{"title":"儿科","authors":"","doi":"10.1111/jgh.16707","DOIUrl":null,"url":null,"abstract":"<p><b>6</b></p><p><b>Comparing real-world utilisation of dietary and medical therapies in paediatric and adult inflammatory bowel disease patients using CCCare: A cross-sectional study</b></p><p><b>Joseph Pipicella</b><sup>1,2,3</sup>, Wai Kin Su<sup>1,3,4</sup>, William Wilson<sup>5,6</sup>, Jane Andrews<sup>1,7,8</sup> and Susan J Connor<sup>1,2,3,4</sup></p><p><sup>1</sup><i>Crohn's Colitis Cure, Sydney, Australia;</i> <sup>2</sup><i>South West Sydney Clinical Campus, University of New South Wales, Sydney, Australia;</i> <sup>3</sup><i>Ingham Institute for Applied Medical Research, Sydney, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia;</i> <sup>5</sup><i>SA Health, Adelaide, Australia;</i> <sup>6</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>7</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>8</sup><i>Faculty of Health Sciences, School of Medicine, University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Approximately 10% of people with inflammatory bowel diseases (IBD) are diagnosed in childhood. Crohn’s Colitis Care (CCCare) is an IBD-specific electronic medical record (EMR) used across Australia and New Zealand, with a recent upgrade to incorporate paediatric functionality. Using CCCare, we explored the real-world use of dietary and medical therapies across the age spectrum in people with IBD under routine ambulatory care in ANZ.</p><p><b><i>Methods:</i></b> De-identified data from CCCare’s linked clinical quality registry were analysed in April 2024. All people with IBD under active care (clinical encounter within the prior 14 months) were included. Children were defined as being <18 years of age at time of extraction.</p><p><b><i>Results:</i></b> A total of 6,396 people with IBD were included. In the <18 years age group (n=172), 59.1% (n=101) were male with a median age of 15 years (IQR 12.8-16). The majority (93%, n=93) resided in Australia, and most had Crohn’s disease (66.5%, n=113), with 16.8% of them having ever had a perianal fistula. In the ≥18 years age group (n=6,224), 49.1% (n=3,055) were male with a median age of 42 years (IQR 32-57). The majority (76.5%, n=4,761) resided in Australia, and over half had Crohn’s disease (55.7%, n=113), with 15.9% having ever had a perianal fistula.Interestingly, 5-aminosalicylate use was more prevalent in adults than children (34% vs 27% respectively, P<0.05), whereas current immunomodulator use was less common in adults compared to children (29% vs 60% respectively, P<0.001). Current steroid use was ≤4% in both cohorts (P=0.26). Advanced therapy use by age group is shown below. Anti-TNF therapies (infliximab and adalimumab) were the predominant therapies in the paediatric cohort. Across the cohort, infliximab use decreased with age, whereas vedolizumab use increased with age. Dietary therapies were infrequently used/documented, with only 5/172 (2.9%) receiving dietary therapy in the paediatric cohort (Exclusive Enteral Nutrition [EEN]=4, Crohn's Disease Exclusion Diet [CDED]=1) and 49/6224 (0.8%) in the adult cohort (EEN=36, CDED=13) (p<0.001).</p><p><b>12</b></p><p><b>Meta-analysis of the pooled positive predictive value of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) no-biopsy approach for coeliac disease testing in children</b></p><p>Angharad Vernon-Roberts<sup>3</sup>, Sanjeev Verma<sup>4</sup>, Andrew Day<sup>3</sup> and <b>Shaun Ho</b><sup>1,2</sup></p><p><sup>1</sup><i>Royal Children's Hospital Melbourne, Parkville, Australia;</i> <sup>2</sup><i>Murdoch Children Research Institute, Parkville, Australia;</i> <sup>3</sup><i>University of Otago Christchurch, Christchurch, New Zealand;</i> <sup>4</sup><i>King George Medical University, Lucknow, India</i></p><p><b><i>Background and Aim:</i></b> The 2012 and 2020 ESPGHAN guidelines for the diagnosis of coeliac disease (CD) in children included a non-biopsy approach for children meeting specific criteria; ≥10 times the upper limit of normal anti-tissue transglutaminase IgA antibody, positive endomysial IgA antibody, +/- positive coeliac HLA haplotypes (HLA). The aim of the study was to perform a meta-analysis of the overall CD diagnostic accuracy using the ESPGHAN non-biopsy criteria in children who also had small bowel biopsy (SBB) confirmation as the reference standard.</p><p><b><i>Methods:</i></b> Database searches (Medline, Embase, Web of Science, Scopus) were done in October 2023 and studies underwent stages of exclusion if they did not adhere to the ESPGHAN criteria and have SBB confirmation. A random effects meta-analysis provided a pooled positive predictive value (PPV) for all studies, sub-group analysis was carried out to identify sources of heterogeneity.</p><p><b><i>Results:</i></b> Searches identified 1053 articles, with 21 included in the final analysis. While study sample sizes ranged from 39 to 707 with a total of 4087, 2323 children fulfilled the ESPGHAN non-biopsy criteria and of these 2289 had comparative SBB and were included in the final meta-analysis. The proportion of CD cases diagnosed using the ESPGHAN non-biopsy approach compared to SBB ranged from 79.2-100% in studies, with an overall pooled PPV of 97.3% (CI 95.4,98.6) [Figure 1]. Between study heterogeneity was high (I2 79.2%, p<0.0001, CI 68.8,86.1), explored using sub-group analysis that showed higher PPV for studies using prospective methodologies (p=0.001). Sensitivity analysis showed that PPV was higher in studies applying the ESPGHAN criteria that included positive HLA, versus the criteria without HLA (PPV 98.5 vs 96.7, p=0.014).</p><p><b>55</b></p><p><b>Collagenous gastritis in children: response to oral budesonide</b></p><p><b>Jay Sharma</b> and Ryan Joseph Anson and Ajay Sharma</p><p><i>University Of Western Australia, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Collagenous gastritis(CG) is a rare disease in children characterized by the subepithelial deposition of collagen bands and inflammatory infiltrates in the gastric lamina propria with no effective treatment described to date. We aim to describe the outcomes of 3 patients with a 3 months course of oral Budesonide that will contribute to improved therapeutic options for this rare condition.</p><p><b><i>Methods:</i></b> A retrospective chart review (0-18 years) in the last 10 years was reviewed (2013-2023) with a total of 3 cases of CG identified.</p><p><b><i>Results:</i></b></p><p><b>Case 1:</b> A 15-year-old female presented with significant anaemia with haemoglobin of 71 g/L (NR-125-175 g/L) with ferritin < 5 ug/L (NR 20-200 ug/L). Esophagogastroduodenoscopy revealed CG in histology. She was started on a 3-month course of Oral Budesonide 9 mg, 6 mg and 3 mg with a repeat Hb and ferritin levels remaining in the normal range.</p><p><b>Case 2:</b> A 17-year-old male was referred with anaemia despite trialling PPI and oral iron. EGD confirmed CG and on daily 3 months of Budesonide with a similar regimen as Case 1, had stable Iron levels and Hb.</p><p><b>Case 3:</b> A 15 yo presented with fatigue (Hb 57 g/dl) and failed trial of PPI and oral iron. EGD confirmed CG and a similar regimen was followed as case 1 with Ferritin and Hb staying in the normal range after 3 months.</p><p><b><i>Conclusions:</i></b> This case series demonstrates considering trialling a 3-month weaning course of Budesonide if Oral iron therapy and PPI trial fail and it could be an effective therapeutic option for the CG patients though it's unclear whether this regimen could be considered a safe long-term option. Further research is needed to understand the Pathophysiology and treatment target.</p><p><b>148</b></p><p><b>An automated approach to the analysis of paediatric high-resolution colonic manometry data: characterisation of the meal response in children with Hirschsprung disease using a Bayesian functional mixed effects model</b></p><p><b>Hannah Evans-Barns</b><sup>1,2,3</sup>, Lukasz Wiklendt<sup>6</sup>, John Hutson<sup>2,3,4</sup>, Warwick Teague<sup>1,2,3</sup>, Mark Safe<sup>5</sup>, Sebastian King<sup>1,2,3</sup> and Phil Dinning<sup>6</sup></p><p><sup>1</sup><i>Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Australia;</i> <sup>2</sup><i>Surgical Research Group, Murdoch Children's Research Institute, Melbourne, Australia;</i> <sup>3</sup><i>Department of Paediatrics, University of Melbourne, Melbourne, Australia;</i> <sup>4</sup><i>Department of Urology, The Royal Children’s Hospital, Melbourne, Australia;</i> <sup>5</sup><i>Department of Gastroenterology and Clinical Nutrition, The Royal Children’s Hospital, Melbourne, Australia;</i> <sup>6</sup><i>Gastroenterology Department, Flinders Medical Centre, Bedford Park, Australia</i></p><p><b><i>Background and Aim:</i></b> Post-operative bowel dysfunction is prevalent in children with Hirschsprung disease (HD). The aim of this study was to characterise the colonic meal response, recorded by high-resolution manometry (HRCM), using a Bayesian functional mixed effects model, and compare findings to healthy controls.</p><p><b><i>Methods:</i></b> A HRCM catheter was positioned in the colon with sensors spanning the caecum to rectum. A one hour baseline recording was followed by a meal challenge and a further one hour recording. The control group consisted of 13 healthy adults. Cross-wavelet analysis was used to compute the frequency and direction of all propagating pressure waves (PPW). A latent Gaussian Process model was used compare the effects of the meal on PPW within, and between, patients and controls. Ethical approval was obtained (HREC 64192).</p><p><b><i>Results:</i></b> A meal was eaten by 13 children (12 male; 6.83±2.56 years; 9/13 short-segment). In the proximal colon, while the meal induced a significant increase both antegrade and retrograde PPW across a range of frequencies (1/16 to 8 cycles per minute [cpm]), the effect was significantly reduced in HD (Figure). In the distal colon of controls, the meal induced a significant increase in all PPWs between 1/16 – 8 cpm. In HD, the meal did not increase PPW between 2-10cpm.</p><p><b>152</b></p><p><b>Crossed wires: aligning clinical practice with family experiences in paediatric temporary tube feeding</b></p><p><b>Claire Reilly</b><sup>1,2</sup>, Jeanne Marshall<sup>1,2</sup>, Rebecca Packer<sup>1</sup>, Jasmine Foley<sup>1</sup> and Nikhil Thapar<sup>1,2,3</sup></p><p><sup>1</sup><i>The University Of Queensland, Brisbane, Australia;</i> <sup>2</sup><i>Children's Health Queensland, Brisbane, Australia;</i> <sup>3</sup><i>Queensland University of Technology, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Temporary tube feeding is crucial for children requiring short-term nutritional support, yet its impact on families is under-researched. This study aimed to compare the perspectives of families of children with temporary feeding tubes with the clinicians who managed them, with the goal of enhancing understanding, improving clinical practice and investigating the children’s quality of life.</p><p><b><i>Methods:</i></b> This study, part of a larger mixed-methods research project at a major children’s hospital, collected data from families of children discharged home with a temporary feeding tube (e.g., nasogastric tube) using electronic diaries and semi-structured interviews. Medical records were reviewed, and quality of life was assessed using the Pediatric Quality of Life Inventory version 4.0 Generic Core Scales (PEDsQL) at key time points (tube insertion, midpoint, removal). Clinicians completed an online survey.</p><p><b><i>Results:</i></b> This study included 37 children with temporary feeding tubes, and 112 clinicians (medical practitioners, nursing, and allied health) overseeing their care. Communication gaps were prevalent: whilst 95% (n=35) of families were informed about the tube’s necessity, only 12% (n=4) recalled being told about the expected duration, despite 44% (n=49) of clinicians describing having this conversation. The medical notes revealed that only one child had a tube exit plan, despite 28 clinicians reporting completing this. Importantly, 32% (n=35) of clinicians were unable to recall whether estimated tube feeding duration was ever discussed. Additionally, whilst 61% (n=68) of clinicians provided written information about the feeding tube, 16% (n=18) were unable to recall whether or not they did. Seven children received feeding tubes despite documented parental objections in their medical notes. Preliminary quality of life results indicated a mean PEDS-QL score of 53.2 (SD±15.9) at tube insertion, 61.5 (SD±16.9) at midpoint, and 65.8 (SD±19.3) at the endpoint. These scores are lower than those reported in healthy children (83.9; SD±12.5), and lower when compared to studies of children with other health conditions.</p><p><i><b>Conclusion:</b></i> This study revealed substantial disparities in clinical decision-making and communication regarding temporary feeding tubes. These children experienced lower reported quality of life compared to their healthy peers and those with other health conditions. There is a discrepancy between the care clinicians believe they provide and what families retain. This study recommends improved guidelines for communication, education, and documentation to better align clinical practices with family needs, ensuring better outcomes for this group of children.</p><p><b>306</b></p><p><b>Proactive therapeutic drug monitoring (TDM) of infliximab leads to durability of treatment in children with inflammatory bowel disease</b></p><p><b>Cher Wei Chuah</b><sup>1</sup> and <b>Shoma Dutt</b><sup>1,2</sup></p><p><sup>1</sup><i>Department Of Gastroenterology, The Children's Hospital At Westmead, Westmead, Australia;</i> <sup>2</sup><i>CHW Clinical School University of Sydney, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Anti-tumour Necrosis Factor therapies are the only biological therapy approved on the pharmaceutical benefits scheme (PBS) for children in Australia. Loss of response to the 1<sup>st</sup> biological predicts poorer responses to subsequent biologicals<sup>1</sup>. Maintaining and preserving response is beneficial in the paediatric age group. Published literature suggest that one third of patients will develop secondary loss of response (LOR) by the first year and up to 50% of initial responders will develop LOR by 5 years.<sup>2</sup> Evidence suggest sustained high trough levels increases the durability of infliximab. The ability to recapture response in secondary LOR with dose escalation is well described.<sup>3</sup> In 2019, our unit opted for proactive TDM (at week 6, week 14 and 6 monthly thereafter) and dose escalation based on cutoffs at week 6 < 15 μg/mL, week 14/maintenance < 5 μg/mL as standard practice, in addition to the usual practice of escalation guided by the clinical picture.<sup>4</sup> We report the outcomes of our patient cohort over a period of 2 years from initiation of infliximab.</p><p><b><i>Methods:</i></b> A retrospective chart review of patients commenced on infliximab was performed between 01/01/2019 to 31/12/2021. Only patients who completed induction were included, patients with acute severe colitis were excluded from this report as they were escalated on different parameters and will be reported separately. Data on demographics, disease characteristics, immunomodifier usage, infliximab dosing and frequency, infliximab drug levels, and antibody levels and switching to alternative biologics were collected and analysed. A physician global assessment (PGA) scale of remission, mild, moderate, and severe was used to assess clinical outcomes. Standard infliximab dosing is 5mg/kg at 0, 2, 6 weeks for induction and every 8 weeks during maintenance phase. Escalation was defined as either shortening of standard interval and/or increased dose to 10mg/kg.</p><p><b><i>Results:</i></b> 98 patients (58% male) were identified, 82% had Crohn’s disease (CD) and 18% Ulcerative Colitis (UC). Median age at diagnosis was 11 years old, and 12.5 years old at starting infliximab. 81% received an immune modifier of which 64% had methotrexate and 39% azathioprine. 13% received escalated induction and 77% escalated maintenance. 3% failed to achieve remission and were discontinued. 2% developed infliximab antibodies. 8% of patients were switched to an alternate biologic by 1 year and 18% by 2 years, median time to switch was 53 weeks. Of those that remained on infliximab, 83% were in clinical remission at 1 year and 94% at 2 years. Switching to alternate biologic was associated with escalated induction, OR 5.8 (1.5 – 22.5, p = 0.01) UC, OR 5.6 (1.8 – 17.5, p < 0.01) and concomitant steroid use, OR 4.1 (1.1-15.5, p = 0.04). Immunomodulator use was not associated with switching biologics (p = 0.84). No patients on escalated induction developed antibodies (p = 0.58) and 1 patient on escalated maintenance developed antibodies (p = 0.48). There was no significance difference with standard or escalated maintenance with the PGA at the 1-year (p = 0.14) and 2 –year mark (p = 0.49).</p><p><b><i>Conclusion:</i></b> Proactive TDM and escalation of infliximab results in good durability with treatment persistence at 92% at 1 year and 82% at 2 year and an excellent clinical remission rate of 94% at 2 years. Escalated induction and UC were predictors to switch biologics which is in keeping with primary non-responders/severe phenotype. Vahabnezhad et al reports in their series of paediatric CD also treated with escalated infliximab had treatment persistence of 80% at 2 years.<sup>3</sup> Our CD cohort had 88% who remain on infliximab at 2 years. This study provides real world evidence that the subset of patients that responds well to infliximab can be maintained on this therapy longer than what is in the current published literature and merit that escalated therapy is funded by the PBS.</p><p><b>References</b></p><p>\n 1. <span>Gisbert, J. P.</span>, & <span>Chaparro, M.</span> (<span>2020</span>). <span>Predictors of Primary Response to Biologic Treatment [Anti-TNF, Vedolizumab, and Ustekinumab] in Patients With Inflammatory Bowel Disease: From Basic Science to Clinical Practice</span>. <i>Journal of Crohn's & colitis</i>, <span>14</span>(<span>5</span>), <span>694</span>–<span>709</span>. https://doi.org/10.1093/ecco-jcc/jjz195</p><p>\n 2. <span>Ding, N. S.</span>, <span>Hart, A.</span>, & <span>De Cruz, P.</span> (<span>2016</span>). <span>Systematic review: predicting and optimising response to anti-TNF therapy in Crohn's disease - algorithm for practical management</span>. <i>Alimentary pharmacology & therapeutics</i>, <span>43</span>(<span>1</span>), <span>30</span>–<span>51</span>. https://doi.org/10.1111/apt.13445</p><p>\n 3. <span>Vahabnezhad, E.</span>, <span>Rabizadeh, S.</span>, & <span>Dubinsky, M. C.</span> (<span>2014</span>). <span>A 10-year, single tertiary care center experience on the durability of infliximab in pediatric inflammatory bowel disease</span>. <i>Inflammatory bowel diseases</i>, <span>20</span>(<span>4</span>), <span>606</span>–<span>613</span>. https://doi.org/10.1097/MIB.0000000000000003</p><p>\n 4. <span>Rheenen, P. F.</span>, <span>Aloi, M.</span>, <span>Assa, A.</span>, et al. (<span>2020</span>). <span>The Medical Management of Paediatric Crohn's Disease: an ECCO-ESPGHAN Guideline Update</span>. <i>Journal of Crohn's & colitis</i>, jjaa161. Advance online publication. https://doi.org/10.1093/ecco-jcc/jjaa161</p><p><b>350</b></p><p><b>Changes in paediatric inflammatory bowel disease care at a paediatric tertiary hospital from 2014 to 2021</b></p><p><b>Jessica Nguyen</b><sup>1</sup>, Joan Cheng<sup>2</sup> and Edward Giles<sup>3,4</sup></p><p><sup>1</sup><i>Department of Paediatric Gastroenterology, Monash Children's Hospital, Monash Health, Clayton, Australia;</i> <sup>2</sup><i>Faculty of Medicine, Nursing and Health Sciences, Monash University, Clayton, Australia;</i> <sup>3</sup><i>Department of Paediatrics, Monash University, Clayton, Australia;</i> <sup>4</sup><i>Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Clayton, Australia</i></p><p><b><i>Background and Aim:</i></b> The recent Paediatric Inflammatory Bowel Disease (PIBD) quality of care project investigated the care of children with IBD in Australia in 2021. This included a national audit of patient care that was almost directly comparable to the IBD audit from 2014. This provided an opportunity for all hospitals that were involved in both audits to examine how their care had changed.</p><p><b><i>Methods:</i></b> Organisational data (including total admissions, staffing etc) from our paediatric tertiary hospital from 2014 to 2021 were compared. In addition, inpatient admissions data was audited from patients with ulcerative colitis (UC) and Crohn’s disease admitted. Statistical analysis was performed using Chi-Square test (Prism software).</p><p><b><i>Results:</i></b> From 2014 to 2021, we had similar number of Crohn’s disease admissions (15 in 2014, 14 in 2021); however, double the number of UC admissions (12 in 2014, 24 in 2021, See figure 1) The most common length of stay was between 3-6 days for both Crohn’s and UC. In 2021, a smaller percentage of Crohn’s patients had a previous admission (78% in 2014 down to 43%, p<0.0001). In UC patients, a higher percentage of patients had a previous admission (25% up to 48%, p=0.0007). In 2021, there were more patients with anaemia (64% in 2021 compared to 33% in 2014 in Crohn’s disease, p<0.0001; 60% in 2021 compared to 25% in 2014 in UC, p<0.0001) and malnutrition on admission (6 compared to 2 with Crohn’s disease, p=0.0015; 4 compared to 1 with UC, p=0.1649).</p><p><b>362</b></p><p><b>A population-based study of the prevalence and metabolic significance of steatotic liver disease in children and their parents</b></p><p><b>Oyekoya Ayonrinde</b><sup>1,2,3</sup>, Shailender Mehta<sup>1</sup>, Stephanie Dowden<sup>4</sup>, Timothy Fairchild<sup>5</sup>, Gina Ambrosini<sup>6</sup>, Desiree Silva<sup>2,7</sup>, Kemi Wright<sup>8</sup>, Sheeraz Mohd<sup>1</sup>, Leela King<sup>1</sup>, Seyifunmi Afolabi<sup>9</sup> and Janine Spencer<sup>1</sup></p><p><sup>1</sup><i>Fiona Stanley Hospital, Murdoch, Australia;</i> <sup>2</sup><i>The University of Western Australia, Perth, Australia;</i> <sup>3</sup><i>Curtin University, Bentley, Australia;</i> <sup>4</sup><i>NursePrac Australia, Success, Australia;</i> <sup>5</sup><i>Murdoch University, Murdoch, Australia;</i> <sup>6</sup><i>Healthway, Perth, Australia;</i> <sup>7</sup><i>Joondalup Hospital, Joondalup, Australia;</i> <sup>8</sup><i>University of New South Wales, Sydney, Australia;</i> <sup>9</sup><i>Oceania University of Medicine, Brisbane, Australia</i></p><p><b><i>Background and Aims:</i></b> Steatotic liver disease (SLD) is the most common chronic liver disorder globally. SLD in childhood reflects prevalent metabolic dysfunction in children and families and poses increased longer-term risk of early-onset cardiometabolic and liver-related complications. We examined the prevalence and metabolic significance of SLD in children and their parents.</p><p><b><i>Method:</i></b> Population-based children, aged 5-15 years, and their parents participated in a cross-sectional observational study of SLD in Perth, Australia. Assessments included anthropometry (weight, height, waist circumference and skinfold thickness [SFT]) and blood tests. Utilising Fibroscan® we non-invasively examined the severity of hepatic steatosis using controlled attenuation parameter (CAP), and severity of liver fibrosis using transient elastography (TE)-measured liver stiffness measurement (LSM). SLD was defined by CAP ≥249 dB/m in children and ≥275 in parents. Children aged 5-10 years were considered as young children and those aged 11-15 years as older children. SLD in children was considered to be metabolic dysfunction-associated SLD (MASLD). We compared cardiometabolic characteristics of children with versus those without MASLD, and sought associations between MASLD in children and parent characteristics.</p><p><b><i>Results:</i></b> One hundred and fifteen children (50% male), with mean [SD] age 9.6[2.7] years, 74 mothers aged 40.7[5.8] years and 24 fathers aged 44.2[5.8] participated in the study. One child did not have FibroScan® assessment. Seventy-three children (64%) were young children. Compared with older children, young children had lower body weight, height and waist circumference (p<0.05), but skinfold thickness, CAP, LSM, serum lipids, leptin, high sensitivity C-reactive protein (hsCRP) and liver enzyme levels were not significantly different (p>0.05 for all). Comparing boys vs. girls, there were no significant differences in anthropometric measures of adiposity or CAP overall (p>0.05 for all). Mean (SD) WC was 88.3(13.4) cm in mothers and 91.8 (10.9) cm in fathers. Mean BMI was 27.7 (5.3) kg/m<sup>2</sup> in mothers and 27.3 (3.0) kg/m<sup>2</sup> in fathers. SLD was diagnosed in 20.2% children (15.8% male vs. 24.6% female, p=0.24), 29.9% mothers and 37.5% fathers. SLD was seen in 55% of children with BMI ≥30 kg/m<sup>2</sup>. Children with MASLD had greater subcutaneous fat measured as SFT, serum alanine aminotransferase (ALT), leptin, hsCRP, and triglycerides, and lower levels of high-density lipoprotein cholesterol, compared with those without SLD (p<0.05 for all, Table 1). CAP in children was positively correlated with BMI z-score, waist circumference, skinfold thickness, weight, ALT, gamma glutamyl transpeptidase (GGT), triglycerides, leptin, and maternal and paternal BMI (p<0.05 for all). There was no significant correlation between SLD in children and their parents, however mothers of children with SLD had higher mean BMI than mothers of children without SLD (30.3[5.7] kg/m<sup>2</sup> vs. 27.1[5.1] kg/m<sup>2</sup>, p=0.04), and fathers had higher mean liver stiffness measurement (LSM), (7.6[4.6] kPa vs. 4.8[1.2] kPa, p=0.02. Using multivariable logistic regression analysis, child ALT (OR 1.21, 95% CI 1.01-1.45) and abdominal SFT (OR 1.59, 95% CI 1.03-2.44) were associated with SLD in children, after adjusting for child WC (OR 0.94, 95% CI 0.87-1.04), and maternal BMI (OR 1.22, 95% CI 0.85-1.76).</p><p><b><i>Conclusion:</i></b> MASLD is common in children, and is associated with increased adiposity, raised ALT, features of metabolic dysfunction, maternal adiposity, and paternal liver stiffness. Our findings suggest intergenerational heritability of metabolic and hepatic risk.</p><p><b>471</b></p><p><b>Similar outcomes following early proactive vs reactive therapeutic drug monitoring in children with Crohn’s disease commencing infliximab – a single centre, retrospective study</b></p><p><b>Asha Jois</b><sup>1</sup>, Rachel Horn<sup>1</sup>, Anysha Walia<sup>1</sup>, Eric Cheah<sup>2</sup>, Robert Little<sup>3</sup> and George Alex<sup>1,4</sup></p><p><sup>1</sup><i>Royal Children's Hospital, Parkville, Australia;</i> <sup>2</sup><i>Monash Children's Hospital, Clayton, Australia;</i> <sup>3</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>4</sup><i>University of Melbourne, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Benefits of a proactive compared to a reactive therapeutic drug monitoring (TDM) strategy when commencing infliximab (IFX) for management of Crohn’s disease are unclear. We evaluated the 6- and 12-month outcomes in children commencing IFX with proactive week 14 TDM compared to those without week 14 TDM.</p><p><b><i>Methods:</i></b> Single-centre, retrospective study of Crohn’s disease patients aged 0-18 years with a primary response to IFX induction between 2018-2021. Proactive TDM was defined by measurement of a week 14 IFX drug level and reactive TDM was defined by no week 14 drug level. Baseline patient, medication and disease characteristics were compared across the two groups. Clinical and biochemical disease activity measures, and IFX dose, frequency and drug level were compared across the two groups at week 0, 6- and 12-months post-induction. Failure was defined by biologic switch, corticosteroid use, hospitalisation or surgery.</p><p><b><i>Results:</i></b> We included 86 patients. 34/86 (40%) were female, diagnosed at median 13 years, with a median disease duration of 4 years. 40/86 (47%) had proactive TDM – baseline characteristics by group are presented in Table 1. At 12-months, there was no difference in failure rates (15% vs. 23%, p = 0.419) or IFX persistence (95% vs. 89%, p = 0.442) between the proactive and reactive TDM groups, respectively. At 6-months, the proactive group had more escalated IFX dose frequency (23% vs. 5%, p = 0.023), but IFX dose was comparable (5.8 vs. 5.5 mg/kg, p = 0.108). There was no difference in IFX drug level or disease severity at either 6- or 12-months.</p><p><i><b>Conclusion:</b></i> In children with Crohn’s disease commenced on IFX, week 14 proactive TDM was not associated with improved outcomes at 12-months compared to children without week 14 TDM, and IFX drug levels were comparable. Prospective studies are required to identify the optimal TDM strategy.</p><p><b>480</b></p><p><b>Subcutaneous infliximab use in children with inflammatory bowel disease in a tertiary paediatric hospital</b></p><p><b>Jessica A Eldredge</b><sup>1</sup>, Cher Wei Chuah<sup>1</sup>, Michelle Tano<sup>1</sup>, Trudy Chidgey, Noel Singh<sup>1,2</sup>, Kunal Thacker<sup>1</sup>, Annabel Magoffin<sup>1</sup> and Shoma Dutt<sup>1</sup> and Edward O'Loughlin<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Children's Hospital at Westmead, Australia;</i> <sup>2</sup><i>Pharmacy Department, Children's Hospital at Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Anti-Tumour Necrosis Factor (anti-TNF) therapies remain the only biological treatment accessible for use in Australian children with moderate to severe inflammatory bowel disease (IBD) via the Pharmaceutical Benefits Scheme. SC infliximab is now well-established in adult IBD care (1-3). Compared to traditional IV formulations, SC dosage may offer relative pharmacokinetic stability with sustained drug delivery, with comparable efficacy, safety and immunogenicity profiles (1-3). Published literature demonstrates that in younger IBD patients, the majority would prefer to switch to subcutaneous (SC) versions of their current intravenous (IV) biologic (1,2). Scarce real-world data is available on use of SC infliximab in paediatric IBD, with only seven children described from a single-centre cohort study in Edinburgh (4). We aimed to assess the clinical efficacy, tolerability and cost-benefit of SC infliximab, as part of an initiative supported by our local institutional Medicines and Therapeutics Committee.</p><p><b><i>Methods:</i></b> We report twelve children with IBD who commenced 120mg fortnightly SC infliximab dosing between February to May 2024. Baseline, 4, 8 and 12 week follow-up biochemical and clinical assessments were undertaken over this treatment period. Nine of twelve children were male, with median age 14.5 years [range 6-17 years]. Eleven had a diagnosis of Crohn’s disease. Two children received SC infliximab as the third dose in their induction therapy and ongoing. Ten children were transitioned from stable infliximab IV maintenance dosing. All were prescribed concomitant immunomodulator therapy (azathioprine or methotrexate).</p><p><b><i>Results:</i></b> Clinical and biochemical parameters for children treated with subcutaneous infliximab are outlined in Table 1. Clinical disease activity indices (Paediatric Crohn’s Disease Activity Index [PCDAI] or Paediatric Ulcerative Colitis Activity Index [PUCAI]) were stable or improved over the treatment period. Median baseline infliximab level prior to first SC dose was 9.2 mg/L [IQR 7.1 – 11.0] with calprotectin 53.5ug/g [IQR 20-334]. Infliximab level increased by a median of 9.3mg/L [IQR 0.7-12.3], and calprotectin reduced by median 32ug/g [IQR -92.5-35.5] over the 12 week follow-up period. No significant adverse events were observed. Combined cost of escalated non-PBS infliximab intravenous dosing, day medical unit admission and consumables saved was estimated at $12,304.92 per patient per annum in this group.</p><p><b><i>Conclusion:</i></b> Calprotectin and clinical disease activity indices were stable or on average improved following twelve weeks of SC infliximab dosing in twelve children with IBD. We propose subcutaneous infliximab may be an efficacious and cost-saving treatment alternative to IV dosing in children with IBD, reducing healthcare costs (admissions for IV infusions), and financial and educational impacts on patients and families (lost work and school days). Further data in larger cohorts of children is required, including quality-of-life and cost-saving assessment scales.</p><p><b>References</b></p><p>\n 1. <span>Buisson, A</span>, <span>Nachury, M</span>, <span>Reymond, M</span> et al. <span>Effectiveness of Switching From Intravenous to Subcutaneous Infliximab in Patients With Inflammatory Bowel Diseases: the REMSWITCH Study</span>. <i>Clin Gastroenterol Hepatol</i> <span>2023</span>; <span>21</span>: <span>2338</span>-<span>46.e3</span>.</p><p>\n 2. <span>Schreiber, S</span>, <span>Ben-Horin, S</span>, <span>Leszczyszyn, J</span> et al. <span>Randomized Controlled Trial: Subcutaneous vs Intravenous Infliximab CT-P13 Maintenance in Inflammatory Bowel Disease</span>. <i>Gastroenterology</i> <span>2021</span>; <span>160</span>: <span>2340</span>-<span>53</span>.</p><p>\n 3. <span>Strik, AS</span>, <span>Vrie, W</span>, <span>Bloemsaat-Minekus, JPJ</span> et al. <span>Serum concentrations after switching from originator infliximab to the biosimilar CT-P13 in patients with quiescent inflammatory bowel disease (SECURE): an open-label, multicentre, phase 4 non-inferiority trial</span>. <i>Lancet Gastroenterol Hepatol</i> <span>2018</span>; <span>3</span>: <span>404</span>-<span>12</span>.</p><p>\n 4. <span>Gianolio, L</span>, <span>Armstrong, K</span>, <span>Swann, E</span> et al. <span>Effectiveness of Switching to Subcutaneous Infliximab in Pediatric Inflammatory Bowel Disease Patients on Intravenous Maintenance Therapy</span>. <i>J Pediatr Gastroenterol Nutr.</i> <span>2023</span>; <span>77</span>(<span>2</span>): <span>235</span>-<span>239</span>. https://doi.org/10.1097/MPG.0000000000003838.</p><p><b>481</b></p><p><b>An Australian paediatric experience using orodispersible budesonide in eosinophilic oesophagitis</b></p><p><b>Juliet Affum</b><sup>1</sup>, Geoff Withers<sup>1</sup>, Alberto Pinzon-Charry<sup>2,3,4</sup> and Looi Ee<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Hepatology & Liver Transplant, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Queensland Paediatric Immunology & Allergy Service, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>The University of Queensland, Brisbane, Australia;</i> <sup>4</sup><i>Griffith University, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is an atopic and debilitating condition which has emerged in the last three decades with limited treatment options. Targeted therapies were not available in Australia until recently. On 1<sup>st</sup> May 2022, Jorveza®, a budesonide orodispersible tablet was listed on the Pharmaceutical Benefits Scheme (PBS) specifically for treating EoE. Our aim was to review the paediatric experience in our centre with this therapy.</p><p><b><i>Methods:</i></b> Retrospective review of patients in a tertiary paediatric hospital who commenced this therapy between 1<sup>st</sup> May 2022 and 7<sup>th</sup> August 2023 was undertaken. Patient demographics, endoscopic appearance and histologic findings were recorded. Histologic remission was defined using two thresholds, <5 eos/hpf (PBS criteria) and ≤15 eos/hpf (standard criteria).</p><p><b><i>Results:</i></b> Sixty-three patients, 87% (55/63) male, median age 14 (range 8-17) years were treated during this period. Thirty-five (56%) had a gastroscopy within 3 months of starting Jorveza® while the rest were “grandfathered” as they were already on swallowed topical steroids. Only 10 patients were newly diagnosed and thus, treatment naïve. Eighty-seven percent (55/63) had repeat gastroscopy at median 3.7 (range 2.1-13.7) months after staring Jorveza®. Remission was achieved in 49.09% (≤15 eos/hpf, standard criteria) and 41.82% (<5 eos/hpf, PBS criteria) respectively. Female gender and medication adherence were significantly associated with remission. Post treatment oesophageal eosinophil count was lower in compliant patients compared to those with suboptimal medication adherence, mean 21 vs 79 eos/hpf, p=0.006. There was a trend to higher oesophageal eosinophil counts with longer duration between Jorveza® commencement and repeat endoscopy in both responders and non-responders, but this did not reach statistical significance.\n\n </p><p><i><b>Conclusion:</b></i> Jorveza® is an effective treatment for inducing histologic remission in children with EoE but is affected by compliance. Gender and medication adherence are significantly associated with histologic remission.</p><p><b>493</b></p><p><b>Percutaneous liver biopsy in children: comparison of complication rates between coaxial and noncoaxial techniques</b></p><p><b>Sudarshan Arvind</b><sup>1</sup> and <b>Murthy Chennapragada</b><sup>1,2</sup></p><p><sup>1</sup><i>The University of Sydney, Camperdown, Australia;</i> <sup>2</sup><i>The Children's Hospital Westmead, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Ultrasound guided percutaneous liver biopsy (PLB) is crucial in diagnosis and monitoring of paediatric liver disease. Two major techniques are used; coaxial (C-PLB) and non-coaxial (NC-PLB). C-PLB uses an outer needle sheath that penetrates the liver capsule, enabling a smaller biopsy needle to pass into the liver parenchyma. NC-PLB does not use an outer sheath, requiring more transgressions of the liver capsule to obtain the same number of cores of liver tissue. There is limited literature directly comparing complication rates following these techniques in children. The aim of this paper is to compare the incidence of complications following ultrasound-guided C-PLB and NC-PLB in children.</p><p><b><i>Methods:</i></b> This is a single-centre retrospective cohort study conducted at The Children’s Hospital Westmead (New South Wales). We studied paediatric patients who underwent ultrasound-guided PLB between September 2016 and December 2019. Patients were divided into C-PLB (n= 227) and NC-PLB (n= 47). Electronic medical records were used to gather demographic data, baseline characteristics, clinical indication and post-procedural complications (stratified into major or minor according to the Society of Interventional Radiology classification system). Chi-square analysis was used to compare demographic and baseline characteristics and to determine if there was a significant difference in the incidence of complications between these groups.</p><p><b><i>Results:</i></b> A total of 274 paediatric patients underwent ultrasound-guided PLB between September 2016 and December 2019. 227 underwent C-PLB (83%) while 47 underwent NC-PLB (17%). 51.5% of all PLB recipients were female. Biliary atresia (34.7%) was the most common primary diagnosis, followed by autoimmune hepatitis (8.4%). Coagulopathy or thrombocytopaenia (6.2%) was the most common pre-biopsy comorbidity. There were no major complications encountered across either cohort. Total incidence of minor complications was 17.9%. Minor complications occurred in 16.7% of the C-PLB cohort compared to 23.4% in the NC-PLB cohort. The difference was not significant (p=0.278). There was a significantly lower incidence of asymptomatic bleeding (p=0.002) in the C-PLB cohort compared to the NC-PLB cohort.</p><p><b><i>Conclusion:</i></b> Our findings do not suggest a significant difference in the incidence of complications following ultrasound-guided C-PLB vs. NC-PLB, with the exception of bleeding which occurs less frequently after C-PLB. Overall, this is a safe procedure when performed in a dedicated Radiology suite by experienced Interventional Radiologists, with no major complications encountered across 274 procedures over a 4-year period. Larger, prospective randomised control trials are required to further investigate the comparative risk of post-procedural complications.</p><p>\n \n </p><p><b>561</b></p><p><b>Inflammatory Bowel Disease Paediatric Quality of Care Hospital Audit 2023 in Australia</b></p><p><b>Mia Komesaroff</b><sup>1</sup>, Laura Rishanghan<sup>1</sup>, Stephan Moller<sup>2</sup>, David Skvarc<sup>3</sup>, George Alex<sup>4</sup>, Christopher Burgess<sup>5</sup>, Ramesh Nataraja<sup>1</sup>, Antonia Mikocka-Walus<sup>3</sup>, Wayne Massuger<sup>6</sup> and Edward Giles<sup>1,6</sup></p><p><sup>1</sup><i>Gastroenterology, Monash Health, Melbourne, Australia;</i> <sup>2</sup><i>Crohn's and Colitis Australia, Melbourne, Australia;</i> <sup>3</sup><i>Deakin University, Adelaide, Australia;</i> <sup>4</sup><i>Gastroenterology, Royal Children's Hospital, Melboune, Australia;</i> <sup>5</sup><i>Gastroenterology, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>6</sup><i>Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Inflammatory bowel disease is a chronic, lifelong gastrointestinal disorder, with 8-10% patients diagnosed before 18 years old. The quality of care for these young people can be variable and a previous 2016 hospital audit showed Australian hospital did not meet the specified standards. The objectives of this study were to re-look at organisation, resources and delivery of hospital care to young people with IBD and identify changes since 2016.</p><p><b><i>Methods:</i></b> This audit was conducted in collaboration with the patient organisation Crohn’s & Colitis Australia. Hospitals nationally were invited to participate in an online survey looking at organisation and resources of care, as well as a clinical audit of inpatient overnight admissions for 2021. Eight hospitals participated looking at 186 admissions, which captured 23% of public hospital admissions for IBD patients in 2021.</p><p><b><i>Results:</i></b> We found there was limited access to multidisciplinary care, with only 23% of CD inpatients being seen by and IBD nurse, compared to 33% in 2014. Despite psychological comorbidity in 28% of cases, psychologists were not part of the team at any site. The use of preventive anti-thrombotic reduced to 10% in 2021, from 30% in 2014 (p<0.001) despite new clinical guidelines supporting use. Of note, sites reported new, off label IBD medications were used in 56 young people. UC surgical admissions reduced to 5% in 2021 from 16% in 2014 (p>0.05). This occurred despite increased in UC admissions overall (almost doubled nationally). The use of corticosteroids for than 3 months in the year prior to admission reduced from 1% to 10% in 2014.</p><p><b><i>Conclusions:</i></b> This audit helped build recommendations including increased support for multidisciplinary team, improved mental health support and streamline access to newer medication.</p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":"39 S1","pages":"321-330"},"PeriodicalIF":3.4000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16707","citationCount":"0","resultStr":"{\"title\":\"Paediatrics\",\"authors\":\"\",\"doi\":\"10.1111/jgh.16707\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>6</b></p><p><b>Comparing real-world utilisation of dietary and medical therapies in paediatric and adult inflammatory bowel disease patients using CCCare: A cross-sectional study</b></p><p><b>Joseph Pipicella</b><sup>1,2,3</sup>, Wai Kin Su<sup>1,3,4</sup>, William Wilson<sup>5,6</sup>, Jane Andrews<sup>1,7,8</sup> and Susan J Connor<sup>1,2,3,4</sup></p><p><sup>1</sup><i>Crohn's Colitis Cure, Sydney, Australia;</i> <sup>2</sup><i>South West Sydney Clinical Campus, University of New South Wales, Sydney, Australia;</i> <sup>3</sup><i>Ingham Institute for Applied Medical Research, Sydney, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia;</i> <sup>5</sup><i>SA Health, Adelaide, Australia;</i> <sup>6</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>7</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>8</sup><i>Faculty of Health Sciences, School of Medicine, University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Approximately 10% of people with inflammatory bowel diseases (IBD) are diagnosed in childhood. Crohn’s Colitis Care (CCCare) is an IBD-specific electronic medical record (EMR) used across Australia and New Zealand, with a recent upgrade to incorporate paediatric functionality. Using CCCare, we explored the real-world use of dietary and medical therapies across the age spectrum in people with IBD under routine ambulatory care in ANZ.</p><p><b><i>Methods:</i></b> De-identified data from CCCare’s linked clinical quality registry were analysed in April 2024. All people with IBD under active care (clinical encounter within the prior 14 months) were included. Children were defined as being <18 years of age at time of extraction.</p><p><b><i>Results:</i></b> A total of 6,396 people with IBD were included. In the <18 years age group (n=172), 59.1% (n=101) were male with a median age of 15 years (IQR 12.8-16). The majority (93%, n=93) resided in Australia, and most had Crohn’s disease (66.5%, n=113), with 16.8% of them having ever had a perianal fistula. In the ≥18 years age group (n=6,224), 49.1% (n=3,055) were male with a median age of 42 years (IQR 32-57). The majority (76.5%, n=4,761) resided in Australia, and over half had Crohn’s disease (55.7%, n=113), with 15.9% having ever had a perianal fistula.Interestingly, 5-aminosalicylate use was more prevalent in adults than children (34% vs 27% respectively, P<0.05), whereas current immunomodulator use was less common in adults compared to children (29% vs 60% respectively, P<0.001). Current steroid use was ≤4% in both cohorts (P=0.26). Advanced therapy use by age group is shown below. Anti-TNF therapies (infliximab and adalimumab) were the predominant therapies in the paediatric cohort. Across the cohort, infliximab use decreased with age, whereas vedolizumab use increased with age. Dietary therapies were infrequently used/documented, with only 5/172 (2.9%) receiving dietary therapy in the paediatric cohort (Exclusive Enteral Nutrition [EEN]=4, Crohn's Disease Exclusion Diet [CDED]=1) and 49/6224 (0.8%) in the adult cohort (EEN=36, CDED=13) (p<0.001).</p><p><b>12</b></p><p><b>Meta-analysis of the pooled positive predictive value of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) no-biopsy approach for coeliac disease testing in children</b></p><p>Angharad Vernon-Roberts<sup>3</sup>, Sanjeev Verma<sup>4</sup>, Andrew Day<sup>3</sup> and <b>Shaun Ho</b><sup>1,2</sup></p><p><sup>1</sup><i>Royal Children's Hospital Melbourne, Parkville, Australia;</i> <sup>2</sup><i>Murdoch Children Research Institute, Parkville, Australia;</i> <sup>3</sup><i>University of Otago Christchurch, Christchurch, New Zealand;</i> <sup>4</sup><i>King George Medical University, Lucknow, India</i></p><p><b><i>Background and Aim:</i></b> The 2012 and 2020 ESPGHAN guidelines for the diagnosis of coeliac disease (CD) in children included a non-biopsy approach for children meeting specific criteria; ≥10 times the upper limit of normal anti-tissue transglutaminase IgA antibody, positive endomysial IgA antibody, +/- positive coeliac HLA haplotypes (HLA). The aim of the study was to perform a meta-analysis of the overall CD diagnostic accuracy using the ESPGHAN non-biopsy criteria in children who also had small bowel biopsy (SBB) confirmation as the reference standard.</p><p><b><i>Methods:</i></b> Database searches (Medline, Embase, Web of Science, Scopus) were done in October 2023 and studies underwent stages of exclusion if they did not adhere to the ESPGHAN criteria and have SBB confirmation. A random effects meta-analysis provided a pooled positive predictive value (PPV) for all studies, sub-group analysis was carried out to identify sources of heterogeneity.</p><p><b><i>Results:</i></b> Searches identified 1053 articles, with 21 included in the final analysis. While study sample sizes ranged from 39 to 707 with a total of 4087, 2323 children fulfilled the ESPGHAN non-biopsy criteria and of these 2289 had comparative SBB and were included in the final meta-analysis. The proportion of CD cases diagnosed using the ESPGHAN non-biopsy approach compared to SBB ranged from 79.2-100% in studies, with an overall pooled PPV of 97.3% (CI 95.4,98.6) [Figure 1]. Between study heterogeneity was high (I2 79.2%, p<0.0001, CI 68.8,86.1), explored using sub-group analysis that showed higher PPV for studies using prospective methodologies (p=0.001). Sensitivity analysis showed that PPV was higher in studies applying the ESPGHAN criteria that included positive HLA, versus the criteria without HLA (PPV 98.5 vs 96.7, p=0.014).</p><p><b>55</b></p><p><b>Collagenous gastritis in children: response to oral budesonide</b></p><p><b>Jay Sharma</b> and Ryan Joseph Anson and Ajay Sharma</p><p><i>University Of Western Australia, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Collagenous gastritis(CG) is a rare disease in children characterized by the subepithelial deposition of collagen bands and inflammatory infiltrates in the gastric lamina propria with no effective treatment described to date. We aim to describe the outcomes of 3 patients with a 3 months course of oral Budesonide that will contribute to improved therapeutic options for this rare condition.</p><p><b><i>Methods:</i></b> A retrospective chart review (0-18 years) in the last 10 years was reviewed (2013-2023) with a total of 3 cases of CG identified.</p><p><b><i>Results:</i></b></p><p><b>Case 1:</b> A 15-year-old female presented with significant anaemia with haemoglobin of 71 g/L (NR-125-175 g/L) with ferritin < 5 ug/L (NR 20-200 ug/L). Esophagogastroduodenoscopy revealed CG in histology. She was started on a 3-month course of Oral Budesonide 9 mg, 6 mg and 3 mg with a repeat Hb and ferritin levels remaining in the normal range.</p><p><b>Case 2:</b> A 17-year-old male was referred with anaemia despite trialling PPI and oral iron. EGD confirmed CG and on daily 3 months of Budesonide with a similar regimen as Case 1, had stable Iron levels and Hb.</p><p><b>Case 3:</b> A 15 yo presented with fatigue (Hb 57 g/dl) and failed trial of PPI and oral iron. EGD confirmed CG and a similar regimen was followed as case 1 with Ferritin and Hb staying in the normal range after 3 months.</p><p><b><i>Conclusions:</i></b> This case series demonstrates considering trialling a 3-month weaning course of Budesonide if Oral iron therapy and PPI trial fail and it could be an effective therapeutic option for the CG patients though it's unclear whether this regimen could be considered a safe long-term option. Further research is needed to understand the Pathophysiology and treatment target.</p><p><b>148</b></p><p><b>An automated approach to the analysis of paediatric high-resolution colonic manometry data: characterisation of the meal response in children with Hirschsprung disease using a Bayesian functional mixed effects model</b></p><p><b>Hannah Evans-Barns</b><sup>1,2,3</sup>, Lukasz Wiklendt<sup>6</sup>, John Hutson<sup>2,3,4</sup>, Warwick Teague<sup>1,2,3</sup>, Mark Safe<sup>5</sup>, Sebastian King<sup>1,2,3</sup> and Phil Dinning<sup>6</sup></p><p><sup>1</sup><i>Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Australia;</i> <sup>2</sup><i>Surgical Research Group, Murdoch Children's Research Institute, Melbourne, Australia;</i> <sup>3</sup><i>Department of Paediatrics, University of Melbourne, Melbourne, Australia;</i> <sup>4</sup><i>Department of Urology, The Royal Children’s Hospital, Melbourne, Australia;</i> <sup>5</sup><i>Department of Gastroenterology and Clinical Nutrition, The Royal Children’s Hospital, Melbourne, Australia;</i> <sup>6</sup><i>Gastroenterology Department, Flinders Medical Centre, Bedford Park, Australia</i></p><p><b><i>Background and Aim:</i></b> Post-operative bowel dysfunction is prevalent in children with Hirschsprung disease (HD). The aim of this study was to characterise the colonic meal response, recorded by high-resolution manometry (HRCM), using a Bayesian functional mixed effects model, and compare findings to healthy controls.</p><p><b><i>Methods:</i></b> A HRCM catheter was positioned in the colon with sensors spanning the caecum to rectum. A one hour baseline recording was followed by a meal challenge and a further one hour recording. The control group consisted of 13 healthy adults. Cross-wavelet analysis was used to compute the frequency and direction of all propagating pressure waves (PPW). A latent Gaussian Process model was used compare the effects of the meal on PPW within, and between, patients and controls. Ethical approval was obtained (HREC 64192).</p><p><b><i>Results:</i></b> A meal was eaten by 13 children (12 male; 6.83±2.56 years; 9/13 short-segment). In the proximal colon, while the meal induced a significant increase both antegrade and retrograde PPW across a range of frequencies (1/16 to 8 cycles per minute [cpm]), the effect was significantly reduced in HD (Figure). In the distal colon of controls, the meal induced a significant increase in all PPWs between 1/16 – 8 cpm. In HD, the meal did not increase PPW between 2-10cpm.</p><p><b>152</b></p><p><b>Crossed wires: aligning clinical practice with family experiences in paediatric temporary tube feeding</b></p><p><b>Claire Reilly</b><sup>1,2</sup>, Jeanne Marshall<sup>1,2</sup>, Rebecca Packer<sup>1</sup>, Jasmine Foley<sup>1</sup> and Nikhil Thapar<sup>1,2,3</sup></p><p><sup>1</sup><i>The University Of Queensland, Brisbane, Australia;</i> <sup>2</sup><i>Children's Health Queensland, Brisbane, Australia;</i> <sup>3</sup><i>Queensland University of Technology, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Temporary tube feeding is crucial for children requiring short-term nutritional support, yet its impact on families is under-researched. This study aimed to compare the perspectives of families of children with temporary feeding tubes with the clinicians who managed them, with the goal of enhancing understanding, improving clinical practice and investigating the children’s quality of life.</p><p><b><i>Methods:</i></b> This study, part of a larger mixed-methods research project at a major children’s hospital, collected data from families of children discharged home with a temporary feeding tube (e.g., nasogastric tube) using electronic diaries and semi-structured interviews. Medical records were reviewed, and quality of life was assessed using the Pediatric Quality of Life Inventory version 4.0 Generic Core Scales (PEDsQL) at key time points (tube insertion, midpoint, removal). Clinicians completed an online survey.</p><p><b><i>Results:</i></b> This study included 37 children with temporary feeding tubes, and 112 clinicians (medical practitioners, nursing, and allied health) overseeing their care. Communication gaps were prevalent: whilst 95% (n=35) of families were informed about the tube’s necessity, only 12% (n=4) recalled being told about the expected duration, despite 44% (n=49) of clinicians describing having this conversation. The medical notes revealed that only one child had a tube exit plan, despite 28 clinicians reporting completing this. Importantly, 32% (n=35) of clinicians were unable to recall whether estimated tube feeding duration was ever discussed. Additionally, whilst 61% (n=68) of clinicians provided written information about the feeding tube, 16% (n=18) were unable to recall whether or not they did. Seven children received feeding tubes despite documented parental objections in their medical notes. Preliminary quality of life results indicated a mean PEDS-QL score of 53.2 (SD±15.9) at tube insertion, 61.5 (SD±16.9) at midpoint, and 65.8 (SD±19.3) at the endpoint. These scores are lower than those reported in healthy children (83.9; SD±12.5), and lower when compared to studies of children with other health conditions.</p><p><i><b>Conclusion:</b></i> This study revealed substantial disparities in clinical decision-making and communication regarding temporary feeding tubes. These children experienced lower reported quality of life compared to their healthy peers and those with other health conditions. There is a discrepancy between the care clinicians believe they provide and what families retain. This study recommends improved guidelines for communication, education, and documentation to better align clinical practices with family needs, ensuring better outcomes for this group of children.</p><p><b>306</b></p><p><b>Proactive therapeutic drug monitoring (TDM) of infliximab leads to durability of treatment in children with inflammatory bowel disease</b></p><p><b>Cher Wei Chuah</b><sup>1</sup> and <b>Shoma Dutt</b><sup>1,2</sup></p><p><sup>1</sup><i>Department Of Gastroenterology, The Children's Hospital At Westmead, Westmead, Australia;</i> <sup>2</sup><i>CHW Clinical School University of Sydney, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Anti-tumour Necrosis Factor therapies are the only biological therapy approved on the pharmaceutical benefits scheme (PBS) for children in Australia. Loss of response to the 1<sup>st</sup> biological predicts poorer responses to subsequent biologicals<sup>1</sup>. Maintaining and preserving response is beneficial in the paediatric age group. Published literature suggest that one third of patients will develop secondary loss of response (LOR) by the first year and up to 50% of initial responders will develop LOR by 5 years.<sup>2</sup> Evidence suggest sustained high trough levels increases the durability of infliximab. The ability to recapture response in secondary LOR with dose escalation is well described.<sup>3</sup> In 2019, our unit opted for proactive TDM (at week 6, week 14 and 6 monthly thereafter) and dose escalation based on cutoffs at week 6 < 15 μg/mL, week 14/maintenance < 5 μg/mL as standard practice, in addition to the usual practice of escalation guided by the clinical picture.<sup>4</sup> We report the outcomes of our patient cohort over a period of 2 years from initiation of infliximab.</p><p><b><i>Methods:</i></b> A retrospective chart review of patients commenced on infliximab was performed between 01/01/2019 to 31/12/2021. Only patients who completed induction were included, patients with acute severe colitis were excluded from this report as they were escalated on different parameters and will be reported separately. Data on demographics, disease characteristics, immunomodifier usage, infliximab dosing and frequency, infliximab drug levels, and antibody levels and switching to alternative biologics were collected and analysed. A physician global assessment (PGA) scale of remission, mild, moderate, and severe was used to assess clinical outcomes. Standard infliximab dosing is 5mg/kg at 0, 2, 6 weeks for induction and every 8 weeks during maintenance phase. Escalation was defined as either shortening of standard interval and/or increased dose to 10mg/kg.</p><p><b><i>Results:</i></b> 98 patients (58% male) were identified, 82% had Crohn’s disease (CD) and 18% Ulcerative Colitis (UC). Median age at diagnosis was 11 years old, and 12.5 years old at starting infliximab. 81% received an immune modifier of which 64% had methotrexate and 39% azathioprine. 13% received escalated induction and 77% escalated maintenance. 3% failed to achieve remission and were discontinued. 2% developed infliximab antibodies. 8% of patients were switched to an alternate biologic by 1 year and 18% by 2 years, median time to switch was 53 weeks. Of those that remained on infliximab, 83% were in clinical remission at 1 year and 94% at 2 years. Switching to alternate biologic was associated with escalated induction, OR 5.8 (1.5 – 22.5, p = 0.01) UC, OR 5.6 (1.8 – 17.5, p < 0.01) and concomitant steroid use, OR 4.1 (1.1-15.5, p = 0.04). Immunomodulator use was not associated with switching biologics (p = 0.84). No patients on escalated induction developed antibodies (p = 0.58) and 1 patient on escalated maintenance developed antibodies (p = 0.48). There was no significance difference with standard or escalated maintenance with the PGA at the 1-year (p = 0.14) and 2 –year mark (p = 0.49).</p><p><b><i>Conclusion:</i></b> Proactive TDM and escalation of infliximab results in good durability with treatment persistence at 92% at 1 year and 82% at 2 year and an excellent clinical remission rate of 94% at 2 years. Escalated induction and UC were predictors to switch biologics which is in keeping with primary non-responders/severe phenotype. Vahabnezhad et al reports in their series of paediatric CD also treated with escalated infliximab had treatment persistence of 80% at 2 years.<sup>3</sup> Our CD cohort had 88% who remain on infliximab at 2 years. This study provides real world evidence that the subset of patients that responds well to infliximab can be maintained on this therapy longer than what is in the current published literature and merit that escalated therapy is funded by the PBS.</p><p><b>References</b></p><p>\\n 1. <span>Gisbert, J. P.</span>, & <span>Chaparro, M.</span> (<span>2020</span>). <span>Predictors of Primary Response to Biologic Treatment [Anti-TNF, Vedolizumab, and Ustekinumab] in Patients With Inflammatory Bowel Disease: From Basic Science to Clinical Practice</span>. <i>Journal of Crohn's & colitis</i>, <span>14</span>(<span>5</span>), <span>694</span>–<span>709</span>. https://doi.org/10.1093/ecco-jcc/jjz195</p><p>\\n 2. <span>Ding, N. S.</span>, <span>Hart, A.</span>, & <span>De Cruz, P.</span> (<span>2016</span>). <span>Systematic review: predicting and optimising response to anti-TNF therapy in Crohn's disease - algorithm for practical management</span>. <i>Alimentary pharmacology & therapeutics</i>, <span>43</span>(<span>1</span>), <span>30</span>–<span>51</span>. https://doi.org/10.1111/apt.13445</p><p>\\n 3. <span>Vahabnezhad, E.</span>, <span>Rabizadeh, S.</span>, & <span>Dubinsky, M. C.</span> (<span>2014</span>). <span>A 10-year, single tertiary care center experience on the durability of infliximab in pediatric inflammatory bowel disease</span>. <i>Inflammatory bowel diseases</i>, <span>20</span>(<span>4</span>), <span>606</span>–<span>613</span>. https://doi.org/10.1097/MIB.0000000000000003</p><p>\\n 4. <span>Rheenen, P. F.</span>, <span>Aloi, M.</span>, <span>Assa, A.</span>, et al. (<span>2020</span>). <span>The Medical Management of Paediatric Crohn's Disease: an ECCO-ESPGHAN Guideline Update</span>. <i>Journal of Crohn's & colitis</i>, jjaa161. Advance online publication. https://doi.org/10.1093/ecco-jcc/jjaa161</p><p><b>350</b></p><p><b>Changes in paediatric inflammatory bowel disease care at a paediatric tertiary hospital from 2014 to 2021</b></p><p><b>Jessica Nguyen</b><sup>1</sup>, Joan Cheng<sup>2</sup> and Edward Giles<sup>3,4</sup></p><p><sup>1</sup><i>Department of Paediatric Gastroenterology, Monash Children's Hospital, Monash Health, Clayton, Australia;</i> <sup>2</sup><i>Faculty of Medicine, Nursing and Health Sciences, Monash University, Clayton, Australia;</i> <sup>3</sup><i>Department of Paediatrics, Monash University, Clayton, Australia;</i> <sup>4</sup><i>Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Clayton, Australia</i></p><p><b><i>Background and Aim:</i></b> The recent Paediatric Inflammatory Bowel Disease (PIBD) quality of care project investigated the care of children with IBD in Australia in 2021. This included a national audit of patient care that was almost directly comparable to the IBD audit from 2014. This provided an opportunity for all hospitals that were involved in both audits to examine how their care had changed.</p><p><b><i>Methods:</i></b> Organisational data (including total admissions, staffing etc) from our paediatric tertiary hospital from 2014 to 2021 were compared. In addition, inpatient admissions data was audited from patients with ulcerative colitis (UC) and Crohn’s disease admitted. Statistical analysis was performed using Chi-Square test (Prism software).</p><p><b><i>Results:</i></b> From 2014 to 2021, we had similar number of Crohn’s disease admissions (15 in 2014, 14 in 2021); however, double the number of UC admissions (12 in 2014, 24 in 2021, See figure 1) The most common length of stay was between 3-6 days for both Crohn’s and UC. In 2021, a smaller percentage of Crohn’s patients had a previous admission (78% in 2014 down to 43%, p<0.0001). In UC patients, a higher percentage of patients had a previous admission (25% up to 48%, p=0.0007). In 2021, there were more patients with anaemia (64% in 2021 compared to 33% in 2014 in Crohn’s disease, p<0.0001; 60% in 2021 compared to 25% in 2014 in UC, p<0.0001) and malnutrition on admission (6 compared to 2 with Crohn’s disease, p=0.0015; 4 compared to 1 with UC, p=0.1649).</p><p><b>362</b></p><p><b>A population-based study of the prevalence and metabolic significance of steatotic liver disease in children and their parents</b></p><p><b>Oyekoya Ayonrinde</b><sup>1,2,3</sup>, Shailender Mehta<sup>1</sup>, Stephanie Dowden<sup>4</sup>, Timothy Fairchild<sup>5</sup>, Gina Ambrosini<sup>6</sup>, Desiree Silva<sup>2,7</sup>, Kemi Wright<sup>8</sup>, Sheeraz Mohd<sup>1</sup>, Leela King<sup>1</sup>, Seyifunmi Afolabi<sup>9</sup> and Janine Spencer<sup>1</sup></p><p><sup>1</sup><i>Fiona Stanley Hospital, Murdoch, Australia;</i> <sup>2</sup><i>The University of Western Australia, Perth, Australia;</i> <sup>3</sup><i>Curtin University, Bentley, Australia;</i> <sup>4</sup><i>NursePrac Australia, Success, Australia;</i> <sup>5</sup><i>Murdoch University, Murdoch, Australia;</i> <sup>6</sup><i>Healthway, Perth, Australia;</i> <sup>7</sup><i>Joondalup Hospital, Joondalup, Australia;</i> <sup>8</sup><i>University of New South Wales, Sydney, Australia;</i> <sup>9</sup><i>Oceania University of Medicine, Brisbane, Australia</i></p><p><b><i>Background and Aims:</i></b> Steatotic liver disease (SLD) is the most common chronic liver disorder globally. SLD in childhood reflects prevalent metabolic dysfunction in children and families and poses increased longer-term risk of early-onset cardiometabolic and liver-related complications. We examined the prevalence and metabolic significance of SLD in children and their parents.</p><p><b><i>Method:</i></b> Population-based children, aged 5-15 years, and their parents participated in a cross-sectional observational study of SLD in Perth, Australia. Assessments included anthropometry (weight, height, waist circumference and skinfold thickness [SFT]) and blood tests. Utilising Fibroscan® we non-invasively examined the severity of hepatic steatosis using controlled attenuation parameter (CAP), and severity of liver fibrosis using transient elastography (TE)-measured liver stiffness measurement (LSM). SLD was defined by CAP ≥249 dB/m in children and ≥275 in parents. Children aged 5-10 years were considered as young children and those aged 11-15 years as older children. SLD in children was considered to be metabolic dysfunction-associated SLD (MASLD). We compared cardiometabolic characteristics of children with versus those without MASLD, and sought associations between MASLD in children and parent characteristics.</p><p><b><i>Results:</i></b> One hundred and fifteen children (50% male), with mean [SD] age 9.6[2.7] years, 74 mothers aged 40.7[5.8] years and 24 fathers aged 44.2[5.8] participated in the study. One child did not have FibroScan® assessment. Seventy-three children (64%) were young children. Compared with older children, young children had lower body weight, height and waist circumference (p<0.05), but skinfold thickness, CAP, LSM, serum lipids, leptin, high sensitivity C-reactive protein (hsCRP) and liver enzyme levels were not significantly different (p>0.05 for all). Comparing boys vs. girls, there were no significant differences in anthropometric measures of adiposity or CAP overall (p>0.05 for all). Mean (SD) WC was 88.3(13.4) cm in mothers and 91.8 (10.9) cm in fathers. Mean BMI was 27.7 (5.3) kg/m<sup>2</sup> in mothers and 27.3 (3.0) kg/m<sup>2</sup> in fathers. SLD was diagnosed in 20.2% children (15.8% male vs. 24.6% female, p=0.24), 29.9% mothers and 37.5% fathers. SLD was seen in 55% of children with BMI ≥30 kg/m<sup>2</sup>. Children with MASLD had greater subcutaneous fat measured as SFT, serum alanine aminotransferase (ALT), leptin, hsCRP, and triglycerides, and lower levels of high-density lipoprotein cholesterol, compared with those without SLD (p<0.05 for all, Table 1). CAP in children was positively correlated with BMI z-score, waist circumference, skinfold thickness, weight, ALT, gamma glutamyl transpeptidase (GGT), triglycerides, leptin, and maternal and paternal BMI (p<0.05 for all). There was no significant correlation between SLD in children and their parents, however mothers of children with SLD had higher mean BMI than mothers of children without SLD (30.3[5.7] kg/m<sup>2</sup> vs. 27.1[5.1] kg/m<sup>2</sup>, p=0.04), and fathers had higher mean liver stiffness measurement (LSM), (7.6[4.6] kPa vs. 4.8[1.2] kPa, p=0.02. Using multivariable logistic regression analysis, child ALT (OR 1.21, 95% CI 1.01-1.45) and abdominal SFT (OR 1.59, 95% CI 1.03-2.44) were associated with SLD in children, after adjusting for child WC (OR 0.94, 95% CI 0.87-1.04), and maternal BMI (OR 1.22, 95% CI 0.85-1.76).</p><p><b><i>Conclusion:</i></b> MASLD is common in children, and is associated with increased adiposity, raised ALT, features of metabolic dysfunction, maternal adiposity, and paternal liver stiffness. Our findings suggest intergenerational heritability of metabolic and hepatic risk.</p><p><b>471</b></p><p><b>Similar outcomes following early proactive vs reactive therapeutic drug monitoring in children with Crohn’s disease commencing infliximab – a single centre, retrospective study</b></p><p><b>Asha Jois</b><sup>1</sup>, Rachel Horn<sup>1</sup>, Anysha Walia<sup>1</sup>, Eric Cheah<sup>2</sup>, Robert Little<sup>3</sup> and George Alex<sup>1,4</sup></p><p><sup>1</sup><i>Royal Children's Hospital, Parkville, Australia;</i> <sup>2</sup><i>Monash Children's Hospital, Clayton, Australia;</i> <sup>3</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>4</sup><i>University of Melbourne, Parkville, Australia</i></p><p><b><i>Background and Aim:</i></b> Benefits of a proactive compared to a reactive therapeutic drug monitoring (TDM) strategy when commencing infliximab (IFX) for management of Crohn’s disease are unclear. We evaluated the 6- and 12-month outcomes in children commencing IFX with proactive week 14 TDM compared to those without week 14 TDM.</p><p><b><i>Methods:</i></b> Single-centre, retrospective study of Crohn’s disease patients aged 0-18 years with a primary response to IFX induction between 2018-2021. Proactive TDM was defined by measurement of a week 14 IFX drug level and reactive TDM was defined by no week 14 drug level. Baseline patient, medication and disease characteristics were compared across the two groups. Clinical and biochemical disease activity measures, and IFX dose, frequency and drug level were compared across the two groups at week 0, 6- and 12-months post-induction. Failure was defined by biologic switch, corticosteroid use, hospitalisation or surgery.</p><p><b><i>Results:</i></b> We included 86 patients. 34/86 (40%) were female, diagnosed at median 13 years, with a median disease duration of 4 years. 40/86 (47%) had proactive TDM – baseline characteristics by group are presented in Table 1. At 12-months, there was no difference in failure rates (15% vs. 23%, p = 0.419) or IFX persistence (95% vs. 89%, p = 0.442) between the proactive and reactive TDM groups, respectively. At 6-months, the proactive group had more escalated IFX dose frequency (23% vs. 5%, p = 0.023), but IFX dose was comparable (5.8 vs. 5.5 mg/kg, p = 0.108). There was no difference in IFX drug level or disease severity at either 6- or 12-months.</p><p><i><b>Conclusion:</b></i> In children with Crohn’s disease commenced on IFX, week 14 proactive TDM was not associated with improved outcomes at 12-months compared to children without week 14 TDM, and IFX drug levels were comparable. Prospective studies are required to identify the optimal TDM strategy.</p><p><b>480</b></p><p><b>Subcutaneous infliximab use in children with inflammatory bowel disease in a tertiary paediatric hospital</b></p><p><b>Jessica A Eldredge</b><sup>1</sup>, Cher Wei Chuah<sup>1</sup>, Michelle Tano<sup>1</sup>, Trudy Chidgey, Noel Singh<sup>1,2</sup>, Kunal Thacker<sup>1</sup>, Annabel Magoffin<sup>1</sup> and Shoma Dutt<sup>1</sup> and Edward O'Loughlin<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Children's Hospital at Westmead, Australia;</i> <sup>2</sup><i>Pharmacy Department, Children's Hospital at Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Anti-Tumour Necrosis Factor (anti-TNF) therapies remain the only biological treatment accessible for use in Australian children with moderate to severe inflammatory bowel disease (IBD) via the Pharmaceutical Benefits Scheme. SC infliximab is now well-established in adult IBD care (1-3). Compared to traditional IV formulations, SC dosage may offer relative pharmacokinetic stability with sustained drug delivery, with comparable efficacy, safety and immunogenicity profiles (1-3). Published literature demonstrates that in younger IBD patients, the majority would prefer to switch to subcutaneous (SC) versions of their current intravenous (IV) biologic (1,2). Scarce real-world data is available on use of SC infliximab in paediatric IBD, with only seven children described from a single-centre cohort study in Edinburgh (4). We aimed to assess the clinical efficacy, tolerability and cost-benefit of SC infliximab, as part of an initiative supported by our local institutional Medicines and Therapeutics Committee.</p><p><b><i>Methods:</i></b> We report twelve children with IBD who commenced 120mg fortnightly SC infliximab dosing between February to May 2024. Baseline, 4, 8 and 12 week follow-up biochemical and clinical assessments were undertaken over this treatment period. Nine of twelve children were male, with median age 14.5 years [range 6-17 years]. Eleven had a diagnosis of Crohn’s disease. Two children received SC infliximab as the third dose in their induction therapy and ongoing. Ten children were transitioned from stable infliximab IV maintenance dosing. All were prescribed concomitant immunomodulator therapy (azathioprine or methotrexate).</p><p><b><i>Results:</i></b> Clinical and biochemical parameters for children treated with subcutaneous infliximab are outlined in Table 1. Clinical disease activity indices (Paediatric Crohn’s Disease Activity Index [PCDAI] or Paediatric Ulcerative Colitis Activity Index [PUCAI]) were stable or improved over the treatment period. Median baseline infliximab level prior to first SC dose was 9.2 mg/L [IQR 7.1 – 11.0] with calprotectin 53.5ug/g [IQR 20-334]. Infliximab level increased by a median of 9.3mg/L [IQR 0.7-12.3], and calprotectin reduced by median 32ug/g [IQR -92.5-35.5] over the 12 week follow-up period. No significant adverse events were observed. Combined cost of escalated non-PBS infliximab intravenous dosing, day medical unit admission and consumables saved was estimated at $12,304.92 per patient per annum in this group.</p><p><b><i>Conclusion:</i></b> Calprotectin and clinical disease activity indices were stable or on average improved following twelve weeks of SC infliximab dosing in twelve children with IBD. We propose subcutaneous infliximab may be an efficacious and cost-saving treatment alternative to IV dosing in children with IBD, reducing healthcare costs (admissions for IV infusions), and financial and educational impacts on patients and families (lost work and school days). Further data in larger cohorts of children is required, including quality-of-life and cost-saving assessment scales.</p><p><b>References</b></p><p>\\n 1. <span>Buisson, A</span>, <span>Nachury, M</span>, <span>Reymond, M</span> et al. <span>Effectiveness of Switching From Intravenous to Subcutaneous Infliximab in Patients With Inflammatory Bowel Diseases: the REMSWITCH Study</span>. <i>Clin Gastroenterol Hepatol</i> <span>2023</span>; <span>21</span>: <span>2338</span>-<span>46.e3</span>.</p><p>\\n 2. <span>Schreiber, S</span>, <span>Ben-Horin, S</span>, <span>Leszczyszyn, J</span> et al. <span>Randomized Controlled Trial: Subcutaneous vs Intravenous Infliximab CT-P13 Maintenance in Inflammatory Bowel Disease</span>. <i>Gastroenterology</i> <span>2021</span>; <span>160</span>: <span>2340</span>-<span>53</span>.</p><p>\\n 3. <span>Strik, AS</span>, <span>Vrie, W</span>, <span>Bloemsaat-Minekus, JPJ</span> et al. <span>Serum concentrations after switching from originator infliximab to the biosimilar CT-P13 in patients with quiescent inflammatory bowel disease (SECURE): an open-label, multicentre, phase 4 non-inferiority trial</span>. <i>Lancet Gastroenterol Hepatol</i> <span>2018</span>; <span>3</span>: <span>404</span>-<span>12</span>.</p><p>\\n 4. <span>Gianolio, L</span>, <span>Armstrong, K</span>, <span>Swann, E</span> et al. <span>Effectiveness of Switching to Subcutaneous Infliximab in Pediatric Inflammatory Bowel Disease Patients on Intravenous Maintenance Therapy</span>. <i>J Pediatr Gastroenterol Nutr.</i> <span>2023</span>; <span>77</span>(<span>2</span>): <span>235</span>-<span>239</span>. https://doi.org/10.1097/MPG.0000000000003838.</p><p><b>481</b></p><p><b>An Australian paediatric experience using orodispersible budesonide in eosinophilic oesophagitis</b></p><p><b>Juliet Affum</b><sup>1</sup>, Geoff Withers<sup>1</sup>, Alberto Pinzon-Charry<sup>2,3,4</sup> and Looi Ee<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Hepatology & Liver Transplant, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Queensland Paediatric Immunology & Allergy Service, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>The University of Queensland, Brisbane, Australia;</i> <sup>4</sup><i>Griffith University, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is an atopic and debilitating condition which has emerged in the last three decades with limited treatment options. Targeted therapies were not available in Australia until recently. On 1<sup>st</sup> May 2022, Jorveza®, a budesonide orodispersible tablet was listed on the Pharmaceutical Benefits Scheme (PBS) specifically for treating EoE. Our aim was to review the paediatric experience in our centre with this therapy.</p><p><b><i>Methods:</i></b> Retrospective review of patients in a tertiary paediatric hospital who commenced this therapy between 1<sup>st</sup> May 2022 and 7<sup>th</sup> August 2023 was undertaken. Patient demographics, endoscopic appearance and histologic findings were recorded. Histologic remission was defined using two thresholds, <5 eos/hpf (PBS criteria) and ≤15 eos/hpf (standard criteria).</p><p><b><i>Results:</i></b> Sixty-three patients, 87% (55/63) male, median age 14 (range 8-17) years were treated during this period. Thirty-five (56%) had a gastroscopy within 3 months of starting Jorveza® while the rest were “grandfathered” as they were already on swallowed topical steroids. Only 10 patients were newly diagnosed and thus, treatment naïve. Eighty-seven percent (55/63) had repeat gastroscopy at median 3.7 (range 2.1-13.7) months after staring Jorveza®. Remission was achieved in 49.09% (≤15 eos/hpf, standard criteria) and 41.82% (<5 eos/hpf, PBS criteria) respectively. Female gender and medication adherence were significantly associated with remission. Post treatment oesophageal eosinophil count was lower in compliant patients compared to those with suboptimal medication adherence, mean 21 vs 79 eos/hpf, p=0.006. There was a trend to higher oesophageal eosinophil counts with longer duration between Jorveza® commencement and repeat endoscopy in both responders and non-responders, but this did not reach statistical significance.\\n\\n </p><p><i><b>Conclusion:</b></i> Jorveza® is an effective treatment for inducing histologic remission in children with EoE but is affected by compliance. Gender and medication adherence are significantly associated with histologic remission.</p><p><b>493</b></p><p><b>Percutaneous liver biopsy in children: comparison of complication rates between coaxial and noncoaxial techniques</b></p><p><b>Sudarshan Arvind</b><sup>1</sup> and <b>Murthy Chennapragada</b><sup>1,2</sup></p><p><sup>1</sup><i>The University of Sydney, Camperdown, Australia;</i> <sup>2</sup><i>The Children's Hospital Westmead, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Ultrasound guided percutaneous liver biopsy (PLB) is crucial in diagnosis and monitoring of paediatric liver disease. Two major techniques are used; coaxial (C-PLB) and non-coaxial (NC-PLB). C-PLB uses an outer needle sheath that penetrates the liver capsule, enabling a smaller biopsy needle to pass into the liver parenchyma. NC-PLB does not use an outer sheath, requiring more transgressions of the liver capsule to obtain the same number of cores of liver tissue. There is limited literature directly comparing complication rates following these techniques in children. The aim of this paper is to compare the incidence of complications following ultrasound-guided C-PLB and NC-PLB in children.</p><p><b><i>Methods:</i></b> This is a single-centre retrospective cohort study conducted at The Children’s Hospital Westmead (New South Wales). We studied paediatric patients who underwent ultrasound-guided PLB between September 2016 and December 2019. Patients were divided into C-PLB (n= 227) and NC-PLB (n= 47). Electronic medical records were used to gather demographic data, baseline characteristics, clinical indication and post-procedural complications (stratified into major or minor according to the Society of Interventional Radiology classification system). Chi-square analysis was used to compare demographic and baseline characteristics and to determine if there was a significant difference in the incidence of complications between these groups.</p><p><b><i>Results:</i></b> A total of 274 paediatric patients underwent ultrasound-guided PLB between September 2016 and December 2019. 227 underwent C-PLB (83%) while 47 underwent NC-PLB (17%). 51.5% of all PLB recipients were female. Biliary atresia (34.7%) was the most common primary diagnosis, followed by autoimmune hepatitis (8.4%). Coagulopathy or thrombocytopaenia (6.2%) was the most common pre-biopsy comorbidity. There were no major complications encountered across either cohort. Total incidence of minor complications was 17.9%. Minor complications occurred in 16.7% of the C-PLB cohort compared to 23.4% in the NC-PLB cohort. The difference was not significant (p=0.278). There was a significantly lower incidence of asymptomatic bleeding (p=0.002) in the C-PLB cohort compared to the NC-PLB cohort.</p><p><b><i>Conclusion:</i></b> Our findings do not suggest a significant difference in the incidence of complications following ultrasound-guided C-PLB vs. NC-PLB, with the exception of bleeding which occurs less frequently after C-PLB. Overall, this is a safe procedure when performed in a dedicated Radiology suite by experienced Interventional Radiologists, with no major complications encountered across 274 procedures over a 4-year period. Larger, prospective randomised control trials are required to further investigate the comparative risk of post-procedural complications.</p><p>\\n \\n </p><p><b>561</b></p><p><b>Inflammatory Bowel Disease Paediatric Quality of Care Hospital Audit 2023 in Australia</b></p><p><b>Mia Komesaroff</b><sup>1</sup>, Laura Rishanghan<sup>1</sup>, Stephan Moller<sup>2</sup>, David Skvarc<sup>3</sup>, George Alex<sup>4</sup>, Christopher Burgess<sup>5</sup>, Ramesh Nataraja<sup>1</sup>, Antonia Mikocka-Walus<sup>3</sup>, Wayne Massuger<sup>6</sup> and Edward Giles<sup>1,6</sup></p><p><sup>1</sup><i>Gastroenterology, Monash Health, Melbourne, Australia;</i> <sup>2</sup><i>Crohn's and Colitis Australia, Melbourne, Australia;</i> <sup>3</sup><i>Deakin University, Adelaide, Australia;</i> <sup>4</sup><i>Gastroenterology, Royal Children's Hospital, Melboune, Australia;</i> <sup>5</sup><i>Gastroenterology, Queensland Children's Hospital, Brisbane, Australia;</i> <sup>6</sup><i>Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Inflammatory bowel disease is a chronic, lifelong gastrointestinal disorder, with 8-10% patients diagnosed before 18 years old. The quality of care for these young people can be variable and a previous 2016 hospital audit showed Australian hospital did not meet the specified standards. The objectives of this study were to re-look at organisation, resources and delivery of hospital care to young people with IBD and identify changes since 2016.</p><p><b><i>Methods:</i></b> This audit was conducted in collaboration with the patient organisation Crohn’s & Colitis Australia. Hospitals nationally were invited to participate in an online survey looking at organisation and resources of care, as well as a clinical audit of inpatient overnight admissions for 2021. Eight hospitals participated looking at 186 admissions, which captured 23% of public hospital admissions for IBD patients in 2021.</p><p><b><i>Results:</i></b> We found there was limited access to multidisciplinary care, with only 23% of CD inpatients being seen by and IBD nurse, compared to 33% in 2014. Despite psychological comorbidity in 28% of cases, psychologists were not part of the team at any site. The use of preventive anti-thrombotic reduced to 10% in 2021, from 30% in 2014 (p<0.001) despite new clinical guidelines supporting use. Of note, sites reported new, off label IBD medications were used in 56 young people. UC surgical admissions reduced to 5% in 2021 from 16% in 2014 (p>0.05). This occurred despite increased in UC admissions overall (almost doubled nationally). The use of corticosteroids for than 3 months in the year prior to admission reduced from 1% to 10% in 2014.</p><p><b><i>Conclusions:</i></b> This audit helped build recommendations including increased support for multidisciplinary team, improved mental health support and streamline access to newer medication.</p>\",\"PeriodicalId\":15877,\"journal\":{\"name\":\"Journal of Gastroenterology and Hepatology\",\"volume\":\"39 S1\",\"pages\":\"321-330\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16707\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16707\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16707","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
1),亚组分析显示,采用前瞻性方法的研究PPV更高(P=0.001)。敏感性分析表明,采用包含阳性 HLA 的 ESPGHAN 标准的研究与不含 HLA 的标准相比,PPV 更高(PPV 98.5 vs 96.7,P=0.014)。55儿童胶原性胃炎:对口服布地奈德的反应Jay Sharma、Ryan Joseph Anson 和 Ajay Sharma澳大利亚珀斯西澳大利亚大学背景和目的:胶原性胃炎(CG)是一种罕见的儿童疾病,其特征是胃固有层胶原带上皮下沉积和炎症浸润,迄今为止尚未发现有效的治疗方法。我们旨在描述 3 名患者口服布地奈德 3 个月疗程的结果,这将有助于改进这种罕见疾病的治疗方案:结果:病例 1:一名 15 岁的女性患者出现严重贫血,血红蛋白为 71 克/升(正常值为 125-175 克/升),铁蛋白为 5 微克/升(正常值为 20-200 微克/升)。食管胃十二指肠镜检查在组织学中发现了 CG。她开始服用布地奈德口服液 9 毫克、6 毫克和 3 毫克,疗程为 3 个月,复查血红蛋白和铁蛋白水平仍在正常范围。病例 3:一名 15 岁患者因疲劳(血红蛋白 57 g/dl)就诊,服用 PPI 和口服铁剂无效。病例 3:一名 15 岁的患者因疲劳(血红蛋白为 57 g/dl)而来就诊,服用 PPI 和口服铁剂均未见效:本系列病例表明,如果口服铁剂和 PPI 试验失败,可以考虑试用布地奈德 3 个月的断药疗程,这对 CG 患者来说可能是一种有效的治疗方案,但目前还不清楚这种治疗方案是否可被视为一种安全的长期方案。要了解病理生理学和治疗目标,还需要进一步的研究。分析儿科高分辨率结肠测压数据的自动化方法:使用贝叶斯功能混合效应模型分析赫氏胃肠病患儿进餐反应的特征Hannah Evans-Barns1,2,3、Lukasz Wiklendt6、John Hutson2,3,4、Warwick Teague1,2,3、Mark Safe5、Sebastian King1,2,3和Phil Dinning61澳大利亚墨尔本皇家儿童医院小儿外科;2澳大利亚墨尔本默多克儿童研究所外科研究小组;3 澳大利亚墨尔本墨尔本大学儿科系;4 澳大利亚墨尔本皇家儿童医院泌尿科;5 澳大利亚墨尔本皇家儿童医院胃肠病学和临床营养学系;6 澳大利亚贝德福德公园弗林德斯医疗中心胃肠病学系背景和目的:赫氏普隆病(Hirschsprung disease,HD)患儿普遍存在术后肠道功能障碍。本研究的目的是利用贝叶斯功能混合效应模型,通过高分辨率测压(HRCM)记录结肠进餐反应的特征,并将结果与健康对照组进行比较:方法: 将一根 HRCM 导管插入结肠,传感器横跨盲肠和直肠。在进行一小时的基线记录后,再进行一小时的进餐挑战和记录。对照组由 13 名健康成人组成。交叉小波分析用于计算所有传播压力波 (PPW) 的频率和方向。使用潜在高斯过程模型比较了患者和对照组内部以及患者和对照组之间进餐对 PPW 的影响。研究获得了伦理批准(HREC 64192):13 名儿童(12 名男性;6.83±2.56 岁;9/13 名短段)进餐。在近端结肠中,虽然进餐会在不同频率(1/16 至 8 周/分 [cpm])范围内引起前向和逆向 PPW 的显著增加,但在 HD 中这种效应显著降低(图)。在对照组的远端结肠中,膳食导致 1/16 - 8 cpm 之间的所有 PPW 都显著增加。而在 HD 患者中,餐点不会增加 2-10 cpm 的 PPW。Crossed wires: aligning clinical practice with family experiences in paediatric temporary tube feedingClaire Reilly1,2, Jeanne Marshall1,2, Rebecca Packer1, Jasmine Foley1 and Nikhil Thapar1,2,31The University Of Queensland, Brisbane, Australia; 2Children's Health Queensland, Brisbane, Australia; 3Queensland University of Technology, Brisbane, Australia背景和目的:临时插管喂养对于需要短期营养支持的儿童至关重要,但对其对家庭的影响研究不足。
Comparing real-world utilisation of dietary and medical therapies in paediatric and adult inflammatory bowel disease patients using CCCare: A cross-sectional study
Joseph Pipicella1,2,3, Wai Kin Su1,3,4, William Wilson5,6, Jane Andrews1,7,8 and Susan J Connor1,2,3,4
1Crohn's Colitis Cure, Sydney, Australia;2South West Sydney Clinical Campus, University of New South Wales, Sydney, Australia;3Ingham Institute for Applied Medical Research, Sydney, Australia;4Department of Gastroenterology, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia;5SA Health, Adelaide, Australia;6Lyell McEwin Hospital, Adelaide, Australia;7Central Adelaide Local Health Network, Adelaide, Australia;8Faculty of Health Sciences, School of Medicine, University of Adelaide, Adelaide, Australia
Background and Aim: Approximately 10% of people with inflammatory bowel diseases (IBD) are diagnosed in childhood. Crohn’s Colitis Care (CCCare) is an IBD-specific electronic medical record (EMR) used across Australia and New Zealand, with a recent upgrade to incorporate paediatric functionality. Using CCCare, we explored the real-world use of dietary and medical therapies across the age spectrum in people with IBD under routine ambulatory care in ANZ.
Methods: De-identified data from CCCare’s linked clinical quality registry were analysed in April 2024. All people with IBD under active care (clinical encounter within the prior 14 months) were included. Children were defined as being <18 years of age at time of extraction.
Results: A total of 6,396 people with IBD were included. In the <18 years age group (n=172), 59.1% (n=101) were male with a median age of 15 years (IQR 12.8-16). The majority (93%, n=93) resided in Australia, and most had Crohn’s disease (66.5%, n=113), with 16.8% of them having ever had a perianal fistula. In the ≥18 years age group (n=6,224), 49.1% (n=3,055) were male with a median age of 42 years (IQR 32-57). The majority (76.5%, n=4,761) resided in Australia, and over half had Crohn’s disease (55.7%, n=113), with 15.9% having ever had a perianal fistula.Interestingly, 5-aminosalicylate use was more prevalent in adults than children (34% vs 27% respectively, P<0.05), whereas current immunomodulator use was less common in adults compared to children (29% vs 60% respectively, P<0.001). Current steroid use was ≤4% in both cohorts (P=0.26). Advanced therapy use by age group is shown below. Anti-TNF therapies (infliximab and adalimumab) were the predominant therapies in the paediatric cohort. Across the cohort, infliximab use decreased with age, whereas vedolizumab use increased with age. Dietary therapies were infrequently used/documented, with only 5/172 (2.9%) receiving dietary therapy in the paediatric cohort (Exclusive Enteral Nutrition [EEN]=4, Crohn's Disease Exclusion Diet [CDED]=1) and 49/6224 (0.8%) in the adult cohort (EEN=36, CDED=13) (p<0.001).
12
Meta-analysis of the pooled positive predictive value of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) no-biopsy approach for coeliac disease testing in children
Angharad Vernon-Roberts3, Sanjeev Verma4, Andrew Day3 and Shaun Ho1,2
1Royal Children's Hospital Melbourne, Parkville, Australia;2Murdoch Children Research Institute, Parkville, Australia;3University of Otago Christchurch, Christchurch, New Zealand;4King George Medical University, Lucknow, India
Background and Aim: The 2012 and 2020 ESPGHAN guidelines for the diagnosis of coeliac disease (CD) in children included a non-biopsy approach for children meeting specific criteria; ≥10 times the upper limit of normal anti-tissue transglutaminase IgA antibody, positive endomysial IgA antibody, +/- positive coeliac HLA haplotypes (HLA). The aim of the study was to perform a meta-analysis of the overall CD diagnostic accuracy using the ESPGHAN non-biopsy criteria in children who also had small bowel biopsy (SBB) confirmation as the reference standard.
Methods: Database searches (Medline, Embase, Web of Science, Scopus) were done in October 2023 and studies underwent stages of exclusion if they did not adhere to the ESPGHAN criteria and have SBB confirmation. A random effects meta-analysis provided a pooled positive predictive value (PPV) for all studies, sub-group analysis was carried out to identify sources of heterogeneity.
Results: Searches identified 1053 articles, with 21 included in the final analysis. While study sample sizes ranged from 39 to 707 with a total of 4087, 2323 children fulfilled the ESPGHAN non-biopsy criteria and of these 2289 had comparative SBB and were included in the final meta-analysis. The proportion of CD cases diagnosed using the ESPGHAN non-biopsy approach compared to SBB ranged from 79.2-100% in studies, with an overall pooled PPV of 97.3% (CI 95.4,98.6) [Figure 1]. Between study heterogeneity was high (I2 79.2%, p<0.0001, CI 68.8,86.1), explored using sub-group analysis that showed higher PPV for studies using prospective methodologies (p=0.001). Sensitivity analysis showed that PPV was higher in studies applying the ESPGHAN criteria that included positive HLA, versus the criteria without HLA (PPV 98.5 vs 96.7, p=0.014).
55
Collagenous gastritis in children: response to oral budesonide
Jay Sharma and Ryan Joseph Anson and Ajay Sharma
University Of Western Australia, Perth, Australia
Background and Aim: Collagenous gastritis(CG) is a rare disease in children characterized by the subepithelial deposition of collagen bands and inflammatory infiltrates in the gastric lamina propria with no effective treatment described to date. We aim to describe the outcomes of 3 patients with a 3 months course of oral Budesonide that will contribute to improved therapeutic options for this rare condition.
Methods: A retrospective chart review (0-18 years) in the last 10 years was reviewed (2013-2023) with a total of 3 cases of CG identified.
Results:
Case 1: A 15-year-old female presented with significant anaemia with haemoglobin of 71 g/L (NR-125-175 g/L) with ferritin < 5 ug/L (NR 20-200 ug/L). Esophagogastroduodenoscopy revealed CG in histology. She was started on a 3-month course of Oral Budesonide 9 mg, 6 mg and 3 mg with a repeat Hb and ferritin levels remaining in the normal range.
Case 2: A 17-year-old male was referred with anaemia despite trialling PPI and oral iron. EGD confirmed CG and on daily 3 months of Budesonide with a similar regimen as Case 1, had stable Iron levels and Hb.
Case 3: A 15 yo presented with fatigue (Hb 57 g/dl) and failed trial of PPI and oral iron. EGD confirmed CG and a similar regimen was followed as case 1 with Ferritin and Hb staying in the normal range after 3 months.
Conclusions: This case series demonstrates considering trialling a 3-month weaning course of Budesonide if Oral iron therapy and PPI trial fail and it could be an effective therapeutic option for the CG patients though it's unclear whether this regimen could be considered a safe long-term option. Further research is needed to understand the Pathophysiology and treatment target.
148
An automated approach to the analysis of paediatric high-resolution colonic manometry data: characterisation of the meal response in children with Hirschsprung disease using a Bayesian functional mixed effects model
Hannah Evans-Barns1,2,3, Lukasz Wiklendt6, John Hutson2,3,4, Warwick Teague1,2,3, Mark Safe5, Sebastian King1,2,3 and Phil Dinning6
1Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Australia;2Surgical Research Group, Murdoch Children's Research Institute, Melbourne, Australia;3Department of Paediatrics, University of Melbourne, Melbourne, Australia;4Department of Urology, The Royal Children’s Hospital, Melbourne, Australia;5Department of Gastroenterology and Clinical Nutrition, The Royal Children’s Hospital, Melbourne, Australia;6Gastroenterology Department, Flinders Medical Centre, Bedford Park, Australia
Background and Aim: Post-operative bowel dysfunction is prevalent in children with Hirschsprung disease (HD). The aim of this study was to characterise the colonic meal response, recorded by high-resolution manometry (HRCM), using a Bayesian functional mixed effects model, and compare findings to healthy controls.
Methods: A HRCM catheter was positioned in the colon with sensors spanning the caecum to rectum. A one hour baseline recording was followed by a meal challenge and a further one hour recording. The control group consisted of 13 healthy adults. Cross-wavelet analysis was used to compute the frequency and direction of all propagating pressure waves (PPW). A latent Gaussian Process model was used compare the effects of the meal on PPW within, and between, patients and controls. Ethical approval was obtained (HREC 64192).
Results: A meal was eaten by 13 children (12 male; 6.83±2.56 years; 9/13 short-segment). In the proximal colon, while the meal induced a significant increase both antegrade and retrograde PPW across a range of frequencies (1/16 to 8 cycles per minute [cpm]), the effect was significantly reduced in HD (Figure). In the distal colon of controls, the meal induced a significant increase in all PPWs between 1/16 – 8 cpm. In HD, the meal did not increase PPW between 2-10cpm.
152
Crossed wires: aligning clinical practice with family experiences in paediatric temporary tube feeding
1The University Of Queensland, Brisbane, Australia;2Children's Health Queensland, Brisbane, Australia;3Queensland University of Technology, Brisbane, Australia
Background and Aim: Temporary tube feeding is crucial for children requiring short-term nutritional support, yet its impact on families is under-researched. This study aimed to compare the perspectives of families of children with temporary feeding tubes with the clinicians who managed them, with the goal of enhancing understanding, improving clinical practice and investigating the children’s quality of life.
Methods: This study, part of a larger mixed-methods research project at a major children’s hospital, collected data from families of children discharged home with a temporary feeding tube (e.g., nasogastric tube) using electronic diaries and semi-structured interviews. Medical records were reviewed, and quality of life was assessed using the Pediatric Quality of Life Inventory version 4.0 Generic Core Scales (PEDsQL) at key time points (tube insertion, midpoint, removal). Clinicians completed an online survey.
Results: This study included 37 children with temporary feeding tubes, and 112 clinicians (medical practitioners, nursing, and allied health) overseeing their care. Communication gaps were prevalent: whilst 95% (n=35) of families were informed about the tube’s necessity, only 12% (n=4) recalled being told about the expected duration, despite 44% (n=49) of clinicians describing having this conversation. The medical notes revealed that only one child had a tube exit plan, despite 28 clinicians reporting completing this. Importantly, 32% (n=35) of clinicians were unable to recall whether estimated tube feeding duration was ever discussed. Additionally, whilst 61% (n=68) of clinicians provided written information about the feeding tube, 16% (n=18) were unable to recall whether or not they did. Seven children received feeding tubes despite documented parental objections in their medical notes. Preliminary quality of life results indicated a mean PEDS-QL score of 53.2 (SD±15.9) at tube insertion, 61.5 (SD±16.9) at midpoint, and 65.8 (SD±19.3) at the endpoint. These scores are lower than those reported in healthy children (83.9; SD±12.5), and lower when compared to studies of children with other health conditions.
Conclusion: This study revealed substantial disparities in clinical decision-making and communication regarding temporary feeding tubes. These children experienced lower reported quality of life compared to their healthy peers and those with other health conditions. There is a discrepancy between the care clinicians believe they provide and what families retain. This study recommends improved guidelines for communication, education, and documentation to better align clinical practices with family needs, ensuring better outcomes for this group of children.
306
Proactive therapeutic drug monitoring (TDM) of infliximab leads to durability of treatment in children with inflammatory bowel disease
Cher Wei Chuah1 and Shoma Dutt1,2
1Department Of Gastroenterology, The Children's Hospital At Westmead, Westmead, Australia;2CHW Clinical School University of Sydney, Westmead, Australia
Background and Aim: Anti-tumour Necrosis Factor therapies are the only biological therapy approved on the pharmaceutical benefits scheme (PBS) for children in Australia. Loss of response to the 1st biological predicts poorer responses to subsequent biologicals1. Maintaining and preserving response is beneficial in the paediatric age group. Published literature suggest that one third of patients will develop secondary loss of response (LOR) by the first year and up to 50% of initial responders will develop LOR by 5 years.2 Evidence suggest sustained high trough levels increases the durability of infliximab. The ability to recapture response in secondary LOR with dose escalation is well described.3 In 2019, our unit opted for proactive TDM (at week 6, week 14 and 6 monthly thereafter) and dose escalation based on cutoffs at week 6 < 15 μg/mL, week 14/maintenance < 5 μg/mL as standard practice, in addition to the usual practice of escalation guided by the clinical picture.4 We report the outcomes of our patient cohort over a period of 2 years from initiation of infliximab.
Methods: A retrospective chart review of patients commenced on infliximab was performed between 01/01/2019 to 31/12/2021. Only patients who completed induction were included, patients with acute severe colitis were excluded from this report as they were escalated on different parameters and will be reported separately. Data on demographics, disease characteristics, immunomodifier usage, infliximab dosing and frequency, infliximab drug levels, and antibody levels and switching to alternative biologics were collected and analysed. A physician global assessment (PGA) scale of remission, mild, moderate, and severe was used to assess clinical outcomes. Standard infliximab dosing is 5mg/kg at 0, 2, 6 weeks for induction and every 8 weeks during maintenance phase. Escalation was defined as either shortening of standard interval and/or increased dose to 10mg/kg.
Results: 98 patients (58% male) were identified, 82% had Crohn’s disease (CD) and 18% Ulcerative Colitis (UC). Median age at diagnosis was 11 years old, and 12.5 years old at starting infliximab. 81% received an immune modifier of which 64% had methotrexate and 39% azathioprine. 13% received escalated induction and 77% escalated maintenance. 3% failed to achieve remission and were discontinued. 2% developed infliximab antibodies. 8% of patients were switched to an alternate biologic by 1 year and 18% by 2 years, median time to switch was 53 weeks. Of those that remained on infliximab, 83% were in clinical remission at 1 year and 94% at 2 years. Switching to alternate biologic was associated with escalated induction, OR 5.8 (1.5 – 22.5, p = 0.01) UC, OR 5.6 (1.8 – 17.5, p < 0.01) and concomitant steroid use, OR 4.1 (1.1-15.5, p = 0.04). Immunomodulator use was not associated with switching biologics (p = 0.84). No patients on escalated induction developed antibodies (p = 0.58) and 1 patient on escalated maintenance developed antibodies (p = 0.48). There was no significance difference with standard or escalated maintenance with the PGA at the 1-year (p = 0.14) and 2 –year mark (p = 0.49).
Conclusion: Proactive TDM and escalation of infliximab results in good durability with treatment persistence at 92% at 1 year and 82% at 2 year and an excellent clinical remission rate of 94% at 2 years. Escalated induction and UC were predictors to switch biologics which is in keeping with primary non-responders/severe phenotype. Vahabnezhad et al reports in their series of paediatric CD also treated with escalated infliximab had treatment persistence of 80% at 2 years.3 Our CD cohort had 88% who remain on infliximab at 2 years. This study provides real world evidence that the subset of patients that responds well to infliximab can be maintained on this therapy longer than what is in the current published literature and merit that escalated therapy is funded by the PBS.
References
1. Gisbert, J. P., & Chaparro, M. (2020). Predictors of Primary Response to Biologic Treatment [Anti-TNF, Vedolizumab, and Ustekinumab] in Patients With Inflammatory Bowel Disease: From Basic Science to Clinical Practice. Journal of Crohn's & colitis, 14(5), 694–709. https://doi.org/10.1093/ecco-jcc/jjz195
2. Ding, N. S., Hart, A., & De Cruz, P. (2016). Systematic review: predicting and optimising response to anti-TNF therapy in Crohn's disease - algorithm for practical management. Alimentary pharmacology & therapeutics, 43(1), 30–51. https://doi.org/10.1111/apt.13445
3. Vahabnezhad, E., Rabizadeh, S., & Dubinsky, M. C. (2014). A 10-year, single tertiary care center experience on the durability of infliximab in pediatric inflammatory bowel disease. Inflammatory bowel diseases, 20(4), 606–613. https://doi.org/10.1097/MIB.0000000000000003
4. Rheenen, P. F., Aloi, M., Assa, A., et al. (2020). The Medical Management of Paediatric Crohn's Disease: an ECCO-ESPGHAN Guideline Update. Journal of Crohn's & colitis, jjaa161. Advance online publication. https://doi.org/10.1093/ecco-jcc/jjaa161
350
Changes in paediatric inflammatory bowel disease care at a paediatric tertiary hospital from 2014 to 2021
Jessica Nguyen1, Joan Cheng2 and Edward Giles3,4
1Department of Paediatric Gastroenterology, Monash Children's Hospital, Monash Health, Clayton, Australia;2Faculty of Medicine, Nursing and Health Sciences, Monash University, Clayton, Australia;3Department of Paediatrics, Monash University, Clayton, Australia;4Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Clayton, Australia
Background and Aim: The recent Paediatric Inflammatory Bowel Disease (PIBD) quality of care project investigated the care of children with IBD in Australia in 2021. This included a national audit of patient care that was almost directly comparable to the IBD audit from 2014. This provided an opportunity for all hospitals that were involved in both audits to examine how their care had changed.
Methods: Organisational data (including total admissions, staffing etc) from our paediatric tertiary hospital from 2014 to 2021 were compared. In addition, inpatient admissions data was audited from patients with ulcerative colitis (UC) and Crohn’s disease admitted. Statistical analysis was performed using Chi-Square test (Prism software).
Results: From 2014 to 2021, we had similar number of Crohn’s disease admissions (15 in 2014, 14 in 2021); however, double the number of UC admissions (12 in 2014, 24 in 2021, See figure 1) The most common length of stay was between 3-6 days for both Crohn’s and UC. In 2021, a smaller percentage of Crohn’s patients had a previous admission (78% in 2014 down to 43%, p<0.0001). In UC patients, a higher percentage of patients had a previous admission (25% up to 48%, p=0.0007). In 2021, there were more patients with anaemia (64% in 2021 compared to 33% in 2014 in Crohn’s disease, p<0.0001; 60% in 2021 compared to 25% in 2014 in UC, p<0.0001) and malnutrition on admission (6 compared to 2 with Crohn’s disease, p=0.0015; 4 compared to 1 with UC, p=0.1649).
362
A population-based study of the prevalence and metabolic significance of steatotic liver disease in children and their parents
1Fiona Stanley Hospital, Murdoch, Australia;2The University of Western Australia, Perth, Australia;3Curtin University, Bentley, Australia;4NursePrac Australia, Success, Australia;5Murdoch University, Murdoch, Australia;6Healthway, Perth, Australia;7Joondalup Hospital, Joondalup, Australia;8University of New South Wales, Sydney, Australia;9Oceania University of Medicine, Brisbane, Australia
Background and Aims: Steatotic liver disease (SLD) is the most common chronic liver disorder globally. SLD in childhood reflects prevalent metabolic dysfunction in children and families and poses increased longer-term risk of early-onset cardiometabolic and liver-related complications. We examined the prevalence and metabolic significance of SLD in children and their parents.
Method: Population-based children, aged 5-15 years, and their parents participated in a cross-sectional observational study of SLD in Perth, Australia. Assessments included anthropometry (weight, height, waist circumference and skinfold thickness [SFT]) and blood tests. Utilising Fibroscan® we non-invasively examined the severity of hepatic steatosis using controlled attenuation parameter (CAP), and severity of liver fibrosis using transient elastography (TE)-measured liver stiffness measurement (LSM). SLD was defined by CAP ≥249 dB/m in children and ≥275 in parents. Children aged 5-10 years were considered as young children and those aged 11-15 years as older children. SLD in children was considered to be metabolic dysfunction-associated SLD (MASLD). We compared cardiometabolic characteristics of children with versus those without MASLD, and sought associations between MASLD in children and parent characteristics.
Results: One hundred and fifteen children (50% male), with mean [SD] age 9.6[2.7] years, 74 mothers aged 40.7[5.8] years and 24 fathers aged 44.2[5.8] participated in the study. One child did not have FibroScan® assessment. Seventy-three children (64%) were young children. Compared with older children, young children had lower body weight, height and waist circumference (p<0.05), but skinfold thickness, CAP, LSM, serum lipids, leptin, high sensitivity C-reactive protein (hsCRP) and liver enzyme levels were not significantly different (p>0.05 for all). Comparing boys vs. girls, there were no significant differences in anthropometric measures of adiposity or CAP overall (p>0.05 for all). Mean (SD) WC was 88.3(13.4) cm in mothers and 91.8 (10.9) cm in fathers. Mean BMI was 27.7 (5.3) kg/m2 in mothers and 27.3 (3.0) kg/m2 in fathers. SLD was diagnosed in 20.2% children (15.8% male vs. 24.6% female, p=0.24), 29.9% mothers and 37.5% fathers. SLD was seen in 55% of children with BMI ≥30 kg/m2. Children with MASLD had greater subcutaneous fat measured as SFT, serum alanine aminotransferase (ALT), leptin, hsCRP, and triglycerides, and lower levels of high-density lipoprotein cholesterol, compared with those without SLD (p<0.05 for all, Table 1). CAP in children was positively correlated with BMI z-score, waist circumference, skinfold thickness, weight, ALT, gamma glutamyl transpeptidase (GGT), triglycerides, leptin, and maternal and paternal BMI (p<0.05 for all). There was no significant correlation between SLD in children and their parents, however mothers of children with SLD had higher mean BMI than mothers of children without SLD (30.3[5.7] kg/m2 vs. 27.1[5.1] kg/m2, p=0.04), and fathers had higher mean liver stiffness measurement (LSM), (7.6[4.6] kPa vs. 4.8[1.2] kPa, p=0.02. Using multivariable logistic regression analysis, child ALT (OR 1.21, 95% CI 1.01-1.45) and abdominal SFT (OR 1.59, 95% CI 1.03-2.44) were associated with SLD in children, after adjusting for child WC (OR 0.94, 95% CI 0.87-1.04), and maternal BMI (OR 1.22, 95% CI 0.85-1.76).
Conclusion: MASLD is common in children, and is associated with increased adiposity, raised ALT, features of metabolic dysfunction, maternal adiposity, and paternal liver stiffness. Our findings suggest intergenerational heritability of metabolic and hepatic risk.
471
Similar outcomes following early proactive vs reactive therapeutic drug monitoring in children with Crohn’s disease commencing infliximab – a single centre, retrospective study
Asha Jois1, Rachel Horn1, Anysha Walia1, Eric Cheah2, Robert Little3 and George Alex1,4
1Royal Children's Hospital, Parkville, Australia;2Monash Children's Hospital, Clayton, Australia;3Alfred Health, Melbourne, Australia;4University of Melbourne, Parkville, Australia
Background and Aim: Benefits of a proactive compared to a reactive therapeutic drug monitoring (TDM) strategy when commencing infliximab (IFX) for management of Crohn’s disease are unclear. We evaluated the 6- and 12-month outcomes in children commencing IFX with proactive week 14 TDM compared to those without week 14 TDM.
Methods: Single-centre, retrospective study of Crohn’s disease patients aged 0-18 years with a primary response to IFX induction between 2018-2021. Proactive TDM was defined by measurement of a week 14 IFX drug level and reactive TDM was defined by no week 14 drug level. Baseline patient, medication and disease characteristics were compared across the two groups. Clinical and biochemical disease activity measures, and IFX dose, frequency and drug level were compared across the two groups at week 0, 6- and 12-months post-induction. Failure was defined by biologic switch, corticosteroid use, hospitalisation or surgery.
Results: We included 86 patients. 34/86 (40%) were female, diagnosed at median 13 years, with a median disease duration of 4 years. 40/86 (47%) had proactive TDM – baseline characteristics by group are presented in Table 1. At 12-months, there was no difference in failure rates (15% vs. 23%, p = 0.419) or IFX persistence (95% vs. 89%, p = 0.442) between the proactive and reactive TDM groups, respectively. At 6-months, the proactive group had more escalated IFX dose frequency (23% vs. 5%, p = 0.023), but IFX dose was comparable (5.8 vs. 5.5 mg/kg, p = 0.108). There was no difference in IFX drug level or disease severity at either 6- or 12-months.
Conclusion: In children with Crohn’s disease commenced on IFX, week 14 proactive TDM was not associated with improved outcomes at 12-months compared to children without week 14 TDM, and IFX drug levels were comparable. Prospective studies are required to identify the optimal TDM strategy.
480
Subcutaneous infliximab use in children with inflammatory bowel disease in a tertiary paediatric hospital
Jessica A Eldredge1, Cher Wei Chuah1, Michelle Tano1, Trudy Chidgey, Noel Singh1,2, Kunal Thacker1, Annabel Magoffin1 and Shoma Dutt1 and Edward O'Loughlin1
1Department of Gastroenterology, Children's Hospital at Westmead, Australia;2Pharmacy Department, Children's Hospital at Westmead, Australia
Background and Aim: Anti-Tumour Necrosis Factor (anti-TNF) therapies remain the only biological treatment accessible for use in Australian children with moderate to severe inflammatory bowel disease (IBD) via the Pharmaceutical Benefits Scheme. SC infliximab is now well-established in adult IBD care (1-3). Compared to traditional IV formulations, SC dosage may offer relative pharmacokinetic stability with sustained drug delivery, with comparable efficacy, safety and immunogenicity profiles (1-3). Published literature demonstrates that in younger IBD patients, the majority would prefer to switch to subcutaneous (SC) versions of their current intravenous (IV) biologic (1,2). Scarce real-world data is available on use of SC infliximab in paediatric IBD, with only seven children described from a single-centre cohort study in Edinburgh (4). We aimed to assess the clinical efficacy, tolerability and cost-benefit of SC infliximab, as part of an initiative supported by our local institutional Medicines and Therapeutics Committee.
Methods: We report twelve children with IBD who commenced 120mg fortnightly SC infliximab dosing between February to May 2024. Baseline, 4, 8 and 12 week follow-up biochemical and clinical assessments were undertaken over this treatment period. Nine of twelve children were male, with median age 14.5 years [range 6-17 years]. Eleven had a diagnosis of Crohn’s disease. Two children received SC infliximab as the third dose in their induction therapy and ongoing. Ten children were transitioned from stable infliximab IV maintenance dosing. All were prescribed concomitant immunomodulator therapy (azathioprine or methotrexate).
Results: Clinical and biochemical parameters for children treated with subcutaneous infliximab are outlined in Table 1. Clinical disease activity indices (Paediatric Crohn’s Disease Activity Index [PCDAI] or Paediatric Ulcerative Colitis Activity Index [PUCAI]) were stable or improved over the treatment period. Median baseline infliximab level prior to first SC dose was 9.2 mg/L [IQR 7.1 – 11.0] with calprotectin 53.5ug/g [IQR 20-334]. Infliximab level increased by a median of 9.3mg/L [IQR 0.7-12.3], and calprotectin reduced by median 32ug/g [IQR -92.5-35.5] over the 12 week follow-up period. No significant adverse events were observed. Combined cost of escalated non-PBS infliximab intravenous dosing, day medical unit admission and consumables saved was estimated at $12,304.92 per patient per annum in this group.
Conclusion: Calprotectin and clinical disease activity indices were stable or on average improved following twelve weeks of SC infliximab dosing in twelve children with IBD. We propose subcutaneous infliximab may be an efficacious and cost-saving treatment alternative to IV dosing in children with IBD, reducing healthcare costs (admissions for IV infusions), and financial and educational impacts on patients and families (lost work and school days). Further data in larger cohorts of children is required, including quality-of-life and cost-saving assessment scales.
References
1. Buisson, A, Nachury, M, Reymond, M et al. Effectiveness of Switching From Intravenous to Subcutaneous Infliximab in Patients With Inflammatory Bowel Diseases: the REMSWITCH Study. Clin Gastroenterol Hepatol2023; 21: 2338-46.e3.
2. Schreiber, S, Ben-Horin, S, Leszczyszyn, J et al. Randomized Controlled Trial: Subcutaneous vs Intravenous Infliximab CT-P13 Maintenance in Inflammatory Bowel Disease. Gastroenterology2021; 160: 2340-53.
3. Strik, AS, Vrie, W, Bloemsaat-Minekus, JPJ et al. Serum concentrations after switching from originator infliximab to the biosimilar CT-P13 in patients with quiescent inflammatory bowel disease (SECURE): an open-label, multicentre, phase 4 non-inferiority trial. Lancet Gastroenterol Hepatol2018; 3: 404-12.
4. Gianolio, L, Armstrong, K, Swann, E et al. Effectiveness of Switching to Subcutaneous Infliximab in Pediatric Inflammatory Bowel Disease Patients on Intravenous Maintenance Therapy. J Pediatr Gastroenterol Nutr.2023; 77(2): 235-239. https://doi.org/10.1097/MPG.0000000000003838.
481
An Australian paediatric experience using orodispersible budesonide in eosinophilic oesophagitis
Juliet Affum1, Geoff Withers1, Alberto Pinzon-Charry2,3,4 and Looi Ee1
1Department of Gastroenterology, Hepatology & Liver Transplant, Queensland Children's Hospital, Brisbane, Australia;2Queensland Paediatric Immunology & Allergy Service, Queensland Children's Hospital, Brisbane, Australia;3The University of Queensland, Brisbane, Australia;4Griffith University, Gold Coast, Australia
Background and Aim: Eosinophilic oesophagitis (EoE) is an atopic and debilitating condition which has emerged in the last three decades with limited treatment options. Targeted therapies were not available in Australia until recently. On 1st May 2022, Jorveza®, a budesonide orodispersible tablet was listed on the Pharmaceutical Benefits Scheme (PBS) specifically for treating EoE. Our aim was to review the paediatric experience in our centre with this therapy.
Methods: Retrospective review of patients in a tertiary paediatric hospital who commenced this therapy between 1st May 2022 and 7th August 2023 was undertaken. Patient demographics, endoscopic appearance and histologic findings were recorded. Histologic remission was defined using two thresholds, <5 eos/hpf (PBS criteria) and ≤15 eos/hpf (standard criteria).
Results: Sixty-three patients, 87% (55/63) male, median age 14 (range 8-17) years were treated during this period. Thirty-five (56%) had a gastroscopy within 3 months of starting Jorveza® while the rest were “grandfathered” as they were already on swallowed topical steroids. Only 10 patients were newly diagnosed and thus, treatment naïve. Eighty-seven percent (55/63) had repeat gastroscopy at median 3.7 (range 2.1-13.7) months after staring Jorveza®. Remission was achieved in 49.09% (≤15 eos/hpf, standard criteria) and 41.82% (<5 eos/hpf, PBS criteria) respectively. Female gender and medication adherence were significantly associated with remission. Post treatment oesophageal eosinophil count was lower in compliant patients compared to those with suboptimal medication adherence, mean 21 vs 79 eos/hpf, p=0.006. There was a trend to higher oesophageal eosinophil counts with longer duration between Jorveza® commencement and repeat endoscopy in both responders and non-responders, but this did not reach statistical significance.
Conclusion: Jorveza® is an effective treatment for inducing histologic remission in children with EoE but is affected by compliance. Gender and medication adherence are significantly associated with histologic remission.
493
Percutaneous liver biopsy in children: comparison of complication rates between coaxial and noncoaxial techniques
Sudarshan Arvind1 and Murthy Chennapragada1,2
1The University of Sydney, Camperdown, Australia;2The Children's Hospital Westmead, Westmead, Australia
Background and Aim: Ultrasound guided percutaneous liver biopsy (PLB) is crucial in diagnosis and monitoring of paediatric liver disease. Two major techniques are used; coaxial (C-PLB) and non-coaxial (NC-PLB). C-PLB uses an outer needle sheath that penetrates the liver capsule, enabling a smaller biopsy needle to pass into the liver parenchyma. NC-PLB does not use an outer sheath, requiring more transgressions of the liver capsule to obtain the same number of cores of liver tissue. There is limited literature directly comparing complication rates following these techniques in children. The aim of this paper is to compare the incidence of complications following ultrasound-guided C-PLB and NC-PLB in children.
Methods: This is a single-centre retrospective cohort study conducted at The Children’s Hospital Westmead (New South Wales). We studied paediatric patients who underwent ultrasound-guided PLB between September 2016 and December 2019. Patients were divided into C-PLB (n= 227) and NC-PLB (n= 47). Electronic medical records were used to gather demographic data, baseline characteristics, clinical indication and post-procedural complications (stratified into major or minor according to the Society of Interventional Radiology classification system). Chi-square analysis was used to compare demographic and baseline characteristics and to determine if there was a significant difference in the incidence of complications between these groups.
Results: A total of 274 paediatric patients underwent ultrasound-guided PLB between September 2016 and December 2019. 227 underwent C-PLB (83%) while 47 underwent NC-PLB (17%). 51.5% of all PLB recipients were female. Biliary atresia (34.7%) was the most common primary diagnosis, followed by autoimmune hepatitis (8.4%). Coagulopathy or thrombocytopaenia (6.2%) was the most common pre-biopsy comorbidity. There were no major complications encountered across either cohort. Total incidence of minor complications was 17.9%. Minor complications occurred in 16.7% of the C-PLB cohort compared to 23.4% in the NC-PLB cohort. The difference was not significant (p=0.278). There was a significantly lower incidence of asymptomatic bleeding (p=0.002) in the C-PLB cohort compared to the NC-PLB cohort.
Conclusion: Our findings do not suggest a significant difference in the incidence of complications following ultrasound-guided C-PLB vs. NC-PLB, with the exception of bleeding which occurs less frequently after C-PLB. Overall, this is a safe procedure when performed in a dedicated Radiology suite by experienced Interventional Radiologists, with no major complications encountered across 274 procedures over a 4-year period. Larger, prospective randomised control trials are required to further investigate the comparative risk of post-procedural complications.
561
Inflammatory Bowel Disease Paediatric Quality of Care Hospital Audit 2023 in Australia
Mia Komesaroff1, Laura Rishanghan1, Stephan Moller2, David Skvarc3, George Alex4, Christopher Burgess5, Ramesh Nataraja1, Antonia Mikocka-Walus3, Wayne Massuger6 and Edward Giles1,6
1Gastroenterology, Monash Health, Melbourne, Australia;2Crohn's and Colitis Australia, Melbourne, Australia;3Deakin University, Adelaide, Australia;4Gastroenterology, Royal Children's Hospital, Melboune, Australia;5Gastroenterology, Queensland Children's Hospital, Brisbane, Australia;6Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Melbourne, Australia
Background and Aim: Inflammatory bowel disease is a chronic, lifelong gastrointestinal disorder, with 8-10% patients diagnosed before 18 years old. The quality of care for these young people can be variable and a previous 2016 hospital audit showed Australian hospital did not meet the specified standards. The objectives of this study were to re-look at organisation, resources and delivery of hospital care to young people with IBD and identify changes since 2016.
Methods: This audit was conducted in collaboration with the patient organisation Crohn’s & Colitis Australia. Hospitals nationally were invited to participate in an online survey looking at organisation and resources of care, as well as a clinical audit of inpatient overnight admissions for 2021. Eight hospitals participated looking at 186 admissions, which captured 23% of public hospital admissions for IBD patients in 2021.
Results: We found there was limited access to multidisciplinary care, with only 23% of CD inpatients being seen by and IBD nurse, compared to 33% in 2014. Despite psychological comorbidity in 28% of cases, psychologists were not part of the team at any site. The use of preventive anti-thrombotic reduced to 10% in 2021, from 30% in 2014 (p<0.001) despite new clinical guidelines supporting use. Of note, sites reported new, off label IBD medications were used in 56 young people. UC surgical admissions reduced to 5% in 2021 from 16% in 2014 (p>0.05). This occurred despite increased in UC admissions overall (almost doubled nationally). The use of corticosteroids for than 3 months in the year prior to admission reduced from 1% to 10% in 2014.
Conclusions: This audit helped build recommendations including increased support for multidisciplinary team, improved mental health support and streamline access to newer medication.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
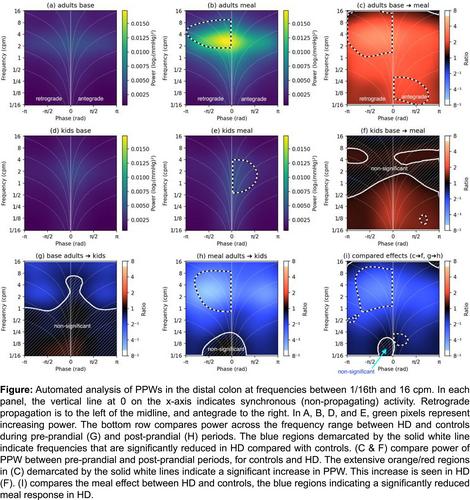



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
