in ulcerative colitis (UC). Reducing ultra-processed, additive-containing food intake is emerging as important, given its role in initiating and perpetuating disease. IBD patients believe in the value of modifying diet to improve disease control. Yet there is no evidence for diet tolerability and benefit outside clinical trials. The DELECTABLE program, a dietitian-led telehealth service, aimed to evaluate the patient acceptability, compliance, and benefit of structured, evidence-based dietary therapy as part of routine clinical care.</p><p><i><b>Methods</b>:</i> In this open-label, prospective, interventional cohort program, patients with Crohn’s disease or an ileo-anal pouch were offered the CDED or a wholefood additive-free diet (WFD), patients with ulcerative colitis were offered a low-sulphur plant-based diet (UCD) or WFD, and patients with microscopic colitis were offered the WFD. The primary outcomes were diet satisfaction (modified DSAT-28: range 27 to 135), dietitian-rated compliance (range 1-6), and patient-rated compliance (range 1 -5). Secondary outcomes were the amount of food additive intake (validated food frequency questionnaire), quality of life (IBDQ9; range 7-49), disease activity score (CDAI in CD, partial Mayo score in UC), CRP, and faecal calprotectin. Baseline to Week 12 differences were assessed for the CDED and wholefood diet using the Paired T-test or Wilcoxon-sign-test. Inferential statistics were not conducted for disease activity on the UCD due to sample size.</p><p><b><i>Results:</i></b> Of 165 patients referred, 76 enrolled in the program. Sixty-four (82%) (mean age 36; 53% male) of enrolled patients completed 12 weeks of diet therapy, with 15, 42 and 7 participants completing the CDED, WFD, and UCD, respectively. Diet satisfaction was high at Week 1 on CDED (median 79 out of 135) and did not significantly change at Week 12 (median 83 out of 135, P=0.212). Diet satisfaction improved on the WFD from Week 1 to 12 (84.1 vs 86.9, P = 0.03) (Figure 1, Panel B). Median dietitian-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/6 v 4/6, P=0.682; WFD: 3/5 vs 3/5, P=0.165; UCD: 4/6 vs 4/6, P=0.233). Likewise, median patient-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/5 v 4/5, P=0.565; WFD: 4/5 vs 4/5, P=0.348; UCD: 4.5/5 vs 4/5, P=0.368) (Figure 1, Panel B). Quality of life increased from Week 1 to Week 12 on the CDED (35 vs 51, P<0.001) and the WFD (37.1 vs 48.3, P<0.001). With regard to food additive ingestion: on the WFD, there was a significant reduction in carboxymethylcellulose (P=0.02), carrageenan (P=0.013), sucralose (P=0.018) and sulphites (P=0.007) ingestion. On the UCD there was a significant reduction in daily intake of all food additives (aspartame P=0.043; others P <0.028). On the CDED, from baseline to Week 12, there was a reduction in CRP (7.5 vs 4.6, P=0.034), calprotectin (195 vs 62, P=0.045) and CDAI (153 vs 43, P=0.023). On the WFD from baseline to Week 12, there was a significant reduction in CDAI (50 vs 32, P= 0.027) and partial Mayo score (2 vs 0, P=0.004). On the UCD, there was no change from baseline to Week 12 CRP (0 vs 1), partial Mayo score (3 vs 3) or calprotectin (112 vs 174).</p><p><b><i>Conclusion:</i></b> Implementation of well-balanced, effective diet therapies is feasible and well-accepted by patients with IBD, with a promising impact on disease activity.</p><p><b>255</b></p><p><b>Peripheral parenteral nutrition: an evaluation of utility and complications</b></p><p><b>Emma Bidgood</b><sup>1</sup>, Joanna Huang<sup>2</sup>, Elise Murphy<sup>3</sup>, Ralley Prentice<sup>4</sup>, Beth Hede<sup>2</sup> and David Russell<sup>2,5</sup></p><p><sup>1</sup><i>Department of Allied Health (Clinical Nutrition), The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>2</sup><i>Department of Gastroenterology, The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>3</sup><i>Pharmacy Department, The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Monash Medical Centre, Clayton, Australia;</i> <sup>5</sup><i>Department of Medicine, Melbourne Medical School, The University of Melbourne, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Peripheral parenteral nutrition (PPN) provides an alternative nutrition support strategy to centrally administered parenteral nutrition (PN) for specific patients requiring short-term PN. Previous studies have demonstrated limited utilization of PPN and variations in complication rates. This study aimed to evaluate PPN complications and usage at this center.</p><p><b><i>Methods:</i></b> This was a single-center retrospective observational study of all adult patients who received at least 1 day of PPN from June 2018 to December 2023. Demographic and clinical data were collected including, complications, indications for PN and reason for PPN, duration of therapy, reason for cessation of PPN, nutritional status, energy and protein provision and central line insertion rates.</p><p><b><i>Results:</i></b> A total of 381 patients were included, median age 62 [IQR 28-74] years, 235 males (61.7%). The most common indication for PN was ileus (n=153, 40%), followed by gastrointestinal obstruction (n=93, 24%). The median time on PPN was 3 [2-4] days. Patients received a median of 65% [55-75] of energy and 58% [50-69] of protein requirements with PPN. Malnutrition was diagnosed in 47.5% (n=181) of this cohort. Total complication rates were 8.7% (n=33) with cannula infiltration being the most common complication (6.6%, n=25). 213 (56%) patients proceeded to central line insertion.</p><p><b><i>Conclusion</i></b>: PPN proved to be a safe and effective therapy for short-term PN when managed by a nutrition support team. PPN has the potential to attenuate short-term nutritional deficits and prevent CVAD insertion in selected patients, making it a valuable therapy in type 1 intestinal failure.</p><p><b>260</b></p><p><b>Low salt diet modifiers may not be necessary for all inpatients with liver cirrhosis</b></p><p><b>Annie Shanahan</b><sup>1</sup>, Stacey Sayers<sup>1</sup>, Nicole Barna<sup>1</sup>, Alison Stewart<sup>1</sup>, Kelly Ho<sup>2</sup>, Georgina Petrusma<sup>2</sup>, Veronika Pudikova<sup>2</sup>, Angela Taylor<sup>2</sup>, Qinfang Yang<sup>2</sup>, Han Yu<sup>2</sup> and Erin Russell<sup>1</sup></p><p><sup>1</sup><i>Department of Nutrition and Dietetics, Monash Health, Australia;</i> <sup>2</sup><i>Department of Nutrition, Dietetics and Food, Monash University, Australia</i></p><p><b><i>Background:</i></b> An order for a high energy, high protein, low salt (HEHPLS) diet is common practice to support inpatients with liver cirrhosis. However, evidence suggests that a low salt (LS) diet can reduce palatability and hinder energy and protein intake in this patient group with increased nutrient needs. International guidelines recommend a ‘moderate’ daily salt restriction (1840-2760mg) for these patients. Clinicians were concerned that the LS diet modifier was unnecessarily limiting meal options. Automated oral nutrition supplements (ONS) are being considered. Therefore, a review of the energy, protein and sodium content of diet codes HEHPLS and high energy, high protein (HEHP) was conducted and compared with established clinical guideline reference ranges.</p><p><b><i>Methods:</i></b> In September 2023, six dietetics students undertook a detailed menu review. Both the 28-day cycle cook-chill and the 7-day frozen meal ‘Smart Pack’ menus at our hospital network were reviewed. To ensure all menu options were captured, the full menu cycle was analysed on the online menu system by selecting three main meals and two snacks per day. A variety of meals and snacks were selected to reflect a typical choice of a patient across the days of the menus. Energy, protein and sodium content was then averaged. Results therefore reflect nutrition provision to patients, rather than actual patient consumption. Requirements of a ‘reference patient’ with BMI 25 and decompensated liver cirrhosis was utilised for comparison.</p><p><b><i>Results:</i></b> The HEHPLS and the HEHP diets for both the cook-chill and frozen Smart Pack menus provided mean sodium levels within the reference range. The LS diet code modifier reduced average sodium level in the menus by 925mg for cook-chill and 539mg for the Smart pack menus (Figure 1). However, the LS diet code modifier also decreased weekly main meal options by 33% and 50% for the two menus, respectively (Table 1). The HEHPLS smart-pack had the highest protein provision (105g) and met reference requirements. There was a varied provision from the other diet codes, ranging from average 86-98g protein and 8.6-10.3 MJ, under the requirements of the reference patient (Table 1) without ONS.</p><p><b>308</b></p><p><b>Effects of an anti inflammatory diet on hepatic fibrosis and inflammation in patients with metabolic dysfunction- associated steatotic liver disease</b></p><p><b>Wai See Ma</b></p><p><i>Blacktown Hospital, Blacktown, Australia</i></p><p><b><i>Background:</i></b> Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) is closely related with obesity, metabolic syndrome, and diabetes. Its prevalence is on the rise, affecting approximately 25% of the world’s population and 5.6M Australians adults (age ≥18). Limited therapeutic options exist for the condition, and the mainstay of treatment remains as lifestyle modification through diet and exercise. Whilst weight loss has a definite role to play in this condition, recent studies have suggested that inflammation also has a role in the pathogenesis of MASLD. An anti-inflammatory diet may be an additional therapeutic option, as the Mediterranean diet, a component in the anti-inflammatory diet, has been recommended as dietary intervention for MASLD.</p><p><b><i>Methods:</i></b> A literature search on MEDLINE, EMBASE, SCOPUS and Cochrane Library was conducted in March 2023, using search terms “anti-inflammatory diet”, “Mediterranean diet”, or “Okinawan diet”, and “metabolic associated fatty liver disease”. Original research and review articles were summarised.</p><p><b><i>Results:</i></b> Positive outcomes have been noted with the anti-inflammatory diet on MASLD, including anthroprometric measurements, Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), hepatic fibrosis, and inflammatory markers.</p><p><b><i>Conclusion:</i></b> Our review indicated that an anti-inflammatory diet, such as the Mediterranean diet, is a useful therapeutic option in the management of MASLD. Whilst only limited cohort studies are available, with this positive relationship, further research in this field is required to draw more solid conclusions on the feasibility and utility of the anti-inflammatory diet on MASLD. It would be interesting and important to devise a diet which is not solely focused on weight loss, but rather combats the inflammatory pathway in the pathogesis of MASLD.</p><p><b>311</b></p><p><b>Nutritional assessment of patients with liver cirrhosis in the outpatient setting: a narrative review</b></p><p><b>Tsz Hong Yiu</b><sup>2</sup>, <b>Stuart Bartlett</b><sup>1</sup> and Zina Valaydon<sup>2</sup></p><p><sup>1</sup><i>University Of Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>Western Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Malnutrition in patients with Liver Cirrhosis (LC) is common and associated with increased rates of liver-related complications and overall mortality. Currently, consensus guidelines for assessment of malnutrition in LC are lacking, and many clinicians are unaware of the available nutritional assessment tools. This leads to underdiagnosis of malnutrition and suboptimal management of these patients. This narrative review evaluates existing nutritional assessment tools, with the aim of providing recommendations on suitable tools for implantation in the outpatient setting.</p><p><b><i>Methods:</i></b> We reviewed 60 articles sourced from Ovid Medline, PubMed, Web of Science and CINAHL databases that met our inclusion criteria. These articles evaluated nutritional assessment tools in patients with LC attributed to alcohol-related liver disease, viral hepatitis and metabolic fatty liver disease.</p><p><b><i>Results:</i></b> Our findings favor Royal Free Hospital-Nutritional Prioritising Tool as a screening tool for its ease of administration showing high sensitivity, specificity and prognostic value. Liver-Disease Undernutrition Screening Tool offers self-administration benefits and high sensitivity but may be inaccurate with variable specificity. Mini Nutritional Assessment-Short Form showed high-sensitivity and specificity but has limited studies investigating it. When malnutrition is suspected, anthropometric tools and body composition analysis can be employed. Easily conducted anthropometric tools of Triceps Skinfold Thickness assessing fat mass and Mid-Arm Muscle Circumference assessing muscle mass are recommended and utilising both of these account for the differing malnutrition pattern in males and females. While Body Mass Index shows low sensitivity, potentially due to fluid retention in LC. For Body composition analysis, bioelectrical Impedance analysis is cost-effective and shows reasonable sensitivity, specificity and reproducibility and thus is recommended. Similarly, Dual X-ray Absorptiometry is recommended due to consistent validity and relatively low cost with minimal radiation exposure while Computer Tomography is not recommended with low sensitivity and greater radiation exposure. Biochemical parameters albumin, Skin-Prick Hypersensitivity and Leucocyte count are not recommended due to correlation with severity of liver disease rather than malnutrition. While leptin shows promise, further investigation establishing specific cut-off values is required. Functional assessment using Hand grip strength is a simple measure for assessing sarcopenia, although its variable specificity requires further validation.</p><p><i><b>Conclusion</b>:</i> Recommended tools are Royal Free Hospital-Nutritional Prioritising Tool, Triceps Skinfold Thickness in females and Mid-Arm Muscle Circumference in males, Bioelectrical impedance Analysis and Dual-energy X-ray Absorptiometry. Further research should focus on developing tailored nutritional assessment tools accounting for the characteristics and unique challenges of liver cirrhosis to enhance diagnosis, management and outcomes.</p><p><b>312</b></p><p><b>Healthier dietary intake is positively associated with disease activity and inflammation in Australian adults with inflammatory bowel disease</b></p><p><b>Denelle Cosier</b><sup>1</sup>, Karen Charlton<sup>1</sup>, Kelly Lambert<sup>1</sup>, Julianna Lys de Sousa Alves Neri<sup>1</sup>, Marijka Batterham<sup>2</sup>, Sabrina Koentgen<sup>3</sup>, Nan Wu<sup>3</sup>, Paris Tavakoli<sup>3</sup>, Andrew Chung<sup>3</sup>, Anson Ho<sup>3</sup>, Simon Ghaly<sup>4</sup>, Susan J Connor<sup>5</sup>, Rupert Leong<sup>6</sup>, Nick J Talley<sup>7</sup>, Steven Leach<sup>8</sup>, Daniel Lemberg<sup>9</sup>, Shoma Dutt<sup>10</sup> and Georgina Hold<sup>3</sup></p><p><sup>1</sup><i>School of Medical, Indigenous and Health Sciences, University of Wollongong, Wollongong, Country;</i> <sup>2</sup><i>Statistical Consulting Centre, National Institute for Applied Statistical Research Australia, Wollongong, Australia;</i> <sup>3</sup><i>Microbiome Research Centre, Faculty of Medicine and Health, University of New South Wales, Sydney, Australia;</i> <sup>4</sup><i>Department of Gastroenterology and Hepatology, St Vincent’s Hospital Sydney and St Vincent’s Clinical School, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;</i> <sup>5</sup><i>Department of Gastroenterology, Liverpool Hospital and South West Sydney Clinical Campuses, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;</i> <sup>6</sup><i>Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;</i> <sup>7</sup><i>School of Medicine and Public Health, University of Newcastle, Newcastle, Australia;</i> <sup>8</sup><i>Discipline of Paediatrics, School of Clinical Medicine UNSW, Sydney, Australia;</i> <sup>9</sup><i>Department of Gastroenterology, Sydney Children's Hospital, Sydney, Australia;</i> <sup>10</sup><i>Department of Gastroenterology, The Sydney Children’s Hospital Network Randwick and Westmead, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Diet has been considered as one driving factor in the onset of Inflammatory Bowel Disease (IBD), however the mechanisms of interplay between diet, inflammation and disease activity are unclear. Given people living with IBD perceive diet to be an important modifiable factor in their disease management, ongoing research is needed to provide specific dietary recommendations. We explored the relationship between dietary intake, disease activity and intestinal inflammation in an Australian adult cohort with and without IBD.</p><p><b><i>Methods:</i></b> We analysed baseline dietary and clinical data from the Australian IBD Microbiome (AIM) study. AIM is a prospective longitudinal cohort study of adults and children with Crohn’s Disease (CD), Ulcerative colitis (UC) as well as healthy controls. Habitual dietary patterns were explored using Principal Component Analysis (PCA) from Food Frequency Questionnaire data (80-item validated tool; Cancer Council Victoria). The Dietary Inflammatory Index (DII) was computed from 3-day food records. Associations between diet, clinical disease activity from CD Activity Index (CDAI) or Partial Mayo scores (categorised as remission or active), and faecal calprotectin (FCP) were explored in adult participants.</p><p><b><i>Results:</i></b> 412 adults (CD = 117, UC = 106, Healthy = 189) were included. FCP data was available for 211 participants (HC = 100, CD = 49, UC = 62). Median (IQR) FCP at baseline was 0 (0-0) μg/g for HC and 33 (0-147) μg/g for IBD (p<0.001), indicating no intestinal inflammation. Median (IQR) partial Mayo at baseline was 1 (0-1) and median CDAI at baseline was 92 (48 – 168), indicating clinical remission in UC and CD. A dietary pattern comprising of high plant diversity was positively associated with active CD (CDAI 159.3 [84.9-204.0], p 0.004), and a ‘Prudent’ dietary pattern (characterised by high intake of plant milk and nuts) was positively associated with high FCP levels in the combined IBD cohort (>150 μg/g, p=0.015). Mean DII score was pro-inflammatory (1.01 ± 1.65) across all cohorts, with no significant differences between healthy vs IBD, CD vs UC or active vs remission cohorts. In UC, a pro-inflammatory diet was associated with a reduced likelihood of having active disease (OR = 0.76, 95% CI [0.58-0.98]) and was associated with no intestinal inflammation (p=0.032).</p><p><i><b>Conclusion:</b></i> Unexpectedly, healthier dietary patterns were positively associated with disease activity and higher FCP in Australian adults with IBD. Similarly, a pro-inflammatory diet was associated with disease remission in the UC cohort. Reverse causality cannot be ruled out, therefore, dietary modifications to manage active disease may explain the inverse association between healthier dietary intake and disease activity. Further longitudinal and clinical studies are needed to expand upon the findings.</p><p><b>400</b></p><p><b>A dietitian-led IBD clinic model is effective and efficient, with high patient satisfaction</b></p><p><b>Sarah Melton</b>, Miles Sparrow, Kate Norton, Alex Boussioutas and Jessica Fitzpatrick</p><p><i>Alfred Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Dietary management plays a critical role in the management of IBD, including using diet to treat active disease, management of non-inflammatory symptoms, prevention and management of complications, identification and treatment of malnutrition and perioperative nutritional optimisation; yet many patients lack access to specialised dietetic care. This audit describes the evaluation and impact of a pilot dietitian-led IBD clinic model in a tertiary IBD centre.</p><p><b><i>Methods:</i></b> A dietitian-led IBD clinic (0.4 dietetic EFT) was established and piloted for 6 months as part of a Nursing and Allied Health Lead Service model of care initiative. The clinic was designed to facilitate more rapid access to dietetic care for patients requiring priority assessment, with intervention frequency in line with best practice. This allowed diversion of stable patients from the regular IBD clinic to reduce frequency of medical review. Audit data was collected at each appointment by the clinic dietitian. Malnutrition was diagnosed according to GLIM<sup>1</sup> criteria. Priority of referrals was determined by Dietitian Crohn’s Colitis Australian Network (DECCAN) triage tool and best practice. Redcap surveys were used to measure patient satisfaction with dietetic care. Patient information was obtained from medical records. Descriptive statistics were used to describe data.</p><p><b><i>Results:</i></b> Seventy patients were referred to the dietitian, of whom 66 attended an initial appointment. A total of 165 appointments (162 TeleHealth, 3 face-to-face) were conducted in 6 months. Referrals were received from the standard IBD clinic and ward dietitians (47%), gastroenterologists (31%), IBD nurses (14%) or other/unknown sources (7%). Reasons for referral are presented in Figure 1. Median time from referral to assessment was 1 day (range 0-36 days) for urgent priority (within 7 days) patients (n=19), 3.5 days (range 1-36 days) for high (within 14 days) priority patients (n=6), 21 days (1-100 days) for moderate (within 30 days) priority patients (n=33) and 25.5 days (range 7-84 days) for low (within 90 days) priority patients (n=6). Eight patients (11%) were escalated to the gastroenterologist (IBD Fellow) due to suspected worsening disease activity, or other clinical concerns. Five patients (7%) were diagnosed with malnutrition as per GLIM criteria however the majority of appointments were conducted via Telehealth and physical assessments were not possible, therefore this is likely an under reporting. Of the patients discharged from the dietitian-led IBD service at the time of the audit, 79% achieved the goal of nutrition intervention. Patient engagement was high, with 90% of scheduled appointments attended. Patient satisfaction (15% survey response rate) was overwhelmingly high with 100% of patients reporting that the dietitian informed them adequately about nutrition and IBD, allowed for regular consultation, gave them confidence in the dietitian and felt that they were always taken seriously.</p><p><i><b>Conclusion</b>:</i> The dietitian-led IBD clinic model demonstrated effective specialised nutritional care within a multidisciplinary framework for IBD management. This approach led to dietetic assessment and intervention within desired and best practice timeframes (particularly for urgent and high priority patients), high patient engagement and satisfaction. Future studies should explore the impact of this model of care on clinical and nutritional outcomes, the scalability and long-term sustainability of this model, as well as financial analysis.</p><p><b>443</b></p><p><b>Dietary intake and nutrition interventions in pregnant women with inflammatory bowel disease: A systematic review</b></p><p><b>Emily Thompson</b><sup>1,2</sup>, Adrienne Forsyth<sup>2</sup> and Adam Walsh<sup>2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>Australian Catholic University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Dietary intake during pregnancy influences maternal health and the health of future generations, including the risk of developing chronic diseases later in life. The prevalence of inflammatory bowel disease (IBD), a condition affecting women of reproductive age, is increasing worldwide. IBD is associated with nutrient deficiencies and malnutrition due to reduced nutrition intake, restrictive diets, impaired nutrient absorption and chronic inflammation. This review aimed to identify studies reporting on dietary intake, quality and patterns of pregnant women with IBD and to evaluate the scope and implementation of nutrition interventions.</p><p><b><i>Methods:</i></b> Four electronic databases, Medline, CINAHL, Embase and Scopus, were systematically searched using the key terms “inflammatory bowel disease”, “pregnancy” and “dietary intake” in September 2023. Primary studies were included investigating food and nutrient intake, diet quality, dietary patterns, or the use of nutrition interventions in pregnant women aged 18 years or older with IBD. The risk of bias was assessed using the Joanna Briggs Institute checklists.</p><p><b><i>Results:</i></b> 12 studies were included. Three studies reported on dietary intake, quality or dietary patterns in pregnant women with Crohn’s disease (CD) and Ulcerative Colitis (UC). Pregnant women with IBD did not meet food and nutrient intake targets recommended by national dietary guidelines. They were more likely to follow a dietary pattern resembling a Western diet and had lower protein intakes from dairy sources compared to pregnant women without IBD. Nine studies, eight of which were case reports or case series, reported on the use of nutrition interventions in women with CD including parenteral nutrition (PN) (n=5), elemental diet (n=2), peptide-based formula therapy (n=1), and the Crohn’s Disease Exclusion Diet (n=1). These interventions were found to be safe and well-tolerated.</p><p><i><b>Conclusion</b>:</i> This review highlights a scarcity of data on the dietary intake of pregnant women with IBD. The evidence supporting the use of nutrition interventions, including therapeutic diets during pregnancy, is primarily derived from a limited number of case reports and case series, with even less data available for UC than CD. Larger scale, high-quality studies are needed to improve nutrition management and support for pregnant women with IBD, addressing their nutritional risks and challenges, and optimising maternal health and the intergenerational transfer of health.</p>\",\"PeriodicalId\":15877,\"journal\":{\"name\":\"Journal of Gastroenterology and Hepatology\",\"volume\":\"39 S1\",\"pages\":\"309-320\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16706\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16706\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16706","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Risk factors for central line-associated bloodstream infections in home parenteral nutrition patients: an observational cohort study
Paris Hoey1, Douglas Roche1, Paul Chapman2, Vishal Kaushik1, Stacey Llewellyn3 and Niwansa Adris1
1Department of Gastroenterology and Hepatology, Royal Brisbane and Women's Hospital, Brisbane, Australia;2Department of Infectious Disease, Royal Brisbane and Women's Hospital, Brisbane, Australia;3QIMR Berghofer Medical Research Institute, Brisbane, Australia
Background and Aim: A central line-associated bloodstream infection (CLABSI) is a common and potentially life-threatening complication for patients with intestinal failure (IF) receiving home parenteral nutrition (HPN). In uncomplicated infections, The European Society for Clinical Nutrition and Metabolism guidelines advocate for central venous access (CVC) salvage for venous access preservation. Existing knowledge regarding the risk factors of HPN-related CLABSIs have been extrapolated from European and North American studies, and the effects of tropical climates and its potentially higher support requirements on the incidence of infection has not yet been studied. We sought to analyse the risk factors of developing HPN-related CLABSI, and assess CLABSI management, in a large Australian state with a highly dispersed population.
Methods: A retrospective observational cohort study was conducted on 34 adult patients receiving HPN via a CVC at a Queensland tertiary referral centre, between 2016 and 2023. Patient charts were reviewed, and a univariate cox regression analysis model was used to identify predictors of CLABSI in the first CVC. Kaplan-Meier analysis was employed to build survival curves of time to CLABSI, and log-rank tests analysed survival between characteristics.
Results: Nineteen patients had ≥1 CLABSI(s), accounting for a total of 39 episodes. Patients with ≥1 CLABSI(s) used regular opioids more than those who did not develop CLABSI (p=0.016). Fourteen patients (41%, n=14/34) developed a CLABSI in their first CVC. No patient or line characteristics, including tropical climate, were found to be predictive of CLABSI in their first CVC. The overall infection rate was 1.02 per 1000 catheter days. Most CLABSIs were caused by Enterobacterales (22%, n=12/55), followed by coagulase-negative Staphylococcus (18%, n=10/55). Administration of empiric antimicrobials within the standardised 3-hour sepsis timeframe was inadequate (50%, n=14/28), with only 25% (n=7/28) providing adequate cover of causative pathogens. The median time to effective antibiotic therapy was 22.7 hours (IQR 4.8-29.8). There were 3 CVC salvages (8%, n=3/39), all of which were successful.
Conclusion: In this cohort of patients, regular opioid use was associated with an increased risk of developing CLABSI which is consistent with international studies. We also found a low CVC salvage rate in our cohort, representing potential missed opportunities for venous access preservation. Based on our findings, an empiric antimicrobial regime of vancomycin, cefepime and caspofungin for all HPN-related CLABSI cases would be expected to be effective for 84.6%. We recommend that Australian IF units with a similar antimicrobial distribution and resistance pattern adopt this regime.
28
Evaluating quality of life in patients who use home enteral nutrition in Australia/New Zealand
Mercedez Hinchcliff and Sarah Gray
University Of Wollongong, Wollongong, Australia
Background and Aim: Home enteral nutrition (HEN) involves providing nutritional support to a person at home, orally or via a feeding tube into their stomach or intestines (1). While existing research primarily focuses on the clinical aspects of HEN (2, 3), there is a gap in the research from the patient perspective. The study aims to delve into various facets of HEN via tube feeding, with a particular emphasis on the financial and psychological burdens from a patient/carer perspective. We also aim to evaluate the societal stigma associated with tube feeding and its impact on patient experience.
Methods: We adopted a mixed-method approach, disseminating an online anonymous questionnaire to patients and carers across Australia and New Zealand via collaborations with various support organizations. The questionnaire was formulated and adapted from NutriQol and HRQoL scales, supplemented with items to assess community and family support and open-ended questions to identify gaps in care.
Results: The survey yielded 158 responses, comprising 91 from carers (both paediatric and adult) and 67 from adults who use HEN. Among the respondents, 47% reported receiving no government financial support (e.g., carer’s payment, health care cards), while 41% spent over $200 monthly on supplies. Most patients reported co-morbid conditions necessitating HEN, with the most prevalent diagnoses including dysphagia, failure to thrive (paediatric), gastroparesis, GERD/reflux, oral aversions, and eosinophilic oesophagitis (EoE). The beneficial implications of tube feeding are noteworthy, with 73% of adults reporting an enhanced sense of health and 80% feeling well-nourished. However, social concerns were evident, with numerous respondents limiting social engagements involving food. For paediatric respondents or their carers, the results were more positive, suggesting a higher level of acceptance of tube feeding among children and adolescents compared to adults. The majority did not attempt to hide their feeding tubes from friends nor feeling excluded. Only 22% of paediatric respondents experienced anxiety or depression, significantly lower than adults, potentially attributable to robust parental support. Despite these positive outcomes, both paediatric and adult respondents experienced physical discomfort (71%) and skin irritation (60%) from tube feeding.
79
Has ulcerative colitis been forgotten: what are the energy and protein requirements of adults with ulcerative colitis? A systematic scoping review
Samantha Plush1,2,3, Robert Bryant1,2,3, Rachel Davis1,2,3, Saravana Kumar4 and Alice Day1,2,3
1Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Woodville South, Australia;2The School of Medicine, University of Adelaide, Adelaide, Australia;3The Basil Hetzel Institute, Adelaide, Australia;4Allied Health and Health Services, University of South Australia, Adelaide, Australia
Background and Aim: Ulcerative colitis (UC) affects only the colonic mucosa whereas Crohn’s disease (CD) is transmural and can involve any gastrointestinal segment. Nutritional requirements for these distinct diseases likely differ depending on location, inflammatory burden, and catabolism. Yet, energy and protein prescription recommendations for UC are largely extrapolated from CD studies. The aim of this scoping review was to evaluate the evidence for energy and protein prescription in adults with UC.
Methods: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews methodology was used. The search strategy identified key words including ulcerative colitis, inflammatory bowel disease, nutrition requirements, energy expenditure, indirect calorimetry, protein, and nitrogen balance. The search was conducted until April 2024 from EMBASE, EMCARE, MEDLINE and CINAHL databases. Full text citations were assessed against predefined inclusion and exclusion criteria by two reviewers. Data extraction was completed into predefined data extraction tables.
Results: Of 9730 studies, 236 studies were eligible for full text screening. Thirteen studies evaluating 150 patients (92 male) were included. Measuring resting energy expenditure (mREE) via indirect calorimetry identified requirements increased in quiescent disease compared with active disease (Table 1). Doubly labelled water investigations found a difference between resting and total energy expenditure of 19.9 ± 7.27 kcal/kg/day in UC in clinical remission. Protein requirements of 1.24-1.4 g/kg/day in acute severe UC were needed to achieve nitrogen balance (Kjeldahl method) (Table 1). There were no data informing protein requirements in quiescent or mild to moderate UC.
98
Roux en Y jejunostomy in gastroparesis: insight into patient perspectives and outcomes
Omar Salehi1, Weilun Gao1, Christian Kenfield2 and Geoffrey Hebbard1,2
1Department of Gastroenterology and Hepatology, Royal Melbourne Hospital, Parkville, Australia;2Department of General Surgery, Melbourne Private Hospital, Parkville, Australia
Background and Aim: Gastroparesis is a debilitating condition with patients sometimes requiring long-term enteral nutrition. Leakage, pain and social stigma may negatively impact quality of life in this patient cohort. This study aimed to explore patient experience post insertion of a jejunostomy with a Roux-en-Y anastomosis, a laparoscopic technique previously described in the pediatric population to reduce leakage and improve enteral feed tolerability, in 7 adult patients with idiopathic gastroparesis.
Methods: Seven patients (6 female, 1 male) were interviewed about their experiences pre-and post-procedure up to 2 years. All had previously used other feeding tubes including nasogastric, nasojejunal and percutaneous endoscopic gastrostomy tubes. The patients were retrospectively surveyed for symptoms, nutrition, complications, day-to-day life, and satisfaction with the Roux en Y jejunostomy compared to previous feeding tubes.
Results: Post-procedure, patients reported improvements in nausea (7/7; 100%), vomiting (6/7; 85.7%), and abdominal pain (6/7; 85.7%). Weight stabilized and oral intake improved in 57.1% (4/7) of patients. Most (6/7; 85.7%) described improved social confidence, increased energy, and better work/school functioning. One patient (1/7; 14.3%) experienced severe abdominal pain post-procedure, leading to jejunostomy removal. Minor leakage occurred in 42.9% (3/7) of cases. Despite challenges, most (6/7; 85.7%) patients preferred the Roux en Y jejunostomy over previous feeding tubes and stated they would undergo the procedure again.
140
Additive content of Australian oral nutrition supplements
Emily Monro1, Erin Russell2,3 and Jessica Fitzpatrick4
1NSW Health, Australia;2St Vincent's Hospital Melbourne, Australia;3University of Melbourne, Australia;4Department of Gastroenterology, School of Translational Medicine, Monash University
Background and Aim: Pre-clinical and some observational studies have implicated ultra-processed foods (UPF), specific emulsifiers, thickeners, and artificial sweeteners in the pathogenesis of inflammatory bowel disease (IBD). Oral nutrition supplements (ONS) are UPFs, and commonly utilised in IBD for nutritional support, exclusive enteral nutrition (EEN) or the Crohn’s disease exclusion diet (CDED). With this paradox, we examine the reported deleterious food additive composition of ONS currently available in Australia.
Methods: Current ingredient composition was sourced from all national suppliers (Nutricia, Fresenius Kabi, Nestle and Abbott). Standard adult and paediatric formulas were included and disease specific formulations were excluded. All additives were classed according to the Food Standards Australia New Zealand E numbers. Additives of interest were those reported to be deleterious to gut health including artificial sweeteners, maltodextrins, sulphites, titanium dioxide, and emulsifiers/thickeners (namely lecithin, gums, polysorbate 80, polyphosphates, carboxymethylcellulose, carrageenan, other mono and diglycerides of fatty acids) as these have been implicated in preclinical studies. Results are presented as mean ± standard deviation.
Results: Forty-six oral supplements were reviewed. All products contained additives (any E number), with a minimum 5 and maximum 21 additives per supplement (Mean 12.8 ± 3.4). Of note, some of these appear to be for micronutrient provision. Specific to additives considered deleterious to gut health (listed above), the ONS had a mean 2.37 ± 1.39 additives per supplement (Figure 1). Maltodextrin was in 64% of products, with 40% (n=18) using maltodextrin as the primary carbohydrate source. Artificial sweeteners were in 6% (n=3), which were all milk-based products. Titanium dioxide, sulphites and polysorbate 80 were not found in any product. In terms of emulsifiers of interest, the supplements contained a mean 1.95 ± 1.0 per product. Specifically, 21% (n=10) contained carboxymethylcellulose, 15% (n=7) contained carrageenan and 72% (n=33) contained lecithin.
142
An exploration of nutrition and metabolic risk factors in non-alcoholic fatty liver disease and related cirrhosis
Catherine Stankevicius1,2,4, Rachel Davis2,4, Alison Yaxley1, Dep Huynh3, Martine Hatzi2 and Alice Day2,4
1College of Nursing and Health Sciences, Flinders University, Bedford Park, Australia;2Nutrition and Dietetics Department, The Queen Elizabeth Hospital, Woodville South, Australia;3Gastroenterology and Hepatology Department, The Queen Elizabeth Hospital, Woodville South, Australia;4Basil Hetzel Institute for Translational Health Research, Woodville South, Australia
Background and Aim: Incidence of non-alcoholic fatty liver disease (NAFLD) is rising. Risk factors for progression to cirrhosis include obesity (over nutrition), type 2 diabetes (T2DM), and westernised diets. Paradoxically, sarcopenia and malnutrition (under nutrition), accelerate disease progression. Clinical guidelines for liver disease recommend early allied health intervention to slow disease progression. This study aimed to determine modifiable nutrition and metabolic risk prevalence in a South Australian outpatient hepatology service without allied health integration for NAFLD and related cirrhosis.
Methods: This cross-sectional study used convenience sampling between July and November 2023. Malnutrition universal screening tool score (MUST ≥2) defined risk while subjective global assessment (SGA, scores of B or C) diagnosed malnutrition. Sarcopenia risk was defined by the SARC-F questionnaire (score of ≥4). Anthropometrics included waist circumference and body mass index (BMI). Previous allied health interventions were assessed. Habitual diet was scored against a Mediterranean diet index (MED-Score).
Results: Thirty-two participants consented to participate (median age 63 (Interquartile range (IQR) 55.5-70.8) years; 44% male). Table 1 summarises the cardiometabolic and nutrition risks. Prevalence of sarcopenia and malnutrition risk was low (median SARC-F scores=1 (IQR 0-2), and all had MUST >2. Three (9.4%) participants were malnourished (SGA B). Fifteen participants (46%) had been referred to a dietitian previously.
Conclusion: Modifiable nutrition or metabolic risk factors in NAFLD and associated cirrhosis were prevalent, but can be optimised with diet and lifestyle intervention. Establishing tertiary referral pathways from Hepatology services to allied health is essential to manage modifiable risk factors to improve patient outcomes.
190
High Mediterranean diet adherence reduces risk of cancer and improves cancer survivorship
Daniel Clayton-chubb1,2, Jessica Fitzpatrick1,2, Andrew T Chan3, Elena George4, Alex Boussioutas1,2, John McNeil2, Robyn Woods2, Alice Owen2, William Kemp1,2, Ammar Majeed1,2 and Stuart Roberts1,2
1Alfred Health, Melbourne, Australia;2Monash University, Melbourne, Australia;3Harvard Medical School, Boston, USA;4Deakin University, Melbourne, Australia
Background and Aim: While a Mediterranean diet (MedDiet) is commonly recommended in primary and specialist care, yet its role in reducing the risk of cancer, gastrointestinal (GI) cancer and improving cancer survivorship is understudied especially in older adults. As such, we aimed to determine whether MedDiet adherence (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with incident cancer, incident GI cancer, and survivorship in older Australian adults.
Methods: This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, which enrolled 12,581 participants. A MedDiet Score (MDS) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 18. Higher scores indicate greater adherence to a MedDiet style dietary pattern. Cancer incidence and sub-type were adjudicated by investigators based on medical records. Participants with cancer diagnosed during ASPREE prior to completion of the FFQ were excluded. GI cancer was defined as colorectal, gastric, gastro-oesophageal, liver, or pancreatic in origin. MDS was analysed in quartiles due to its non-linear association with incident GI cancer. Both unadjusted and adjusted cox regression were used in these analyses.
Results: We included the 12,394 participants (median 76.8 [IQR 74.6 – 80.3] years) who answered a semi-quantitative FFQ while living at home/with family during ALSOP. Of these, 563 (4.5%) developed cancer during ASPREE but pre-questionnaire and were excluded and 10 had incomplete data. The remaining 11,831 were subsequently followed up for a median of 5.8 (IQR 4.6 – 6.5) years. Of these 11,4831, 1629 (13.8%) developed cancer, of which 344 (2.9% overall) were GI cancers. The mean (± SD) MDS was 11.1 (± 2.0). Univariate analysis showed higher adherence to a MedDiet was associated with a reduced hazard of all cancer (Q4 vs Q1 HR 0.71 [95% CI 0.62 – 0.81]) and GI cancer specifically (Q4 vs Q1 HR 0.70 [95% CI 0.51 – 0.95]) (Figure 1). Results remained significant for all cancer when adjusting for age, sex, BMI, alcohol and smoking status, ethnicity, diabetes, aspirin use, education, and participant history of cancer pre-dating ASPREE (all cancer Q1 vs Q4 aHR 0.85 [95% CI 0.74 – 0.99] but not GI cancer Q1 vs Q4 aHR 0.82 [95% CI 0.60 – 1.13]). In those who developed cancer, higher MDS was associated with reduced all-cause mortality (Q4 vs Q1 aHR 0.73 [95% CI 0.56 – 0.96]), though not in the GI cancer subgroup (Q4 vs Q1 aHR 0.87 [95% CI 0.53 – 1.43]).
191
Ultra-processed food is associated with death and dementia in older Australian adults
Daniel Clayton-chubb1,2, Jessica Fitzpatrick1,2, Priscila Machado4, William Kemp1,2, Alice Owen2, John McNeil2, Robyn Woods1,2, Joanne Ryan1,2, Ammar Majeed1,2, Andrew T Chan3 and Stuart Roberts1,2
1Alfred Health, Melbourne, Australia;2Monash University, Melbourne, Australia;3Harvard Medical School, Boston, USA;4Deakin University, Melbourne, Australia
Background and Aim: There is a growing body of evidence linking high Ultra-Processed Foods (UPFs) intake with deleterious health outcomes, including mortality and cognitive dysfunction. However, there are less data on the risks of high UPF intake in older adults. As such, we aimed to determine whether a high UPF diet (via semi-quantitative food-frequency questionnaires [FFQs]) was associated with mortality or incident dementia in older Australian adults.
Methods: This study is a non-pre-specified post hoc analysis of the ASPirin in Reducing Events in the Elderly (ASPREE) randomized trial and the ASPREE Longitudinal Study of Older Persons (ALSOP) sub-study, with 12,581 respondents. A UPF Diet Score (UPFQ) was developed based on self-reported eating patterns for the preceding 12 months via a 54-item FFQ, giving a potential score ranging from 0 to 25. Higher scores indicate greater exposure to UPFs. Mortality and incident dementia were adjudicated by investigators based on medical records. Participants with dementia diagnosed during ASPREE prior to completion of the FFQ were excluded in dementia analyses, as were those with more than 20% missing UPF FFQ data. UPFQ was analysed in quartiles due to its non-linear association with all-cause mortality, and linearly for incident dementia. The nadir quartile was used as the reference for Cox models.
Results: We included the 11,962 participants living home alone or with family (median [IQR] 76.8 [74.6 – 80.2] years) who adequately answered the FFQ during ALSOP. This group was followed up for a median of 5.9 (IQR 4.7 – 6.6) years. Of the included participants, 1,349 (11.3%) died. Sixty-six developed dementia pre-FFQ (0.6%) and were excluded from dementia analyses. The median (IQR) UPFQ was 6 (4.9 – 7.3). Univariate Cox Proportional Hazards Models showed higher UPF intake was associated with an increased hazard of all-cause mortality (Q4 vs Q2 HR 1.47 [95% CI 1.26 – 1.71]) and dementia (HR 1.09 [95% CI 1.04 – 1.14]). Results remained significant for mortality when adjusting for sex, BMI, age, smoking status, diabetes, renal function, cognitive function, depression, education, grip strength and gait speed (Q4 vs Q2 aHR 1.31 [95% CI 1.12 – 1.55]). Similarly, when fully adjusted, for every one-point increase in UPFQ there was an increased risk of dementia (aHR 1.08 [95% CI 1.03 – 1.14]). The increase in mortality impacted cardiovascular death (including stroke), cancer death, and other causes similarly (χ2 p-value = 0.687). Results remained significant when excluding those with less than 12 months of follow-up.
195
Quality over quantity: How can the quality of therapeutic diets be assessed for inflammatory bowel disease in Australia?
Laura Portmann1,2, Jessica Fitzpatrick3,4, Emma Halmos3,4, Robert Bryant1,2,5 and Alice Day1,2,5
1The Queen Elizabeth Hospital, Woodville South, Australia;2Basil Hetzel Institute, Woodville South, Australia;3Monash University, Melbourne, Australia;4Alfred Health, Melbourne, Australia;5The University of Adelaide, Adelaide, Australia
Background and Aim: Examining the quality of diets used to treat inflammatory bowel disease (IBD) is challenging as traditional dietary analysis methods are used to quantitatively assess food group and nutrient intakes, not overall diet quality. Yet, evidence is suggesting dietary patterns of differing quality such as ultra-processed foods or the Mediterranean diet (MED), rather than specific food components may be more predictive of disease onset and course. An IBD-specific diet quality index (DQI) does not exist. It is therefore unknown which DQI is most suitable to use in therapeutic IBD diet trials. This review aimed to identify current DQIs and assess their suitability for use on therapeutic diets in an Australian IBD population.
Methods: Electronic databases, MEDLINE and EmCare, were systematically searched for a-priori, food-based DQI reflecting national dietary guidelines and/or latest nutrition science for adults published 2013 to 2023, in English language. Excluded were DQI that were posteriori or for specific, non-IBD diseases (e.g., diabetes). Data extracted were adapted from optimal DQI criteria described by Burggraf et al.,1 which include quality measures of adequacy, moderation, variety and balance for food and nutrient components and DQI evaluation, as well as its use, if any, for IBD health outcomes.
Results: Twenty-five articles describing 25 DQI were included in final analysis. Sixteen DQI were adapted from existing DQI. Dietary guidelines were used to develop 19/25 (76%) DQI, while the remaining six were developed from dietary patterns (e.g., MED, EAT-Lancet Diet). Whole food groups were assessed by all DQI, but assessment of individual foods within groups varied. Ultra-processed foods were assessed in 16/25 (64%) DQI. No DQI included all optimal DQI criteria1. The Dietary Guideline Index 2013 (DGI-2013) most closely met DQI criteria, followed by the Healthy Eating Index for Australian Adults-2013 (HEIFA-2013) (Table 1). Seven of 25 DQI were Australian population specific. All Australian DQI evaluated adequacy, however assessment of other quality dimensions and scoring methods varied as outlined in Table 1. All except one Australian DQI were applied to food frequency questionnaires (FFQ). Eleven of 25 (44%) DQI, yet only two Australian DQI were not weighted equally to account for different weighted contributions of foods and nutrients to established health and disease outcomes. Seventeen of 25 (68%) DQI were validated, however few were evaluated for reproducibility (2/25) or reliability (7/25). No DQI was validated to assess gut-specific health outcomes. Two DQI (Dietary Diversity Score and Australian Recommended Food Score (ARFS)) were used to assess against gut microbiota. The DGI-2013 and Dutch Healthy Diet index-2015 were applied to FFQ from various IBD participants.
Reference
1. Burggraf, C., Teuber, R., Brosig, S., & Meier, T. (2018). Review of a priori dietary quality indices in relation to their construction criteria. Nutrition reviews, 76(10), 747-764.
206
Systematic scoping review: dietary interventions for the treatment of primary sclerosing cholangitis
Caitlin Theron1,2, Robert Bryant1,2, Damjana Bogatic1,2 and Alice Day1,2
1The Queen Elizabeth Hospital Gastroenterology Department, Adelaide, Australia;2Basil Hetzel Institute, Adelaide, Australia
Background and Aim: Primary sclerosing cholangitis (PSC), is a rare autoimmune liver disease with no effective medical therapies. The etiopathogenesis of PSC is incompletely understood, however evolving evidence suggests dysbiosis of the gut microbiota may play a key role. Diet is an important fertiliser of gut microbiota and has potential to be a modifiable risk factor in PSC. This review aims to scope available evidence of dietary factors that may influence PSC disease course.
Methods: A systematic scoping search of electronic databases EMBASE, EMCARE, MEDLINE and CINAL was carried out. Key search terms included primary sclerosing cholangitis, diet, nutrition, therapy, and gut microbial diversity. Included articles were original, peer-reviewed research and case reports, both human and pre-clinical models, that produced evidence of a diet or nutrient that contributed any effect to disease stabilisation, progression, symptoms, gut microbes, or survival rate associated with PSC.
Results: Of 1466 articles screened, 15 were included for review including four pre-clinical PSC models and 13 in humans. Outcome measures varied across studies, however most (8/15, 53%) assessed a change in biochemical parameters associated with poor patient outcomes, as outlined in Table 1. In human studies, the addition of retinoic acid for patient’s taking ursodeoxycholic acid (UDCA) was the only intervention found to significantly change one of the liver function tests, causing a reduction in alanine transferase (ALT). In mouse models of PSC, geniposide and berberine significantly reduced alkaline phosphatase (ALP), aspartate aminotransferase (AST) and ALT. No other interventions were found to significantly alter biochemical parameters. Survival rates were increased by coffee in patients with PSC (p=0.02), and by vitamin D in a PSC mouse model (p=0.01). Regarding symptoms, pruritis and abdominal pain were improved by N-acetylcysteine (p value not reported), while dietary fiber had no significant effect on pruritus (p value not reported). Only one article examined the effect of the intervention on the gut microbiome, finding that berberine reduced gut permeability (p<0.001), increased Bacteroidetes and decreased Firmicutes (p values not reported).
Conclusion: There are limited well designed clinical trials and data evaluating diet in PSC disease course. Of existing evidence, few dietary interventions significantly altered biochemical parameters associated with disease progression, including retinoic acid, geniposide and berberine. Only one article provided data on the relationship between the dietary factor, the gut microbiome and PSC disease course. Further research should include well-designed clinical trials that investigate the role of dietary factors in disease progression and the role of diet as a microbial restoration therapy.
223
Practical application of evidence-based dietary therapy into inflammatory bowel disease care shows high patient satisfaction and compliance, and improved disease activity: The DELECTABLE program
Gina Trakman1,2,3, Erin Russell1,2, Amy Hamilton1,2, Amy Wilson-o'brien1,2, Emily Thompson1, Natalie Simmance1, Ola Niewiadomski1 and Michael Kamm1,2
1St Vincent's Hospital Melbourne, Melbourne, Australia;2University of Melbourne, Melbourne, Australia;3La Trobe University, Melbourne, Australia
Background and aims: A range of diets have been shown in controlled trials to be therapeutically effective in Inflammatory Bowel Diseases (IBD). Exclusive enteral nutrition (EEN) and the Crohn’s Disease Exclusion Diet (CDED) have confirmed efficacy in inducing remission in Crohn’s disease (CD). Low sulphur and plant-based diets are being investigated in ulcerative colitis (UC). Reducing ultra-processed, additive-containing food intake is emerging as important, given its role in initiating and perpetuating disease. IBD patients believe in the value of modifying diet to improve disease control. Yet there is no evidence for diet tolerability and benefit outside clinical trials. The DELECTABLE program, a dietitian-led telehealth service, aimed to evaluate the patient acceptability, compliance, and benefit of structured, evidence-based dietary therapy as part of routine clinical care.
Methods: In this open-label, prospective, interventional cohort program, patients with Crohn’s disease or an ileo-anal pouch were offered the CDED or a wholefood additive-free diet (WFD), patients with ulcerative colitis were offered a low-sulphur plant-based diet (UCD) or WFD, and patients with microscopic colitis were offered the WFD. The primary outcomes were diet satisfaction (modified DSAT-28: range 27 to 135), dietitian-rated compliance (range 1-6), and patient-rated compliance (range 1 -5). Secondary outcomes were the amount of food additive intake (validated food frequency questionnaire), quality of life (IBDQ9; range 7-49), disease activity score (CDAI in CD, partial Mayo score in UC), CRP, and faecal calprotectin. Baseline to Week 12 differences were assessed for the CDED and wholefood diet using the Paired T-test or Wilcoxon-sign-test. Inferential statistics were not conducted for disease activity on the UCD due to sample size.
Results: Of 165 patients referred, 76 enrolled in the program. Sixty-four (82%) (mean age 36; 53% male) of enrolled patients completed 12 weeks of diet therapy, with 15, 42 and 7 participants completing the CDED, WFD, and UCD, respectively. Diet satisfaction was high at Week 1 on CDED (median 79 out of 135) and did not significantly change at Week 12 (median 83 out of 135, P=0.212). Diet satisfaction improved on the WFD from Week 1 to 12 (84.1 vs 86.9, P = 0.03) (Figure 1, Panel B). Median dietitian-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/6 v 4/6, P=0.682; WFD: 3/5 vs 3/5, P=0.165; UCD: 4/6 vs 4/6, P=0.233). Likewise, median patient-rated compliance scores were high at Week 1 and did not change at Week 12 (CDED: 5/5 v 4/5, P=0.565; WFD: 4/5 vs 4/5, P=0.348; UCD: 4.5/5 vs 4/5, P=0.368) (Figure 1, Panel B). Quality of life increased from Week 1 to Week 12 on the CDED (35 vs 51, P<0.001) and the WFD (37.1 vs 48.3, P<0.001). With regard to food additive ingestion: on the WFD, there was a significant reduction in carboxymethylcellulose (P=0.02), carrageenan (P=0.013), sucralose (P=0.018) and sulphites (P=0.007) ingestion. On the UCD there was a significant reduction in daily intake of all food additives (aspartame P=0.043; others P <0.028). On the CDED, from baseline to Week 12, there was a reduction in CRP (7.5 vs 4.6, P=0.034), calprotectin (195 vs 62, P=0.045) and CDAI (153 vs 43, P=0.023). On the WFD from baseline to Week 12, there was a significant reduction in CDAI (50 vs 32, P= 0.027) and partial Mayo score (2 vs 0, P=0.004). On the UCD, there was no change from baseline to Week 12 CRP (0 vs 1), partial Mayo score (3 vs 3) or calprotectin (112 vs 174).
Conclusion: Implementation of well-balanced, effective diet therapies is feasible and well-accepted by patients with IBD, with a promising impact on disease activity.
255
Peripheral parenteral nutrition: an evaluation of utility and complications
Emma Bidgood1, Joanna Huang2, Elise Murphy3, Ralley Prentice4, Beth Hede2 and David Russell2,5
1Department of Allied Health (Clinical Nutrition), The Royal Melbourne Hospital, Parkville, Australia;2Department of Gastroenterology, The Royal Melbourne Hospital, Parkville, Australia;3Pharmacy Department, The Royal Melbourne Hospital, Parkville, Australia;4Department of Gastroenterology, Monash Medical Centre, Clayton, Australia;5Department of Medicine, Melbourne Medical School, The University of Melbourne, Parkville, Australia
Background and Aim: Peripheral parenteral nutrition (PPN) provides an alternative nutrition support strategy to centrally administered parenteral nutrition (PN) for specific patients requiring short-term PN. Previous studies have demonstrated limited utilization of PPN and variations in complication rates. This study aimed to evaluate PPN complications and usage at this center.
Methods: This was a single-center retrospective observational study of all adult patients who received at least 1 day of PPN from June 2018 to December 2023. Demographic and clinical data were collected including, complications, indications for PN and reason for PPN, duration of therapy, reason for cessation of PPN, nutritional status, energy and protein provision and central line insertion rates.
Results: A total of 381 patients were included, median age 62 [IQR 28-74] years, 235 males (61.7%). The most common indication for PN was ileus (n=153, 40%), followed by gastrointestinal obstruction (n=93, 24%). The median time on PPN was 3 [2-4] days. Patients received a median of 65% [55-75] of energy and 58% [50-69] of protein requirements with PPN. Malnutrition was diagnosed in 47.5% (n=181) of this cohort. Total complication rates were 8.7% (n=33) with cannula infiltration being the most common complication (6.6%, n=25). 213 (56%) patients proceeded to central line insertion.
Conclusion: PPN proved to be a safe and effective therapy for short-term PN when managed by a nutrition support team. PPN has the potential to attenuate short-term nutritional deficits and prevent CVAD insertion in selected patients, making it a valuable therapy in type 1 intestinal failure.
260
Low salt diet modifiers may not be necessary for all inpatients with liver cirrhosis
Annie Shanahan1, Stacey Sayers1, Nicole Barna1, Alison Stewart1, Kelly Ho2, Georgina Petrusma2, Veronika Pudikova2, Angela Taylor2, Qinfang Yang2, Han Yu2 and Erin Russell1
1Department of Nutrition and Dietetics, Monash Health, Australia;2Department of Nutrition, Dietetics and Food, Monash University, Australia
Background: An order for a high energy, high protein, low salt (HEHPLS) diet is common practice to support inpatients with liver cirrhosis. However, evidence suggests that a low salt (LS) diet can reduce palatability and hinder energy and protein intake in this patient group with increased nutrient needs. International guidelines recommend a ‘moderate’ daily salt restriction (1840-2760mg) for these patients. Clinicians were concerned that the LS diet modifier was unnecessarily limiting meal options. Automated oral nutrition supplements (ONS) are being considered. Therefore, a review of the energy, protein and sodium content of diet codes HEHPLS and high energy, high protein (HEHP) was conducted and compared with established clinical guideline reference ranges.
Methods: In September 2023, six dietetics students undertook a detailed menu review. Both the 28-day cycle cook-chill and the 7-day frozen meal ‘Smart Pack’ menus at our hospital network were reviewed. To ensure all menu options were captured, the full menu cycle was analysed on the online menu system by selecting three main meals and two snacks per day. A variety of meals and snacks were selected to reflect a typical choice of a patient across the days of the menus. Energy, protein and sodium content was then averaged. Results therefore reflect nutrition provision to patients, rather than actual patient consumption. Requirements of a ‘reference patient’ with BMI 25 and decompensated liver cirrhosis was utilised for comparison.
Results: The HEHPLS and the HEHP diets for both the cook-chill and frozen Smart Pack menus provided mean sodium levels within the reference range. The LS diet code modifier reduced average sodium level in the menus by 925mg for cook-chill and 539mg for the Smart pack menus (Figure 1). However, the LS diet code modifier also decreased weekly main meal options by 33% and 50% for the two menus, respectively (Table 1). The HEHPLS smart-pack had the highest protein provision (105g) and met reference requirements. There was a varied provision from the other diet codes, ranging from average 86-98g protein and 8.6-10.3 MJ, under the requirements of the reference patient (Table 1) without ONS.
308
Effects of an anti inflammatory diet on hepatic fibrosis and inflammation in patients with metabolic dysfunction- associated steatotic liver disease
Wai See Ma
Blacktown Hospital, Blacktown, Australia
Background: Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) is closely related with obesity, metabolic syndrome, and diabetes. Its prevalence is on the rise, affecting approximately 25% of the world’s population and 5.6M Australians adults (age ≥18). Limited therapeutic options exist for the condition, and the mainstay of treatment remains as lifestyle modification through diet and exercise. Whilst weight loss has a definite role to play in this condition, recent studies have suggested that inflammation also has a role in the pathogenesis of MASLD. An anti-inflammatory diet may be an additional therapeutic option, as the Mediterranean diet, a component in the anti-inflammatory diet, has been recommended as dietary intervention for MASLD.
Methods: A literature search on MEDLINE, EMBASE, SCOPUS and Cochrane Library was conducted in March 2023, using search terms “anti-inflammatory diet”, “Mediterranean diet”, or “Okinawan diet”, and “metabolic associated fatty liver disease”. Original research and review articles were summarised.
Results: Positive outcomes have been noted with the anti-inflammatory diet on MASLD, including anthroprometric measurements, Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), hepatic fibrosis, and inflammatory markers.
Conclusion: Our review indicated that an anti-inflammatory diet, such as the Mediterranean diet, is a useful therapeutic option in the management of MASLD. Whilst only limited cohort studies are available, with this positive relationship, further research in this field is required to draw more solid conclusions on the feasibility and utility of the anti-inflammatory diet on MASLD. It would be interesting and important to devise a diet which is not solely focused on weight loss, but rather combats the inflammatory pathway in the pathogesis of MASLD.
311
Nutritional assessment of patients with liver cirrhosis in the outpatient setting: a narrative review
Tsz Hong Yiu2, Stuart Bartlett1 and Zina Valaydon2
1University Of Melbourne, Melbourne, Australia;2Western Health, Melbourne, Australia
Background and Aim: Malnutrition in patients with Liver Cirrhosis (LC) is common and associated with increased rates of liver-related complications and overall mortality. Currently, consensus guidelines for assessment of malnutrition in LC are lacking, and many clinicians are unaware of the available nutritional assessment tools. This leads to underdiagnosis of malnutrition and suboptimal management of these patients. This narrative review evaluates existing nutritional assessment tools, with the aim of providing recommendations on suitable tools for implantation in the outpatient setting.
Methods: We reviewed 60 articles sourced from Ovid Medline, PubMed, Web of Science and CINAHL databases that met our inclusion criteria. These articles evaluated nutritional assessment tools in patients with LC attributed to alcohol-related liver disease, viral hepatitis and metabolic fatty liver disease.
Results: Our findings favor Royal Free Hospital-Nutritional Prioritising Tool as a screening tool for its ease of administration showing high sensitivity, specificity and prognostic value. Liver-Disease Undernutrition Screening Tool offers self-administration benefits and high sensitivity but may be inaccurate with variable specificity. Mini Nutritional Assessment-Short Form showed high-sensitivity and specificity but has limited studies investigating it. When malnutrition is suspected, anthropometric tools and body composition analysis can be employed. Easily conducted anthropometric tools of Triceps Skinfold Thickness assessing fat mass and Mid-Arm Muscle Circumference assessing muscle mass are recommended and utilising both of these account for the differing malnutrition pattern in males and females. While Body Mass Index shows low sensitivity, potentially due to fluid retention in LC. For Body composition analysis, bioelectrical Impedance analysis is cost-effective and shows reasonable sensitivity, specificity and reproducibility and thus is recommended. Similarly, Dual X-ray Absorptiometry is recommended due to consistent validity and relatively low cost with minimal radiation exposure while Computer Tomography is not recommended with low sensitivity and greater radiation exposure. Biochemical parameters albumin, Skin-Prick Hypersensitivity and Leucocyte count are not recommended due to correlation with severity of liver disease rather than malnutrition. While leptin shows promise, further investigation establishing specific cut-off values is required. Functional assessment using Hand grip strength is a simple measure for assessing sarcopenia, although its variable specificity requires further validation.
Conclusion: Recommended tools are Royal Free Hospital-Nutritional Prioritising Tool, Triceps Skinfold Thickness in females and Mid-Arm Muscle Circumference in males, Bioelectrical impedance Analysis and Dual-energy X-ray Absorptiometry. Further research should focus on developing tailored nutritional assessment tools accounting for the characteristics and unique challenges of liver cirrhosis to enhance diagnosis, management and outcomes.
312
Healthier dietary intake is positively associated with disease activity and inflammation in Australian adults with inflammatory bowel disease
Denelle Cosier1, Karen Charlton1, Kelly Lambert1, Julianna Lys de Sousa Alves Neri1, Marijka Batterham2, Sabrina Koentgen3, Nan Wu3, Paris Tavakoli3, Andrew Chung3, Anson Ho3, Simon Ghaly4, Susan J Connor5, Rupert Leong6, Nick J Talley7, Steven Leach8, Daniel Lemberg9, Shoma Dutt10 and Georgina Hold3
1School of Medical, Indigenous and Health Sciences, University of Wollongong, Wollongong, Country;2Statistical Consulting Centre, National Institute for Applied Statistical Research Australia, Wollongong, Australia;3Microbiome Research Centre, Faculty of Medicine and Health, University of New South Wales, Sydney, Australia;4Department of Gastroenterology and Hepatology, St Vincent’s Hospital Sydney and St Vincent’s Clinical School, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;5Department of Gastroenterology, Liverpool Hospital and South West Sydney Clinical Campuses, UNSW Medicine & Health, UNSW Sydney, Sydney, Australia;6Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;7School of Medicine and Public Health, University of Newcastle, Newcastle, Australia;8Discipline of Paediatrics, School of Clinical Medicine UNSW, Sydney, Australia;9Department of Gastroenterology, Sydney Children's Hospital, Sydney, Australia;10Department of Gastroenterology, The Sydney Children’s Hospital Network Randwick and Westmead, Sydney, Australia
Background and Aim: Diet has been considered as one driving factor in the onset of Inflammatory Bowel Disease (IBD), however the mechanisms of interplay between diet, inflammation and disease activity are unclear. Given people living with IBD perceive diet to be an important modifiable factor in their disease management, ongoing research is needed to provide specific dietary recommendations. We explored the relationship between dietary intake, disease activity and intestinal inflammation in an Australian adult cohort with and without IBD.
Methods: We analysed baseline dietary and clinical data from the Australian IBD Microbiome (AIM) study. AIM is a prospective longitudinal cohort study of adults and children with Crohn’s Disease (CD), Ulcerative colitis (UC) as well as healthy controls. Habitual dietary patterns were explored using Principal Component Analysis (PCA) from Food Frequency Questionnaire data (80-item validated tool; Cancer Council Victoria). The Dietary Inflammatory Index (DII) was computed from 3-day food records. Associations between diet, clinical disease activity from CD Activity Index (CDAI) or Partial Mayo scores (categorised as remission or active), and faecal calprotectin (FCP) were explored in adult participants.
Results: 412 adults (CD = 117, UC = 106, Healthy = 189) were included. FCP data was available for 211 participants (HC = 100, CD = 49, UC = 62). Median (IQR) FCP at baseline was 0 (0-0) μg/g for HC and 33 (0-147) μg/g for IBD (p<0.001), indicating no intestinal inflammation. Median (IQR) partial Mayo at baseline was 1 (0-1) and median CDAI at baseline was 92 (48 – 168), indicating clinical remission in UC and CD. A dietary pattern comprising of high plant diversity was positively associated with active CD (CDAI 159.3 [84.9-204.0], p 0.004), and a ‘Prudent’ dietary pattern (characterised by high intake of plant milk and nuts) was positively associated with high FCP levels in the combined IBD cohort (>150 μg/g, p=0.015). Mean DII score was pro-inflammatory (1.01 ± 1.65) across all cohorts, with no significant differences between healthy vs IBD, CD vs UC or active vs remission cohorts. In UC, a pro-inflammatory diet was associated with a reduced likelihood of having active disease (OR = 0.76, 95% CI [0.58-0.98]) and was associated with no intestinal inflammation (p=0.032).
Conclusion: Unexpectedly, healthier dietary patterns were positively associated with disease activity and higher FCP in Australian adults with IBD. Similarly, a pro-inflammatory diet was associated with disease remission in the UC cohort. Reverse causality cannot be ruled out, therefore, dietary modifications to manage active disease may explain the inverse association between healthier dietary intake and disease activity. Further longitudinal and clinical studies are needed to expand upon the findings.
400
A dietitian-led IBD clinic model is effective and efficient, with high patient satisfaction
Sarah Melton, Miles Sparrow, Kate Norton, Alex Boussioutas and Jessica Fitzpatrick
Alfred Health, Melbourne, Australia
Background and Aim: Dietary management plays a critical role in the management of IBD, including using diet to treat active disease, management of non-inflammatory symptoms, prevention and management of complications, identification and treatment of malnutrition and perioperative nutritional optimisation; yet many patients lack access to specialised dietetic care. This audit describes the evaluation and impact of a pilot dietitian-led IBD clinic model in a tertiary IBD centre.
Methods: A dietitian-led IBD clinic (0.4 dietetic EFT) was established and piloted for 6 months as part of a Nursing and Allied Health Lead Service model of care initiative. The clinic was designed to facilitate more rapid access to dietetic care for patients requiring priority assessment, with intervention frequency in line with best practice. This allowed diversion of stable patients from the regular IBD clinic to reduce frequency of medical review. Audit data was collected at each appointment by the clinic dietitian. Malnutrition was diagnosed according to GLIM1 criteria. Priority of referrals was determined by Dietitian Crohn’s Colitis Australian Network (DECCAN) triage tool and best practice. Redcap surveys were used to measure patient satisfaction with dietetic care. Patient information was obtained from medical records. Descriptive statistics were used to describe data.
Results: Seventy patients were referred to the dietitian, of whom 66 attended an initial appointment. A total of 165 appointments (162 TeleHealth, 3 face-to-face) were conducted in 6 months. Referrals were received from the standard IBD clinic and ward dietitians (47%), gastroenterologists (31%), IBD nurses (14%) or other/unknown sources (7%). Reasons for referral are presented in Figure 1. Median time from referral to assessment was 1 day (range 0-36 days) for urgent priority (within 7 days) patients (n=19), 3.5 days (range 1-36 days) for high (within 14 days) priority patients (n=6), 21 days (1-100 days) for moderate (within 30 days) priority patients (n=33) and 25.5 days (range 7-84 days) for low (within 90 days) priority patients (n=6). Eight patients (11%) were escalated to the gastroenterologist (IBD Fellow) due to suspected worsening disease activity, or other clinical concerns. Five patients (7%) were diagnosed with malnutrition as per GLIM criteria however the majority of appointments were conducted via Telehealth and physical assessments were not possible, therefore this is likely an under reporting. Of the patients discharged from the dietitian-led IBD service at the time of the audit, 79% achieved the goal of nutrition intervention. Patient engagement was high, with 90% of scheduled appointments attended. Patient satisfaction (15% survey response rate) was overwhelmingly high with 100% of patients reporting that the dietitian informed them adequately about nutrition and IBD, allowed for regular consultation, gave them confidence in the dietitian and felt that they were always taken seriously.
Conclusion: The dietitian-led IBD clinic model demonstrated effective specialised nutritional care within a multidisciplinary framework for IBD management. This approach led to dietetic assessment and intervention within desired and best practice timeframes (particularly for urgent and high priority patients), high patient engagement and satisfaction. Future studies should explore the impact of this model of care on clinical and nutritional outcomes, the scalability and long-term sustainability of this model, as well as financial analysis.
443
Dietary intake and nutrition interventions in pregnant women with inflammatory bowel disease: A systematic review
Emily Thompson1,2, Adrienne Forsyth2 and Adam Walsh2
1St Vincent's Hospital Melbourne, Melbourne, Australia;2Australian Catholic University, Melbourne, Australia
Background and Aim: Dietary intake during pregnancy influences maternal health and the health of future generations, including the risk of developing chronic diseases later in life. The prevalence of inflammatory bowel disease (IBD), a condition affecting women of reproductive age, is increasing worldwide. IBD is associated with nutrient deficiencies and malnutrition due to reduced nutrition intake, restrictive diets, impaired nutrient absorption and chronic inflammation. This review aimed to identify studies reporting on dietary intake, quality and patterns of pregnant women with IBD and to evaluate the scope and implementation of nutrition interventions.
Methods: Four electronic databases, Medline, CINAHL, Embase and Scopus, were systematically searched using the key terms “inflammatory bowel disease”, “pregnancy” and “dietary intake” in September 2023. Primary studies were included investigating food and nutrient intake, diet quality, dietary patterns, or the use of nutrition interventions in pregnant women aged 18 years or older with IBD. The risk of bias was assessed using the Joanna Briggs Institute checklists.
Results: 12 studies were included. Three studies reported on dietary intake, quality or dietary patterns in pregnant women with Crohn’s disease (CD) and Ulcerative Colitis (UC). Pregnant women with IBD did not meet food and nutrient intake targets recommended by national dietary guidelines. They were more likely to follow a dietary pattern resembling a Western diet and had lower protein intakes from dairy sources compared to pregnant women without IBD. Nine studies, eight of which were case reports or case series, reported on the use of nutrition interventions in women with CD including parenteral nutrition (PN) (n=5), elemental diet (n=2), peptide-based formula therapy (n=1), and the Crohn’s Disease Exclusion Diet (n=1). These interventions were found to be safe and well-tolerated.
Conclusion: This review highlights a scarcity of data on the dietary intake of pregnant women with IBD. The evidence supporting the use of nutrition interventions, including therapeutic diets during pregnancy, is primarily derived from a limited number of case reports and case series, with even less data available for UC than CD. Larger scale, high-quality studies are needed to improve nutrition management and support for pregnant women with IBD, addressing their nutritional risks and challenges, and optimising maternal health and the intergenerational transfer of health.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
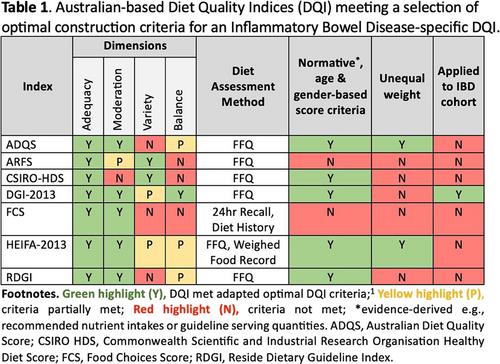



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
