{"title":"隐匿性疝气伤人:呼吁早期诊断和治疗隐匿性腹股沟疝气","authors":"Harry J. Wong, Cherin Oh, Shirin Towfigh","doi":"10.1007/s00464-024-11253-4","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>Hidden or occult inguinal hernias are symptomatic hernias that do not present with a bulge. For some surgeons, if a bulge is not present, then no hernia repair is contemplated. We report preoperative findings of patients with occult inguinal hernias and outcomes after repair to assist in early detection and treatment of this special population.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>All patients who underwent inguinal hernia repairs, 2008–2019, were reviewed. Patients were classified as having occult inguinal hernias if they (a) complained of groin pain, (b) did not have bulging on exam, (c) had supportive imaging showing an inguinal hernia, and (d) were confirmed to have inguinal hernias that were repaired intraoperatively. Presentation and outcomes were compared with the non-occult group treated during the same time period.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Of 485 patients who underwent elective inguinal hernia repairs over 10 years, 212 (44%) had occult inguinal hernias. Patients in the occult group were significantly more likely to be female, younger, and with higher BMI compared to the non-occult group. They also had more preoperative pain for a significantly longer time. This was associated with higher incidence of pain medications usage, including opioids, in the occult group. On physical examination, those with occult hernias were twice as likely to have tenderness over the inguinal canal. Most hernia repairs (66%) were laparoscopic and 94% used mesh. Postoperatively, the occult group had 83% resolution of symptoms after hernia repair.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Some surgeons hesitate recommending hernia repair to patients with occult inguinal hernias, as these patients do not fit the traditional definition of a hernia, i.e., a bulge. Our study challenges this perception by showing that discounting groin pain due to occult hernia prolongs patient’s suffering and may risk increased opioid use, especially in females, although 83% cure can be achieved with hernia repair.</p><h3 data-test=\"abstract-sub-heading\">Graphical abstract</h3>\n","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"9 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Hidden hernias hurt: a plea for early diagnosis and treatment of occult inguinal hernias\",\"authors\":\"Harry J. Wong, Cherin Oh, Shirin Towfigh\",\"doi\":\"10.1007/s00464-024-11253-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Introduction</h3><p>Hidden or occult inguinal hernias are symptomatic hernias that do not present with a bulge. For some surgeons, if a bulge is not present, then no hernia repair is contemplated. We report preoperative findings of patients with occult inguinal hernias and outcomes after repair to assist in early detection and treatment of this special population.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>All patients who underwent inguinal hernia repairs, 2008–2019, were reviewed. Patients were classified as having occult inguinal hernias if they (a) complained of groin pain, (b) did not have bulging on exam, (c) had supportive imaging showing an inguinal hernia, and (d) were confirmed to have inguinal hernias that were repaired intraoperatively. Presentation and outcomes were compared with the non-occult group treated during the same time period.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>Of 485 patients who underwent elective inguinal hernia repairs over 10 years, 212 (44%) had occult inguinal hernias. Patients in the occult group were significantly more likely to be female, younger, and with higher BMI compared to the non-occult group. They also had more preoperative pain for a significantly longer time. This was associated with higher incidence of pain medications usage, including opioids, in the occult group. On physical examination, those with occult hernias were twice as likely to have tenderness over the inguinal canal. Most hernia repairs (66%) were laparoscopic and 94% used mesh. Postoperatively, the occult group had 83% resolution of symptoms after hernia repair.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>Some surgeons hesitate recommending hernia repair to patients with occult inguinal hernias, as these patients do not fit the traditional definition of a hernia, i.e., a bulge. Our study challenges this perception by showing that discounting groin pain due to occult hernia prolongs patient’s suffering and may risk increased opioid use, especially in females, although 83% cure can be achieved with hernia repair.</p><h3 data-test=\\\"abstract-sub-heading\\\">Graphical abstract</h3>\\n\",\"PeriodicalId\":501625,\"journal\":{\"name\":\"Surgical Endoscopy\",\"volume\":\"9 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Endoscopy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s00464-024-11253-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-11253-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Hidden hernias hurt: a plea for early diagnosis and treatment of occult inguinal hernias
Introduction
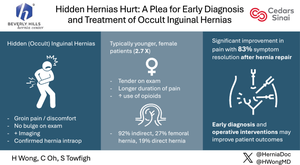
Hidden or occult inguinal hernias are symptomatic hernias that do not present with a bulge. For some surgeons, if a bulge is not present, then no hernia repair is contemplated. We report preoperative findings of patients with occult inguinal hernias and outcomes after repair to assist in early detection and treatment of this special population.
Methods
All patients who underwent inguinal hernia repairs, 2008–2019, were reviewed. Patients were classified as having occult inguinal hernias if they (a) complained of groin pain, (b) did not have bulging on exam, (c) had supportive imaging showing an inguinal hernia, and (d) were confirmed to have inguinal hernias that were repaired intraoperatively. Presentation and outcomes were compared with the non-occult group treated during the same time period.
Results
Of 485 patients who underwent elective inguinal hernia repairs over 10 years, 212 (44%) had occult inguinal hernias. Patients in the occult group were significantly more likely to be female, younger, and with higher BMI compared to the non-occult group. They also had more preoperative pain for a significantly longer time. This was associated with higher incidence of pain medications usage, including opioids, in the occult group. On physical examination, those with occult hernias were twice as likely to have tenderness over the inguinal canal. Most hernia repairs (66%) were laparoscopic and 94% used mesh. Postoperatively, the occult group had 83% resolution of symptoms after hernia repair.
Conclusion
Some surgeons hesitate recommending hernia repair to patients with occult inguinal hernias, as these patients do not fit the traditional definition of a hernia, i.e., a bulge. Our study challenges this perception by showing that discounting groin pain due to occult hernia prolongs patient’s suffering and may risk increased opioid use, especially in females, although 83% cure can be achieved with hernia repair.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
