{"title":"流明基础科学","authors":"","doi":"10.1111/jgh.16703","DOIUrl":null,"url":null,"abstract":"<p><b>92</b></p><p><b>Simethicone suppresses the growth of microbes cultured from the human duodenal mucosa</b></p><p>Thomas Fairlie<sup>1,2</sup>, Ayesha Shah<sup>1,2</sup>, Yenkai Lim<sup>2</sup>, Jing-Jie Teh<sup>2</sup>, Lauren Schooth<sup>2</sup>, Mark Morrison<sup>2</sup> and Gerald Holtmann<sup>1,2</sup></p><p><sup>1</sup><i>Princess Alexandria Hospital, Metro South Health, Woolloongabba, Australia;</i> <sup>2</sup><i>University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Small intestinal dysbiosis (SID) is known to play an important role in the pathophysiology of various gastrointestinal and extraintestinal disorders, with recent studies linking select members of the duodenal microbiota with symptom severity in functional dyspepsia (FD). Simethicone is routinely used during endoscopy as an anti-foaming agent and at lower concentrations used to alleviate painful gut symptoms associated with excessive gas and/or bloating. Here, we assessed the effects from simethicone on the growth of a mixed culture of duodenal mucosa-associated microbiota (MAM).</p><p><b><i>Methods:</i></b> The consortia of duodenal MAM recovered from the biopsies of a non-FD asymptomatic control subject were anaerobically cultured using a duodenal habitat-simulating medium with no addition, or supplemented with a commercially available source of Simethicone to provide final concentrations of 0.2 mg/ml (lowest effective dose for antifoaming effects, 1 mg/mL, 2 mg/mL or 4 mg/mL. Three biological replicates with six technical replicates of the cultures (and uninoculated controls) were prepared using a 96-well microtitre plate format within an anaerobic chamber, then microbial growth (optical density change at 600 nm) at 37 °C was measured every 30 minutes for 18 hours using an automated microtiter plate also housed within the anaerobic chamber. The R package Growthcurver was applied to assess the growth kinetic profiles by calculating the area under the curve and statistical comparisons to control cultures calculated with a paired t-test.</p><p><b><i>Results:</i></b> Relative to control cultures, the growth kinetic profile (area under the curve) after 18 hours was unaffected by the addition of 0.2 mg/mL simethicone (<i>P</i> = 0.99), but progressively reduced by the addition of greater simethicone concentrations (Fig. 1). The reduction of growth kinetics with 2 mg/mL simethicone approached significance (<i>P</i> = 0.059) and were significantly reduced with 4 mg/mL simethicone (<i>P</i> = 0.023).</p><p><b>139</b></p><p><b>A whole blood interleukin-2 release assay offers a novel approach to detect and monitor pathogenic T cells to support epitope discovery and drug development in coeliac disease and beyond</b></p><p><b>Olivia Moscatelli</b><sup>1</sup>, Amy Russell<sup>1</sup>, Lee Henneken<sup>2</sup>, Linda Fothergill<sup>1</sup>, Hugh Reid<sup>3</sup>, Jamie Rossjohn<sup>3</sup>, Melinda Hardy<sup>1</sup>, Vanessa Bryant<sup>1</sup> and Jason Tye-Din<sup>1</sup></p><p><sup>1</sup><i>Walter and Eliza Hall Institute, Parkville, Australia;</i> <sup>2</sup><i>The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>3</sup><i>Monash University, Clayton, Australia</i></p><p><b><i>Background and Aim:</i></b> Definition of the pathogenic gluten peptides in coeliac disease (CD) has afforded the opportunity to develop tools that assess the gluten-specific CD4 + T cells central to its pathogenesis. Current approaches support immune discovery (epitope mapping) and are employed in pre-clinical and clinical CD drug development as efficacy and proof-of-concept endpoints. However, current detection approaches are suboptimal: they necessitate gluten challenge to expand the T cells, which is unappealing to patients, or rely on HLA-gluten tetramers that are technically demanding. We showed interleukin (IL)-2 production is a marker of activated gluten-specific T cells and propose it offers a simpler approach. We assessed the performance of IL-2 release in an <i>in vitro</i> whole blood assay (WBA) before and after <i>in vivo</i> expansion of gluten-specific T cells by gluten-challenge and compared these readouts to the well-established functional T cell readout, IFN-γ enzyme-linked immunosorbent spot (ELISpot) assay.</p><p><b><i>Methods:</i></b> Adults with HLA-DQ2.5 + treated CD (n = 10) underwent assessment before and 6 days after commencing single-bolus 10 g gluten challenge. <i>In vitro</i> IL-2 release was assessed after whole blood was incubated with gluten peptides (IL-2 WBA), and peripheral blood mononuclear cells were assessed using the IFN-γ ELISpot to quantify activated gluten-specific T cells. The functional effects of gluten peptides of varying immunogenicity and pan-HLA-DQ blocking were compared across these approaches.</p><p><b><i>Results:</i></b> At baseline, positive responses to peptides encompassing immunodominant α-gliadin or ω-gliadin epitopes were seen in 70% (IL-2 WBA) and 10% (IFN-γ ELISpot). Six days post challenge, positive responses increased to 90% (IL-2 WBA) and 40% (IFN-γ ELISpot). IL-2 WBA responses ranked gluten peptide immunogenicity concordant with published data. Pan-HLA-DQ blocking reduced the IL-2 WBA response by mean 30-fold (Wilcoxon matched-pairs test, <i>P</i> = 0.002).</p><p><i><b>Conclusion:</b></i> Compared to traditional measures, the IL-2 WBA shows superior sensitivity to detect the gluten-specific T cell in CD patients even when they are following a gluten-free diet. It faithfully measures <i>in vivo</i> systemic responses to gluten and the functional blockade of HLA, supporting its role in testing the efficacy of drugs aiming to block gluten-specific T cell responses. This approach provides a tool for Phase 1/2 clinical trials to monitor the functional status of the pathogenic T cell while avoiding the need for gluten challenge, that can be poorly tolerated and negatively impact recruitment. The IL-2 WBA has promise as a research and clinical tool in a variety of autoimmune, allergic, malignant, and infectious diseases where T cells are important.</p><p><b>187</b></p><p><b>Coeliac disease and the stomach: Is this an under-recognised entity? A prospective case control study</b></p><p><b>Laura Hollingsworth</b><sup>1,2</sup>, Anthony Brownson<sup>1</sup> and Srikantaiah Manjunatha<sup>1</sup></p><p><sup>1</sup><i>Dunedin Hospital, Dunedin, New Zealand;</i> <sup>2</sup><i>Christchurch Hospital, Christchurch, New Zealand</i></p><p><b><i>Background and Aim:</i></b> Coeliac disease (CD) is an immune-mediated disorder triggered by the ingestion of gluten leading to small intestinal damage. Lymphocytic gastritis characterised by an increase in intraepithelial lymphocytes in the gastric mucosa has been associated with CD and a more aggressive coeliac phenotype. There is limited data regarding the prevalence of this association or sequelae and at present gastric biopsies are not standard or practice in CD across Australia or New Zealand. The aim of this study is to investigate the prevalence of gastric mucosal change including lymphocytic gastritis in patients with CD.</p><p><b><i>Methods:</i></b> This prospective case control study included a total of 44 adults referred to a tertiary public hospital gastroenterology department in New Zealand. The sample size was based on a 95% confidence level. Ethics was obtained in accordance with the Health Research Council of New Zealand. Twenty-four participants were included, referred with positive coeliac serology and 20 participants were included as a control arm - referred for dyspepsia without positive serology. All participants underwent a gastroscopy in accordance with national guidelines. In those with positive coeliac serology, biopsies were taken from the first and second part of the duodenum to assess for microscopic evidence of CD. Two biopsies were also taken from the stomach to assess for concurrent changes. In those referred for dyspepsia, the duodenum was evaluated for macroscopic changes during endoscopy. Duodenal biopsies were conducted if there was suspicion of CD and gastric biopsies were taken in all participants.</p><p><b><i>Results:</i></b> Of the 24 participants with positive coeliac serology, 20 had confirmed gluten sensitive enteropathy on duodenal biopsy. Histology from the gastric mucosa returned within normal limits in 16 cases. Chronic gastritis was found in 3 sampled participants and one gastric sample showed intestinal metaplasia. No gastric biopsies showed features of lymphocytic gastritis, atrophic gastritis or <i>Helicobacter pylori</i>. From the controls 19 gastric histology samples returned within normal limits and one showed reactive gastropathy (Table 1).</p><p><b>382</b></p><p><b>Colonic mucus attenuates the genotoxic effect of the <i>Bacteroides fragilis</i> toxin</b></p><p><b>Krista Dawson</b>, Andrew Day and Jacqueline Keenan</p><p><i>University Of Otago, Christchurch, New Zealand</i></p><p><b><i>Background and aims:</i></b> Enterotoxigenic <i>Bacteroides fragilis</i> (ETBF) is a pathogenic subspecies of <i>B. fragilis</i> that induces cleavage of E-cadherin and Interleukin (IL)-8 secretion in colonocytes. In experimental models using HT29 cells, ETBF has been shown to contribute to colorectal carcinogenesis through this mechanism. However, HT29 cells model colonocytes in isolation and fail to consider the role that secreted mucus has in protecting colonocytes <i>in vivo</i>. This study assessed whether mucus protects against the ETBF toxin using the mucus-secreting HT29 MTX-E12 cell line that more accurately models the colonic epithelium of a healthy individual.</p><p><b><i>Methods:</i></b> HT29 MTX-E12 cells were treated with fluorescently labelled ETBF for 24 hours. The ability for ETBF to infiltrate and degrade the mucus layer was quantified by assessing the relative abundance of MUC2 in cell lysates by immunoblot analysis, coupled with immunofluorescence microscopy. E-cadherin cleavage and IL-8 secretion were assessed in both HT29 and HT29 MTX-E12 cells by immunofluorescence microscopy and ELISA assay, respectively. Bacterial pellets were collected (pre-and post-culture) to quantify the levels of toxin (<i>bft</i>) expression following co-culture with mucus and non-mucus producing cells by RT-qPCR. For all experiments, a one-way ANOVA or unpaired <i>t</i>-test was used to assess differences between treated and untreated cells.</p><p><b><i>Results:</i></b> ETBF is capable of degrading colonic mucin. This was confirmed by the presence of bacteria within the mucus layer and a reduction in MUC2 expression in treated cells (<i>P</i> < 0.01). Despite this, no loss of E-cadherin or toxin-associated increase in IL-8 was observed in HT29 MTX-E12 cells treated with ETBF when compared to untreated controls. Moreover, the expression of the <i>bft2</i> gene was downregulated (<i>P</i> < 0.0001) after co-culture with the mucus-secreting HT29 MTX-E12 cell line. In contrast, E-cadherin was reduced (<i>P</i> < 0.05) and IL-8 release was increased (<i>P</i> < 0.05) in HT29 cells treated with ETBF when compared with untreated controls, while <i>bft2</i> expression levels remained comparable to the zero-hour control following co-culture with the non-mucus producing HT29 cell line (<i>P</i> > 0.05).</p><p><b><i>Conclusions:</i></b> The colonic mucus barrier plays an essential role in maintaining gut homeostasis and is an important aspect to consider when modelling host-pathogen interactions <i>in vitro</i>. The results of this study indicate that the colonic mucus layer protects against the pathogenic effects of ETBF by regulating the expression of the <i>bft</i> toxin. Although <i>B. fragilis</i> exhibits the capacity to degrade colonic mucin, this alone was not sufficient to negate the protective attributes of the mucus barrier within this experimental timeframe.</p><p><b>395</b></p><p><b>Establishing intestinal organoid-microbe co-culture model to study host–microbe interactions</b></p><p><b>Ghanyah Al-Qadami</b><sup>1</sup>, Ilka Priebe<sup>1</sup>, Maryam Hor<sup>1</sup>, Rajvinder Singh<sup>2</sup>, Anna Wawer<sup>2</sup> and Kim Fung<sup>3</sup></p><p><sup>1</sup><i>CSIRO, Adelaide, Australia;</i> <sup>2</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>3</sup><i>CSIRO, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> The gastrointestinal tract is home to trillions of microorganisms that play a key role in human health and disease. The recent advancement in microbial detection technologies and next-generation sequencing tools has allowed us to identify and characterise most of these microbes. However, due to the complexity of the intestinal microenvironment, the exact mechanisms by which these microbes influence intestinal health and disease are yet to be explored. Intestinal organoids, 3D mini-intestines that recapitulate both the architecture and the cellular diversity of the intestinal epithelium, have emerged as a powerful tool for studying host-microbiome interactions in a reductionist yet biologically relevant model. As such, this project aims to develop an intestinal organoid-microbe co-culture model to investigate the interaction between microbes and epithelial cells in the organoids.</p><p><b><i>Methods:</i></b> 3D human intestinal organoids were generated from adult intestinal stem cells isolated from intestinal tissue biopsies. Apical-out organoids – 3D organoids with reversed epithelial polarity so the apical surface is facing outward – and organoid-derived monolayer (ODM) were also established. The oral microbe <i>Fusobacterium nucleatum</i> was used as a model microorganism to develop the co-culture model. <i>F. nucleatum</i> was co-cultured with the organoids and its viability in the co-culture system was assessed.</p><p><i><b>Results:</b> Ex vivo</i> intestinal organoids, apical-out organoids, and ODM were successfully generated from intestinal tissue biopsy samples. A co-culture model was developed using three approaches i) microinjection of <i>F. nucleatum</i> into the organoid lumen, ii) <i>F. nucleatum</i> incubation with apical-out organoids, and iii) <i>F. nucleatum</i> incubation with ODM. Bacterial viability analysis confirmed that <i>F. nucleatum</i> retains its viability when incubated with organoids.</p><p><i><b>Conclusion:</b></i> Organoid co-culture with <i>F. nucleatum</i> was successfully established. In future work, we aim to investigate how <i>F. nucleatum</i> influences the intestinal epithelium by measuring DNA damage, intestinal barrier integrity, inflammatory responses, and changes in gene expression.</p><p><b>542</b></p><p><b>The duodenal mucosa-associated microbiota differs in patients based on their Rome IV classification, and has variable effects on duodenal spheroid barrier function subjects</b></p><p><b>Lauren Schooth</b><sup>1,6</sup>, Grace Burns<sup>4,5,7</sup>, Kyra Minahan<sup>4,5,7</sup>, Jing-Jie Teh<sup>8</sup>, Tom Fairlie<sup>2,3</sup>, Ayesha Shah<sup>2,3,6</sup>, Gerald Holtmann<sup>2,3,6</sup> and Mark Morrison<sup>1,2,6</sup></p><p><sup>1</sup><i>The University of Queensland, Woollongabba, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Woollongabba, Australia;</i> <sup>3</sup><i>Faculty of Medicine, The University of Queensland, Brisbane, Australia;</i> <sup>4</sup><i>Faculty of Health and Medicine, University of Newcastle, Callaghan, Australia;</i> <sup>5</sup><i>Hunter Medical Research Insitute, New Lambton Heights, Australia;</i> <sup>6</sup><i>NHMCR Center of Research Excellence for Digestive Health, Brisbane, Australia;</i> <sup>7</sup><i>NHMCR Center of Research Excellence for Digestive Health, Newcastle, Australia;</i> <sup>8</sup><i>Centre for Microbiome Research, Queensland University of Technology, Woolloongabba, Australia</i></p><p><b><i>Background and Aim:</i></b> The socioeconomic burdens from gastrointestinal diseases and disorders continue to rise globally, and knowledge gaps remain that constrain efforts to improve their advanced diagnosis and treatment. Microbial involvement in these conditions is now widely recognised and includes specialised communities of mucosa-associated microbes. However, relatively little is known about this “forgotten microbiome”, particularly so for the proximal small intestine. Here, we seek to overcome this knowledge gap through a novel combination of microbe culture and metagenomics. We first characterize and differentiate the duodenal mucosa-associated microbiota (d-MAM) in subjects with disorders of gut brain interaction (DGBI). Next, we examine how the barrier function of duodenal spheroid cultures is affected on exposure to secreted products arising from these d-MAM cultures.</p><p><b><i>Methods:</i></b> Biopsies of duodenal tissue collected from 19 patients with DGBI (Rome IV classification) and 17 non-DGBI control subjects with no significant gastrointestinal symptoms and negative findings on endoscopy were used to inoculate a duodenal habitat-simulating medium. The diversity and functional attributes of the d-MAM recovered from these samples was produced by 16S RNA gene profiling and shotgun metagenomic sequencing (MGS) respectively. In parallel, the d-MAM cultures from each subject were filter sterilised to recover their “secretomes” of metabolites and other small molecules produced during growth. A select number of these secretomes were then used to challenge the barrier integrity of 9 different duodenal spheroid cultures produced using tissue from 3 non-DGBI “control” subjects and 3 subjects each with functional dyspepsia exclusively (FD), or with overlapping symptoms of the irritable bowel syndrome (FD/IBS). To that end, the duodenal spheroids were propagated as monolayers in transwells, and exposed to 1:5 dilutions of the chosen secretomes within the apical compartment. Trans-epithelial resistance (TEER) was measured at baseline, 6 and 24 hours.</p><p><b><i>Results:</i></b> Profiling of the d-MAM from these 36 subjects revealed not only differences between the DGBI and non-DGBI subjects, but the DGBI subjects could be further differentiated according to their Rome IV-based classifications. Specifically, the d-MAM of subjects diagnosed with FD exclusively could be differentiated from those with FD/IBS, and evidence of further differences was apparent in the d-MAM of subjects assigned to different subcategories within those diagnosed with IBS. The deep metagenomic sequencing also suggest species-level differences of the microbes recovered from these d-MAM communities. Based on the TEER measurements there were no clear interactions between secretome and spheroid response based on their respective DGBI classifications. However, the spheroid cultures derived from the non-DGBI subjects did show an improved recovery on secretome challenge relative to those derived from DGBI-subjects; suggesting the barrier integrity of spheroids from non-DGBI subjects is more resilient to the microbial secretomes than those from the DGBI subjects.</p><p><i><b>Conclusions:</b></i> Collectively, the findings presented here demonstrate the d-MAM not only differs between DGBI and non-DGBI subjects, but there are also microbial “biomarkers” of specific Rome IV symptom profiles, thereby offering new targets to advance the diagnosis and treatment options for DGBI. Our preliminary studies with duodenal spheroid cultures also suggests that barrier integrity can be measured and quantified in response to the d-MAM secretome preparations. As such, this approach brings “microbial genomes to life” and new ways to biologically reveal the key host–microbe interactions inherent to the underlying causes of different DGBI. By doing so, strategies to provide a more predictable and permanent relief from these debilitating conditions are more likely to be realised and expedited.</p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":"39 S1","pages":"262-265"},"PeriodicalIF":3.4000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16703","citationCount":"0","resultStr":"{\"title\":\"Luminal Basic Science\",\"authors\":\"\",\"doi\":\"10.1111/jgh.16703\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>92</b></p><p><b>Simethicone suppresses the growth of microbes cultured from the human duodenal mucosa</b></p><p>Thomas Fairlie<sup>1,2</sup>, Ayesha Shah<sup>1,2</sup>, Yenkai Lim<sup>2</sup>, Jing-Jie Teh<sup>2</sup>, Lauren Schooth<sup>2</sup>, Mark Morrison<sup>2</sup> and Gerald Holtmann<sup>1,2</sup></p><p><sup>1</sup><i>Princess Alexandria Hospital, Metro South Health, Woolloongabba, Australia;</i> <sup>2</sup><i>University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Small intestinal dysbiosis (SID) is known to play an important role in the pathophysiology of various gastrointestinal and extraintestinal disorders, with recent studies linking select members of the duodenal microbiota with symptom severity in functional dyspepsia (FD). Simethicone is routinely used during endoscopy as an anti-foaming agent and at lower concentrations used to alleviate painful gut symptoms associated with excessive gas and/or bloating. Here, we assessed the effects from simethicone on the growth of a mixed culture of duodenal mucosa-associated microbiota (MAM).</p><p><b><i>Methods:</i></b> The consortia of duodenal MAM recovered from the biopsies of a non-FD asymptomatic control subject were anaerobically cultured using a duodenal habitat-simulating medium with no addition, or supplemented with a commercially available source of Simethicone to provide final concentrations of 0.2 mg/ml (lowest effective dose for antifoaming effects, 1 mg/mL, 2 mg/mL or 4 mg/mL. Three biological replicates with six technical replicates of the cultures (and uninoculated controls) were prepared using a 96-well microtitre plate format within an anaerobic chamber, then microbial growth (optical density change at 600 nm) at 37 °C was measured every 30 minutes for 18 hours using an automated microtiter plate also housed within the anaerobic chamber. The R package Growthcurver was applied to assess the growth kinetic profiles by calculating the area under the curve and statistical comparisons to control cultures calculated with a paired t-test.</p><p><b><i>Results:</i></b> Relative to control cultures, the growth kinetic profile (area under the curve) after 18 hours was unaffected by the addition of 0.2 mg/mL simethicone (<i>P</i> = 0.99), but progressively reduced by the addition of greater simethicone concentrations (Fig. 1). The reduction of growth kinetics with 2 mg/mL simethicone approached significance (<i>P</i> = 0.059) and were significantly reduced with 4 mg/mL simethicone (<i>P</i> = 0.023).</p><p><b>139</b></p><p><b>A whole blood interleukin-2 release assay offers a novel approach to detect and monitor pathogenic T cells to support epitope discovery and drug development in coeliac disease and beyond</b></p><p><b>Olivia Moscatelli</b><sup>1</sup>, Amy Russell<sup>1</sup>, Lee Henneken<sup>2</sup>, Linda Fothergill<sup>1</sup>, Hugh Reid<sup>3</sup>, Jamie Rossjohn<sup>3</sup>, Melinda Hardy<sup>1</sup>, Vanessa Bryant<sup>1</sup> and Jason Tye-Din<sup>1</sup></p><p><sup>1</sup><i>Walter and Eliza Hall Institute, Parkville, Australia;</i> <sup>2</sup><i>The Royal Melbourne Hospital, Parkville, Australia;</i> <sup>3</sup><i>Monash University, Clayton, Australia</i></p><p><b><i>Background and Aim:</i></b> Definition of the pathogenic gluten peptides in coeliac disease (CD) has afforded the opportunity to develop tools that assess the gluten-specific CD4 + T cells central to its pathogenesis. Current approaches support immune discovery (epitope mapping) and are employed in pre-clinical and clinical CD drug development as efficacy and proof-of-concept endpoints. However, current detection approaches are suboptimal: they necessitate gluten challenge to expand the T cells, which is unappealing to patients, or rely on HLA-gluten tetramers that are technically demanding. We showed interleukin (IL)-2 production is a marker of activated gluten-specific T cells and propose it offers a simpler approach. We assessed the performance of IL-2 release in an <i>in vitro</i> whole blood assay (WBA) before and after <i>in vivo</i> expansion of gluten-specific T cells by gluten-challenge and compared these readouts to the well-established functional T cell readout, IFN-γ enzyme-linked immunosorbent spot (ELISpot) assay.</p><p><b><i>Methods:</i></b> Adults with HLA-DQ2.5 + treated CD (n = 10) underwent assessment before and 6 days after commencing single-bolus 10 g gluten challenge. <i>In vitro</i> IL-2 release was assessed after whole blood was incubated with gluten peptides (IL-2 WBA), and peripheral blood mononuclear cells were assessed using the IFN-γ ELISpot to quantify activated gluten-specific T cells. The functional effects of gluten peptides of varying immunogenicity and pan-HLA-DQ blocking were compared across these approaches.</p><p><b><i>Results:</i></b> At baseline, positive responses to peptides encompassing immunodominant α-gliadin or ω-gliadin epitopes were seen in 70% (IL-2 WBA) and 10% (IFN-γ ELISpot). Six days post challenge, positive responses increased to 90% (IL-2 WBA) and 40% (IFN-γ ELISpot). IL-2 WBA responses ranked gluten peptide immunogenicity concordant with published data. Pan-HLA-DQ blocking reduced the IL-2 WBA response by mean 30-fold (Wilcoxon matched-pairs test, <i>P</i> = 0.002).</p><p><i><b>Conclusion:</b></i> Compared to traditional measures, the IL-2 WBA shows superior sensitivity to detect the gluten-specific T cell in CD patients even when they are following a gluten-free diet. It faithfully measures <i>in vivo</i> systemic responses to gluten and the functional blockade of HLA, supporting its role in testing the efficacy of drugs aiming to block gluten-specific T cell responses. This approach provides a tool for Phase 1/2 clinical trials to monitor the functional status of the pathogenic T cell while avoiding the need for gluten challenge, that can be poorly tolerated and negatively impact recruitment. The IL-2 WBA has promise as a research and clinical tool in a variety of autoimmune, allergic, malignant, and infectious diseases where T cells are important.</p><p><b>187</b></p><p><b>Coeliac disease and the stomach: Is this an under-recognised entity? A prospective case control study</b></p><p><b>Laura Hollingsworth</b><sup>1,2</sup>, Anthony Brownson<sup>1</sup> and Srikantaiah Manjunatha<sup>1</sup></p><p><sup>1</sup><i>Dunedin Hospital, Dunedin, New Zealand;</i> <sup>2</sup><i>Christchurch Hospital, Christchurch, New Zealand</i></p><p><b><i>Background and Aim:</i></b> Coeliac disease (CD) is an immune-mediated disorder triggered by the ingestion of gluten leading to small intestinal damage. Lymphocytic gastritis characterised by an increase in intraepithelial lymphocytes in the gastric mucosa has been associated with CD and a more aggressive coeliac phenotype. There is limited data regarding the prevalence of this association or sequelae and at present gastric biopsies are not standard or practice in CD across Australia or New Zealand. The aim of this study is to investigate the prevalence of gastric mucosal change including lymphocytic gastritis in patients with CD.</p><p><b><i>Methods:</i></b> This prospective case control study included a total of 44 adults referred to a tertiary public hospital gastroenterology department in New Zealand. The sample size was based on a 95% confidence level. Ethics was obtained in accordance with the Health Research Council of New Zealand. Twenty-four participants were included, referred with positive coeliac serology and 20 participants were included as a control arm - referred for dyspepsia without positive serology. All participants underwent a gastroscopy in accordance with national guidelines. In those with positive coeliac serology, biopsies were taken from the first and second part of the duodenum to assess for microscopic evidence of CD. Two biopsies were also taken from the stomach to assess for concurrent changes. In those referred for dyspepsia, the duodenum was evaluated for macroscopic changes during endoscopy. Duodenal biopsies were conducted if there was suspicion of CD and gastric biopsies were taken in all participants.</p><p><b><i>Results:</i></b> Of the 24 participants with positive coeliac serology, 20 had confirmed gluten sensitive enteropathy on duodenal biopsy. Histology from the gastric mucosa returned within normal limits in 16 cases. Chronic gastritis was found in 3 sampled participants and one gastric sample showed intestinal metaplasia. No gastric biopsies showed features of lymphocytic gastritis, atrophic gastritis or <i>Helicobacter pylori</i>. From the controls 19 gastric histology samples returned within normal limits and one showed reactive gastropathy (Table 1).</p><p><b>382</b></p><p><b>Colonic mucus attenuates the genotoxic effect of the <i>Bacteroides fragilis</i> toxin</b></p><p><b>Krista Dawson</b>, Andrew Day and Jacqueline Keenan</p><p><i>University Of Otago, Christchurch, New Zealand</i></p><p><b><i>Background and aims:</i></b> Enterotoxigenic <i>Bacteroides fragilis</i> (ETBF) is a pathogenic subspecies of <i>B. fragilis</i> that induces cleavage of E-cadherin and Interleukin (IL)-8 secretion in colonocytes. In experimental models using HT29 cells, ETBF has been shown to contribute to colorectal carcinogenesis through this mechanism. However, HT29 cells model colonocytes in isolation and fail to consider the role that secreted mucus has in protecting colonocytes <i>in vivo</i>. This study assessed whether mucus protects against the ETBF toxin using the mucus-secreting HT29 MTX-E12 cell line that more accurately models the colonic epithelium of a healthy individual.</p><p><b><i>Methods:</i></b> HT29 MTX-E12 cells were treated with fluorescently labelled ETBF for 24 hours. The ability for ETBF to infiltrate and degrade the mucus layer was quantified by assessing the relative abundance of MUC2 in cell lysates by immunoblot analysis, coupled with immunofluorescence microscopy. E-cadherin cleavage and IL-8 secretion were assessed in both HT29 and HT29 MTX-E12 cells by immunofluorescence microscopy and ELISA assay, respectively. Bacterial pellets were collected (pre-and post-culture) to quantify the levels of toxin (<i>bft</i>) expression following co-culture with mucus and non-mucus producing cells by RT-qPCR. For all experiments, a one-way ANOVA or unpaired <i>t</i>-test was used to assess differences between treated and untreated cells.</p><p><b><i>Results:</i></b> ETBF is capable of degrading colonic mucin. This was confirmed by the presence of bacteria within the mucus layer and a reduction in MUC2 expression in treated cells (<i>P</i> < 0.01). Despite this, no loss of E-cadherin or toxin-associated increase in IL-8 was observed in HT29 MTX-E12 cells treated with ETBF when compared to untreated controls. Moreover, the expression of the <i>bft2</i> gene was downregulated (<i>P</i> < 0.0001) after co-culture with the mucus-secreting HT29 MTX-E12 cell line. In contrast, E-cadherin was reduced (<i>P</i> < 0.05) and IL-8 release was increased (<i>P</i> < 0.05) in HT29 cells treated with ETBF when compared with untreated controls, while <i>bft2</i> expression levels remained comparable to the zero-hour control following co-culture with the non-mucus producing HT29 cell line (<i>P</i> > 0.05).</p><p><b><i>Conclusions:</i></b> The colonic mucus barrier plays an essential role in maintaining gut homeostasis and is an important aspect to consider when modelling host-pathogen interactions <i>in vitro</i>. The results of this study indicate that the colonic mucus layer protects against the pathogenic effects of ETBF by regulating the expression of the <i>bft</i> toxin. Although <i>B. fragilis</i> exhibits the capacity to degrade colonic mucin, this alone was not sufficient to negate the protective attributes of the mucus barrier within this experimental timeframe.</p><p><b>395</b></p><p><b>Establishing intestinal organoid-microbe co-culture model to study host–microbe interactions</b></p><p><b>Ghanyah Al-Qadami</b><sup>1</sup>, Ilka Priebe<sup>1</sup>, Maryam Hor<sup>1</sup>, Rajvinder Singh<sup>2</sup>, Anna Wawer<sup>2</sup> and Kim Fung<sup>3</sup></p><p><sup>1</sup><i>CSIRO, Adelaide, Australia;</i> <sup>2</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>3</sup><i>CSIRO, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> The gastrointestinal tract is home to trillions of microorganisms that play a key role in human health and disease. The recent advancement in microbial detection technologies and next-generation sequencing tools has allowed us to identify and characterise most of these microbes. However, due to the complexity of the intestinal microenvironment, the exact mechanisms by which these microbes influence intestinal health and disease are yet to be explored. Intestinal organoids, 3D mini-intestines that recapitulate both the architecture and the cellular diversity of the intestinal epithelium, have emerged as a powerful tool for studying host-microbiome interactions in a reductionist yet biologically relevant model. As such, this project aims to develop an intestinal organoid-microbe co-culture model to investigate the interaction between microbes and epithelial cells in the organoids.</p><p><b><i>Methods:</i></b> 3D human intestinal organoids were generated from adult intestinal stem cells isolated from intestinal tissue biopsies. Apical-out organoids – 3D organoids with reversed epithelial polarity so the apical surface is facing outward – and organoid-derived monolayer (ODM) were also established. The oral microbe <i>Fusobacterium nucleatum</i> was used as a model microorganism to develop the co-culture model. <i>F. nucleatum</i> was co-cultured with the organoids and its viability in the co-culture system was assessed.</p><p><i><b>Results:</b> Ex vivo</i> intestinal organoids, apical-out organoids, and ODM were successfully generated from intestinal tissue biopsy samples. A co-culture model was developed using three approaches i) microinjection of <i>F. nucleatum</i> into the organoid lumen, ii) <i>F. nucleatum</i> incubation with apical-out organoids, and iii) <i>F. nucleatum</i> incubation with ODM. Bacterial viability analysis confirmed that <i>F. nucleatum</i> retains its viability when incubated with organoids.</p><p><i><b>Conclusion:</b></i> Organoid co-culture with <i>F. nucleatum</i> was successfully established. In future work, we aim to investigate how <i>F. nucleatum</i> influences the intestinal epithelium by measuring DNA damage, intestinal barrier integrity, inflammatory responses, and changes in gene expression.</p><p><b>542</b></p><p><b>The duodenal mucosa-associated microbiota differs in patients based on their Rome IV classification, and has variable effects on duodenal spheroid barrier function subjects</b></p><p><b>Lauren Schooth</b><sup>1,6</sup>, Grace Burns<sup>4,5,7</sup>, Kyra Minahan<sup>4,5,7</sup>, Jing-Jie Teh<sup>8</sup>, Tom Fairlie<sup>2,3</sup>, Ayesha Shah<sup>2,3,6</sup>, Gerald Holtmann<sup>2,3,6</sup> and Mark Morrison<sup>1,2,6</sup></p><p><sup>1</sup><i>The University of Queensland, Woollongabba, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Woollongabba, Australia;</i> <sup>3</sup><i>Faculty of Medicine, The University of Queensland, Brisbane, Australia;</i> <sup>4</sup><i>Faculty of Health and Medicine, University of Newcastle, Callaghan, Australia;</i> <sup>5</sup><i>Hunter Medical Research Insitute, New Lambton Heights, Australia;</i> <sup>6</sup><i>NHMCR Center of Research Excellence for Digestive Health, Brisbane, Australia;</i> <sup>7</sup><i>NHMCR Center of Research Excellence for Digestive Health, Newcastle, Australia;</i> <sup>8</sup><i>Centre for Microbiome Research, Queensland University of Technology, Woolloongabba, Australia</i></p><p><b><i>Background and Aim:</i></b> The socioeconomic burdens from gastrointestinal diseases and disorders continue to rise globally, and knowledge gaps remain that constrain efforts to improve their advanced diagnosis and treatment. Microbial involvement in these conditions is now widely recognised and includes specialised communities of mucosa-associated microbes. However, relatively little is known about this “forgotten microbiome”, particularly so for the proximal small intestine. Here, we seek to overcome this knowledge gap through a novel combination of microbe culture and metagenomics. We first characterize and differentiate the duodenal mucosa-associated microbiota (d-MAM) in subjects with disorders of gut brain interaction (DGBI). Next, we examine how the barrier function of duodenal spheroid cultures is affected on exposure to secreted products arising from these d-MAM cultures.</p><p><b><i>Methods:</i></b> Biopsies of duodenal tissue collected from 19 patients with DGBI (Rome IV classification) and 17 non-DGBI control subjects with no significant gastrointestinal symptoms and negative findings on endoscopy were used to inoculate a duodenal habitat-simulating medium. The diversity and functional attributes of the d-MAM recovered from these samples was produced by 16S RNA gene profiling and shotgun metagenomic sequencing (MGS) respectively. In parallel, the d-MAM cultures from each subject were filter sterilised to recover their “secretomes” of metabolites and other small molecules produced during growth. A select number of these secretomes were then used to challenge the barrier integrity of 9 different duodenal spheroid cultures produced using tissue from 3 non-DGBI “control” subjects and 3 subjects each with functional dyspepsia exclusively (FD), or with overlapping symptoms of the irritable bowel syndrome (FD/IBS). To that end, the duodenal spheroids were propagated as monolayers in transwells, and exposed to 1:5 dilutions of the chosen secretomes within the apical compartment. Trans-epithelial resistance (TEER) was measured at baseline, 6 and 24 hours.</p><p><b><i>Results:</i></b> Profiling of the d-MAM from these 36 subjects revealed not only differences between the DGBI and non-DGBI subjects, but the DGBI subjects could be further differentiated according to their Rome IV-based classifications. Specifically, the d-MAM of subjects diagnosed with FD exclusively could be differentiated from those with FD/IBS, and evidence of further differences was apparent in the d-MAM of subjects assigned to different subcategories within those diagnosed with IBS. The deep metagenomic sequencing also suggest species-level differences of the microbes recovered from these d-MAM communities. Based on the TEER measurements there were no clear interactions between secretome and spheroid response based on their respective DGBI classifications. However, the spheroid cultures derived from the non-DGBI subjects did show an improved recovery on secretome challenge relative to those derived from DGBI-subjects; suggesting the barrier integrity of spheroids from non-DGBI subjects is more resilient to the microbial secretomes than those from the DGBI subjects.</p><p><i><b>Conclusions:</b></i> Collectively, the findings presented here demonstrate the d-MAM not only differs between DGBI and non-DGBI subjects, but there are also microbial “biomarkers” of specific Rome IV symptom profiles, thereby offering new targets to advance the diagnosis and treatment options for DGBI. Our preliminary studies with duodenal spheroid cultures also suggests that barrier integrity can be measured and quantified in response to the d-MAM secretome preparations. As such, this approach brings “microbial genomes to life” and new ways to biologically reveal the key host–microbe interactions inherent to the underlying causes of different DGBI. By doing so, strategies to provide a more predictable and permanent relief from these debilitating conditions are more likely to be realised and expedited.</p>\",\"PeriodicalId\":15877,\"journal\":{\"name\":\"Journal of Gastroenterology and Hepatology\",\"volume\":\"39 S1\",\"pages\":\"262-265\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16703\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16703\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16703","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Simethicone suppresses the growth of microbes cultured from the human duodenal mucosa
Thomas Fairlie1,2, Ayesha Shah1,2, Yenkai Lim2, Jing-Jie Teh2, Lauren Schooth2, Mark Morrison2 and Gerald Holtmann1,2
1Princess Alexandria Hospital, Metro South Health, Woolloongabba, Australia;2University of Queensland, Brisbane, Australia
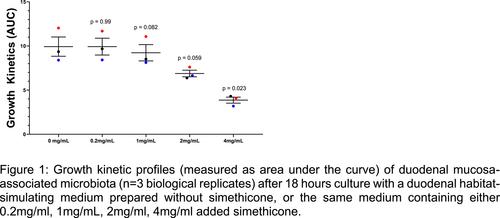
Background and Aim: Small intestinal dysbiosis (SID) is known to play an important role in the pathophysiology of various gastrointestinal and extraintestinal disorders, with recent studies linking select members of the duodenal microbiota with symptom severity in functional dyspepsia (FD). Simethicone is routinely used during endoscopy as an anti-foaming agent and at lower concentrations used to alleviate painful gut symptoms associated with excessive gas and/or bloating. Here, we assessed the effects from simethicone on the growth of a mixed culture of duodenal mucosa-associated microbiota (MAM).
Methods: The consortia of duodenal MAM recovered from the biopsies of a non-FD asymptomatic control subject were anaerobically cultured using a duodenal habitat-simulating medium with no addition, or supplemented with a commercially available source of Simethicone to provide final concentrations of 0.2 mg/ml (lowest effective dose for antifoaming effects, 1 mg/mL, 2 mg/mL or 4 mg/mL. Three biological replicates with six technical replicates of the cultures (and uninoculated controls) were prepared using a 96-well microtitre plate format within an anaerobic chamber, then microbial growth (optical density change at 600 nm) at 37 °C was measured every 30 minutes for 18 hours using an automated microtiter plate also housed within the anaerobic chamber. The R package Growthcurver was applied to assess the growth kinetic profiles by calculating the area under the curve and statistical comparisons to control cultures calculated with a paired t-test.
Results: Relative to control cultures, the growth kinetic profile (area under the curve) after 18 hours was unaffected by the addition of 0.2 mg/mL simethicone (P = 0.99), but progressively reduced by the addition of greater simethicone concentrations (Fig. 1). The reduction of growth kinetics with 2 mg/mL simethicone approached significance (P = 0.059) and were significantly reduced with 4 mg/mL simethicone (P = 0.023).
139
A whole blood interleukin-2 release assay offers a novel approach to detect and monitor pathogenic T cells to support epitope discovery and drug development in coeliac disease and beyond
Olivia Moscatelli1, Amy Russell1, Lee Henneken2, Linda Fothergill1, Hugh Reid3, Jamie Rossjohn3, Melinda Hardy1, Vanessa Bryant1 and Jason Tye-Din1
1Walter and Eliza Hall Institute, Parkville, Australia;2The Royal Melbourne Hospital, Parkville, Australia;3Monash University, Clayton, Australia
Background and Aim: Definition of the pathogenic gluten peptides in coeliac disease (CD) has afforded the opportunity to develop tools that assess the gluten-specific CD4 + T cells central to its pathogenesis. Current approaches support immune discovery (epitope mapping) and are employed in pre-clinical and clinical CD drug development as efficacy and proof-of-concept endpoints. However, current detection approaches are suboptimal: they necessitate gluten challenge to expand the T cells, which is unappealing to patients, or rely on HLA-gluten tetramers that are technically demanding. We showed interleukin (IL)-2 production is a marker of activated gluten-specific T cells and propose it offers a simpler approach. We assessed the performance of IL-2 release in an in vitro whole blood assay (WBA) before and after in vivo expansion of gluten-specific T cells by gluten-challenge and compared these readouts to the well-established functional T cell readout, IFN-γ enzyme-linked immunosorbent spot (ELISpot) assay.
Methods: Adults with HLA-DQ2.5 + treated CD (n = 10) underwent assessment before and 6 days after commencing single-bolus 10 g gluten challenge. In vitro IL-2 release was assessed after whole blood was incubated with gluten peptides (IL-2 WBA), and peripheral blood mononuclear cells were assessed using the IFN-γ ELISpot to quantify activated gluten-specific T cells. The functional effects of gluten peptides of varying immunogenicity and pan-HLA-DQ blocking were compared across these approaches.
Results: At baseline, positive responses to peptides encompassing immunodominant α-gliadin or ω-gliadin epitopes were seen in 70% (IL-2 WBA) and 10% (IFN-γ ELISpot). Six days post challenge, positive responses increased to 90% (IL-2 WBA) and 40% (IFN-γ ELISpot). IL-2 WBA responses ranked gluten peptide immunogenicity concordant with published data. Pan-HLA-DQ blocking reduced the IL-2 WBA response by mean 30-fold (Wilcoxon matched-pairs test, P = 0.002).
Conclusion: Compared to traditional measures, the IL-2 WBA shows superior sensitivity to detect the gluten-specific T cell in CD patients even when they are following a gluten-free diet. It faithfully measures in vivo systemic responses to gluten and the functional blockade of HLA, supporting its role in testing the efficacy of drugs aiming to block gluten-specific T cell responses. This approach provides a tool for Phase 1/2 clinical trials to monitor the functional status of the pathogenic T cell while avoiding the need for gluten challenge, that can be poorly tolerated and negatively impact recruitment. The IL-2 WBA has promise as a research and clinical tool in a variety of autoimmune, allergic, malignant, and infectious diseases where T cells are important.
187
Coeliac disease and the stomach: Is this an under-recognised entity? A prospective case control study
Laura Hollingsworth1,2, Anthony Brownson1 and Srikantaiah Manjunatha1
1Dunedin Hospital, Dunedin, New Zealand;2Christchurch Hospital, Christchurch, New Zealand
Background and Aim: Coeliac disease (CD) is an immune-mediated disorder triggered by the ingestion of gluten leading to small intestinal damage. Lymphocytic gastritis characterised by an increase in intraepithelial lymphocytes in the gastric mucosa has been associated with CD and a more aggressive coeliac phenotype. There is limited data regarding the prevalence of this association or sequelae and at present gastric biopsies are not standard or practice in CD across Australia or New Zealand. The aim of this study is to investigate the prevalence of gastric mucosal change including lymphocytic gastritis in patients with CD.
Methods: This prospective case control study included a total of 44 adults referred to a tertiary public hospital gastroenterology department in New Zealand. The sample size was based on a 95% confidence level. Ethics was obtained in accordance with the Health Research Council of New Zealand. Twenty-four participants were included, referred with positive coeliac serology and 20 participants were included as a control arm - referred for dyspepsia without positive serology. All participants underwent a gastroscopy in accordance with national guidelines. In those with positive coeliac serology, biopsies were taken from the first and second part of the duodenum to assess for microscopic evidence of CD. Two biopsies were also taken from the stomach to assess for concurrent changes. In those referred for dyspepsia, the duodenum was evaluated for macroscopic changes during endoscopy. Duodenal biopsies were conducted if there was suspicion of CD and gastric biopsies were taken in all participants.
Results: Of the 24 participants with positive coeliac serology, 20 had confirmed gluten sensitive enteropathy on duodenal biopsy. Histology from the gastric mucosa returned within normal limits in 16 cases. Chronic gastritis was found in 3 sampled participants and one gastric sample showed intestinal metaplasia. No gastric biopsies showed features of lymphocytic gastritis, atrophic gastritis or Helicobacter pylori. From the controls 19 gastric histology samples returned within normal limits and one showed reactive gastropathy (Table 1).
382
Colonic mucus attenuates the genotoxic effect of the Bacteroides fragilis toxin
Krista Dawson, Andrew Day and Jacqueline Keenan
University Of Otago, Christchurch, New Zealand
Background and aims: Enterotoxigenic Bacteroides fragilis (ETBF) is a pathogenic subspecies of B. fragilis that induces cleavage of E-cadherin and Interleukin (IL)-8 secretion in colonocytes. In experimental models using HT29 cells, ETBF has been shown to contribute to colorectal carcinogenesis through this mechanism. However, HT29 cells model colonocytes in isolation and fail to consider the role that secreted mucus has in protecting colonocytes in vivo. This study assessed whether mucus protects against the ETBF toxin using the mucus-secreting HT29 MTX-E12 cell line that more accurately models the colonic epithelium of a healthy individual.
Methods: HT29 MTX-E12 cells were treated with fluorescently labelled ETBF for 24 hours. The ability for ETBF to infiltrate and degrade the mucus layer was quantified by assessing the relative abundance of MUC2 in cell lysates by immunoblot analysis, coupled with immunofluorescence microscopy. E-cadherin cleavage and IL-8 secretion were assessed in both HT29 and HT29 MTX-E12 cells by immunofluorescence microscopy and ELISA assay, respectively. Bacterial pellets were collected (pre-and post-culture) to quantify the levels of toxin (bft) expression following co-culture with mucus and non-mucus producing cells by RT-qPCR. For all experiments, a one-way ANOVA or unpaired t-test was used to assess differences between treated and untreated cells.
Results: ETBF is capable of degrading colonic mucin. This was confirmed by the presence of bacteria within the mucus layer and a reduction in MUC2 expression in treated cells (P < 0.01). Despite this, no loss of E-cadherin or toxin-associated increase in IL-8 was observed in HT29 MTX-E12 cells treated with ETBF when compared to untreated controls. Moreover, the expression of the bft2 gene was downregulated (P < 0.0001) after co-culture with the mucus-secreting HT29 MTX-E12 cell line. In contrast, E-cadherin was reduced (P < 0.05) and IL-8 release was increased (P < 0.05) in HT29 cells treated with ETBF when compared with untreated controls, while bft2 expression levels remained comparable to the zero-hour control following co-culture with the non-mucus producing HT29 cell line (P > 0.05).
Conclusions: The colonic mucus barrier plays an essential role in maintaining gut homeostasis and is an important aspect to consider when modelling host-pathogen interactions in vitro. The results of this study indicate that the colonic mucus layer protects against the pathogenic effects of ETBF by regulating the expression of the bft toxin. Although B. fragilis exhibits the capacity to degrade colonic mucin, this alone was not sufficient to negate the protective attributes of the mucus barrier within this experimental timeframe.
395
Establishing intestinal organoid-microbe co-culture model to study host–microbe interactions
Ghanyah Al-Qadami1, Ilka Priebe1, Maryam Hor1, Rajvinder Singh2, Anna Wawer2 and Kim Fung3
1CSIRO, Adelaide, Australia;2Lyell McEwin Hospital, Adelaide, Australia;3CSIRO, Sydney, Australia
Background and Aim: The gastrointestinal tract is home to trillions of microorganisms that play a key role in human health and disease. The recent advancement in microbial detection technologies and next-generation sequencing tools has allowed us to identify and characterise most of these microbes. However, due to the complexity of the intestinal microenvironment, the exact mechanisms by which these microbes influence intestinal health and disease are yet to be explored. Intestinal organoids, 3D mini-intestines that recapitulate both the architecture and the cellular diversity of the intestinal epithelium, have emerged as a powerful tool for studying host-microbiome interactions in a reductionist yet biologically relevant model. As such, this project aims to develop an intestinal organoid-microbe co-culture model to investigate the interaction between microbes and epithelial cells in the organoids.
Methods: 3D human intestinal organoids were generated from adult intestinal stem cells isolated from intestinal tissue biopsies. Apical-out organoids – 3D organoids with reversed epithelial polarity so the apical surface is facing outward – and organoid-derived monolayer (ODM) were also established. The oral microbe Fusobacterium nucleatum was used as a model microorganism to develop the co-culture model. F. nucleatum was co-cultured with the organoids and its viability in the co-culture system was assessed.
Results: Ex vivo intestinal organoids, apical-out organoids, and ODM were successfully generated from intestinal tissue biopsy samples. A co-culture model was developed using three approaches i) microinjection of F. nucleatum into the organoid lumen, ii) F. nucleatum incubation with apical-out organoids, and iii) F. nucleatum incubation with ODM. Bacterial viability analysis confirmed that F. nucleatum retains its viability when incubated with organoids.
Conclusion: Organoid co-culture with F. nucleatum was successfully established. In future work, we aim to investigate how F. nucleatum influences the intestinal epithelium by measuring DNA damage, intestinal barrier integrity, inflammatory responses, and changes in gene expression.
542
The duodenal mucosa-associated microbiota differs in patients based on their Rome IV classification, and has variable effects on duodenal spheroid barrier function subjects
Lauren Schooth1,6, Grace Burns4,5,7, Kyra Minahan4,5,7, Jing-Jie Teh8, Tom Fairlie2,3, Ayesha Shah2,3,6, Gerald Holtmann2,3,6 and Mark Morrison1,2,6
1The University of Queensland, Woollongabba, Australia;2Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Woollongabba, Australia;3Faculty of Medicine, The University of Queensland, Brisbane, Australia;4Faculty of Health and Medicine, University of Newcastle, Callaghan, Australia;5Hunter Medical Research Insitute, New Lambton Heights, Australia;6NHMCR Center of Research Excellence for Digestive Health, Brisbane, Australia;7NHMCR Center of Research Excellence for Digestive Health, Newcastle, Australia;8Centre for Microbiome Research, Queensland University of Technology, Woolloongabba, Australia
Background and Aim: The socioeconomic burdens from gastrointestinal diseases and disorders continue to rise globally, and knowledge gaps remain that constrain efforts to improve their advanced diagnosis and treatment. Microbial involvement in these conditions is now widely recognised and includes specialised communities of mucosa-associated microbes. However, relatively little is known about this “forgotten microbiome”, particularly so for the proximal small intestine. Here, we seek to overcome this knowledge gap through a novel combination of microbe culture and metagenomics. We first characterize and differentiate the duodenal mucosa-associated microbiota (d-MAM) in subjects with disorders of gut brain interaction (DGBI). Next, we examine how the barrier function of duodenal spheroid cultures is affected on exposure to secreted products arising from these d-MAM cultures.
Methods: Biopsies of duodenal tissue collected from 19 patients with DGBI (Rome IV classification) and 17 non-DGBI control subjects with no significant gastrointestinal symptoms and negative findings on endoscopy were used to inoculate a duodenal habitat-simulating medium. The diversity and functional attributes of the d-MAM recovered from these samples was produced by 16S RNA gene profiling and shotgun metagenomic sequencing (MGS) respectively. In parallel, the d-MAM cultures from each subject were filter sterilised to recover their “secretomes” of metabolites and other small molecules produced during growth. A select number of these secretomes were then used to challenge the barrier integrity of 9 different duodenal spheroid cultures produced using tissue from 3 non-DGBI “control” subjects and 3 subjects each with functional dyspepsia exclusively (FD), or with overlapping symptoms of the irritable bowel syndrome (FD/IBS). To that end, the duodenal spheroids were propagated as monolayers in transwells, and exposed to 1:5 dilutions of the chosen secretomes within the apical compartment. Trans-epithelial resistance (TEER) was measured at baseline, 6 and 24 hours.
Results: Profiling of the d-MAM from these 36 subjects revealed not only differences between the DGBI and non-DGBI subjects, but the DGBI subjects could be further differentiated according to their Rome IV-based classifications. Specifically, the d-MAM of subjects diagnosed with FD exclusively could be differentiated from those with FD/IBS, and evidence of further differences was apparent in the d-MAM of subjects assigned to different subcategories within those diagnosed with IBS. The deep metagenomic sequencing also suggest species-level differences of the microbes recovered from these d-MAM communities. Based on the TEER measurements there were no clear interactions between secretome and spheroid response based on their respective DGBI classifications. However, the spheroid cultures derived from the non-DGBI subjects did show an improved recovery on secretome challenge relative to those derived from DGBI-subjects; suggesting the barrier integrity of spheroids from non-DGBI subjects is more resilient to the microbial secretomes than those from the DGBI subjects.
Conclusions: Collectively, the findings presented here demonstrate the d-MAM not only differs between DGBI and non-DGBI subjects, but there are also microbial “biomarkers” of specific Rome IV symptom profiles, thereby offering new targets to advance the diagnosis and treatment options for DGBI. Our preliminary studies with duodenal spheroid cultures also suggests that barrier integrity can be measured and quantified in response to the d-MAM secretome preparations. As such, this approach brings “microbial genomes to life” and new ways to biologically reveal the key host–microbe interactions inherent to the underlying causes of different DGBI. By doing so, strategies to provide a more predictable and permanent relief from these debilitating conditions are more likely to be realised and expedited.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
