Clara Rollet, Camille Le Ray, Françoise Vendittelli, Béatrice Blondel, Anne Alice Chantry, the MDN Research Group
{"title":"根据助产士主导的分娩中心或产科主导的分娩单位的计划分娩环境,孕产妇和新生儿的严重不良后果","authors":"Clara Rollet, Camille Le Ray, Françoise Vendittelli, Béatrice Blondel, Anne Alice Chantry, the MDN Research Group","doi":"10.1111/aogs.14971","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The establishment of midwife-led birth centers (MLBCs) is still being debated. The study aimed to compare severe adverse outcomes and mode of birth in low-risk women according to their birth planned in MLBCs or in obstetric-led units (OUs) in France.</p>\n </section>\n \n <section>\n \n <h3> Material and Methods</h3>\n \n <p>We used nationwide databases to select low-risk women at the start of care in labor in MLBCs (<i>n</i> = 1294) and in OUs (<i>n</i> = 5985). Using multilevel logistic regression, we compared severe adverse maternal and neonatal morbidity as a composite outcome and as individual outcomes. These include severe postpartum hemorrhage (≥1000 mL of blood loss), obstetrical anal sphincter injury, maternal admission to an intensive care unit, maternal death, a 5-minute Apgar score <7, neonatal resuscitation at birth, neonatal admission to an intensive care unit, and stillbirth or neonatal death. We also studied the mode of birth and the role of prophylactic administration of oxytocin at birth in the association between birth settings and severe postpartum hemorrhage.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Severe adverse maternal and neonatal outcome indicated a slightly higher rate in women in MLBCs compared to OUs according to unadjusted analyses (4.6% in MLBCs vs. 3.4% in OUs; cOR 1.36; 95%CI [1.01–1.83]), but the difference was not significant between birth settings after adjustment (aOR 1.37 [0.92–2.05]). Severe neonatal morbidity alone was not different (1.7% vs. 1.6%; aOR 1.17 [0.55–2.47]). However, severe maternal morbidity was significantly higher in MLBCs than in OUs (3.0% vs. 1.9%; aOR 1.61 [1.09–2.39]), mainly explained by higher risks of severe postpartum hemorrhage (2.4 vs. 1.1%; aOR 2.37 [1.29–4.36]), with 2 out of 5 in MLBCs partly explained by the low use of prophylactic oxytocin. Cesarean and operative vaginal births were significantly decreased in women with a birth planned in MLBCs.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>In France, 3 to 4% of low-risk women experienced a severe adverse maternal or neonatal outcome regardless of the planned birth setting. Results were favorable for MLBCs in terms of mode of birth but not for severe postpartum hemorrhage, which could be partly addressed by revising practices of prophylactic administration of oxytocin.</p>\n </section>\n </div>","PeriodicalId":6990,"journal":{"name":"Acta Obstetricia et Gynecologica Scandinavica","volume":"103 12","pages":"2465-2474"},"PeriodicalIF":3.5000,"publicationDate":"2024-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aogs.14971","citationCount":"0","resultStr":"{\"title\":\"Severe adverse maternal and neonatal outcomes according to the planned birth setting being midwife-led birth centers or obstetric-led units\",\"authors\":\"Clara Rollet, Camille Le Ray, Françoise Vendittelli, Béatrice Blondel, Anne Alice Chantry, the MDN Research Group\",\"doi\":\"10.1111/aogs.14971\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>The establishment of midwife-led birth centers (MLBCs) is still being debated. The study aimed to compare severe adverse outcomes and mode of birth in low-risk women according to their birth planned in MLBCs or in obstetric-led units (OUs) in France.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Material and Methods</h3>\\n \\n <p>We used nationwide databases to select low-risk women at the start of care in labor in MLBCs (<i>n</i> = 1294) and in OUs (<i>n</i> = 5985). Using multilevel logistic regression, we compared severe adverse maternal and neonatal morbidity as a composite outcome and as individual outcomes. These include severe postpartum hemorrhage (≥1000 mL of blood loss), obstetrical anal sphincter injury, maternal admission to an intensive care unit, maternal death, a 5-minute Apgar score <7, neonatal resuscitation at birth, neonatal admission to an intensive care unit, and stillbirth or neonatal death. We also studied the mode of birth and the role of prophylactic administration of oxytocin at birth in the association between birth settings and severe postpartum hemorrhage.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Severe adverse maternal and neonatal outcome indicated a slightly higher rate in women in MLBCs compared to OUs according to unadjusted analyses (4.6% in MLBCs vs. 3.4% in OUs; cOR 1.36; 95%CI [1.01–1.83]), but the difference was not significant between birth settings after adjustment (aOR 1.37 [0.92–2.05]). Severe neonatal morbidity alone was not different (1.7% vs. 1.6%; aOR 1.17 [0.55–2.47]). However, severe maternal morbidity was significantly higher in MLBCs than in OUs (3.0% vs. 1.9%; aOR 1.61 [1.09–2.39]), mainly explained by higher risks of severe postpartum hemorrhage (2.4 vs. 1.1%; aOR 2.37 [1.29–4.36]), with 2 out of 5 in MLBCs partly explained by the low use of prophylactic oxytocin. Cesarean and operative vaginal births were significantly decreased in women with a birth planned in MLBCs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>In France, 3 to 4% of low-risk women experienced a severe adverse maternal or neonatal outcome regardless of the planned birth setting. Results were favorable for MLBCs in terms of mode of birth but not for severe postpartum hemorrhage, which could be partly addressed by revising practices of prophylactic administration of oxytocin.</p>\\n </section>\\n </div>\",\"PeriodicalId\":6990,\"journal\":{\"name\":\"Acta Obstetricia et Gynecologica Scandinavica\",\"volume\":\"103 12\",\"pages\":\"2465-2474\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aogs.14971\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Obstetricia et Gynecologica Scandinavica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/aogs.14971\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Obstetricia et Gynecologica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/aogs.14971","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Severe adverse maternal and neonatal outcomes according to the planned birth setting being midwife-led birth centers or obstetric-led units
Introduction
The establishment of midwife-led birth centers (MLBCs) is still being debated. The study aimed to compare severe adverse outcomes and mode of birth in low-risk women according to their birth planned in MLBCs or in obstetric-led units (OUs) in France.
Material and Methods
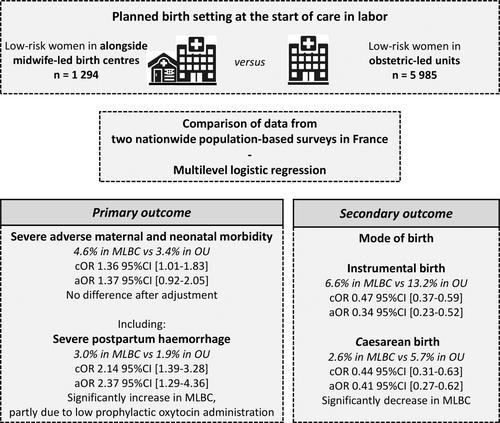
We used nationwide databases to select low-risk women at the start of care in labor in MLBCs (n = 1294) and in OUs (n = 5985). Using multilevel logistic regression, we compared severe adverse maternal and neonatal morbidity as a composite outcome and as individual outcomes. These include severe postpartum hemorrhage (≥1000 mL of blood loss), obstetrical anal sphincter injury, maternal admission to an intensive care unit, maternal death, a 5-minute Apgar score <7, neonatal resuscitation at birth, neonatal admission to an intensive care unit, and stillbirth or neonatal death. We also studied the mode of birth and the role of prophylactic administration of oxytocin at birth in the association between birth settings and severe postpartum hemorrhage.
Results
Severe adverse maternal and neonatal outcome indicated a slightly higher rate in women in MLBCs compared to OUs according to unadjusted analyses (4.6% in MLBCs vs. 3.4% in OUs; cOR 1.36; 95%CI [1.01–1.83]), but the difference was not significant between birth settings after adjustment (aOR 1.37 [0.92–2.05]). Severe neonatal morbidity alone was not different (1.7% vs. 1.6%; aOR 1.17 [0.55–2.47]). However, severe maternal morbidity was significantly higher in MLBCs than in OUs (3.0% vs. 1.9%; aOR 1.61 [1.09–2.39]), mainly explained by higher risks of severe postpartum hemorrhage (2.4 vs. 1.1%; aOR 2.37 [1.29–4.36]), with 2 out of 5 in MLBCs partly explained by the low use of prophylactic oxytocin. Cesarean and operative vaginal births were significantly decreased in women with a birth planned in MLBCs.
Conclusions
In France, 3 to 4% of low-risk women experienced a severe adverse maternal or neonatal outcome regardless of the planned birth setting. Results were favorable for MLBCs in terms of mode of birth but not for severe postpartum hemorrhage, which could be partly addressed by revising practices of prophylactic administration of oxytocin.
期刊介绍:
Published monthly, Acta Obstetricia et Gynecologica Scandinavica is an international journal dedicated to providing the very latest information on the results of both clinical, basic and translational research work related to all aspects of women’s health from around the globe. The journal regularly publishes commentaries, reviews, and original articles on a wide variety of topics including: gynecology, pregnancy, birth, female urology, gynecologic oncology, fertility and reproductive biology.





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
