Emma Vanderschueren , Youri Bekhuis , Jan Clerick , Jappe Decock , Philippe Meersseman , Alexander Wilmer , Eveline Claus , Lawrence Bonne , Guido Claessen , Chris Verslype , Geert Maleux , Wim Laleman
{"title":"图卢兹算法只识别因难治性腹水而接受 TIPS 治疗的患者中心脏失代偿风险增加的患者。","authors":"Emma Vanderschueren , Youri Bekhuis , Jan Clerick , Jappe Decock , Philippe Meersseman , Alexander Wilmer , Eveline Claus , Lawrence Bonne , Guido Claessen , Chris Verslype , Geert Maleux , Wim Laleman","doi":"10.1016/j.aohep.2024.101568","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction and Objectives</h3><div>TIPS placement is an effective, possibly life-saving, treatment for complications of portal hypertension. The pressure shift induced by the stent can lead to cardiac decompensation (CD). We investigated the incidence of CD, possible variables associated with CD and the validity of the Toulouse algorithm for risk prediction of CD post-TIPS.</div></div><div><h3>Patients and Methods</h3><div>A total of 106 patients receiving TIPS for variceal bleeding (VB, 41.5%) or refractory ascites (RA, 58.5%) with available echocardiography and NT-proBNP results were included and retrospectively reviewed. Development of CD between time of TIPS placement and occurrence of liver transplantation, death or loss-to-follow-up was recorded. Competing risk regression analysis was performed to assess which baseline variables predicted occurrence of CD post-TIPS.</div></div><div><h3>Results</h3><div>A total of 12 patients (11.3%) developed CD after a median of 11.5 days (IQR 4 to 56.5) post-TIPS. Multivariate regression showed age (HR 1.06, <em>p</em> = 0.019), albumin (HR 1.10, <em>p</em> = 0.009) and NT-proBNP (HR 1.00, <em>p</em> = 0.023) at baseline predicted CD in the RA group. No clear predictors were found in those receiving TIPS for VB. Correspondingly, the Toulouse algorithm successfully identified patients at risk for CD, however only in the RA population (zero risk 0% vs. low risk 12.5% vs. high risk 35.3% with CD; <em>p</em> = 0.003).</div></div><div><h3>Conclusions</h3><div>CD is not an infrequent complication post-TIPS occurring in 1/10 patients. The Toulouse algorithm can identify patients at risk of CD, though only in patients receiving TIPS for RA. Allocation to the high-risk category warrants close monitoring but should not preclude TIPS placement.</div></div>","PeriodicalId":7979,"journal":{"name":"Annals of hepatology","volume":"30 1","pages":"Article 101568"},"PeriodicalIF":4.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"The Toulouse algorithm identifies patients with increased risk of cardiac decompensation only in patients with TIPS for refractory ascites\",\"authors\":\"Emma Vanderschueren , Youri Bekhuis , Jan Clerick , Jappe Decock , Philippe Meersseman , Alexander Wilmer , Eveline Claus , Lawrence Bonne , Guido Claessen , Chris Verslype , Geert Maleux , Wim Laleman\",\"doi\":\"10.1016/j.aohep.2024.101568\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Introduction and Objectives</h3><div>TIPS placement is an effective, possibly life-saving, treatment for complications of portal hypertension. The pressure shift induced by the stent can lead to cardiac decompensation (CD). We investigated the incidence of CD, possible variables associated with CD and the validity of the Toulouse algorithm for risk prediction of CD post-TIPS.</div></div><div><h3>Patients and Methods</h3><div>A total of 106 patients receiving TIPS for variceal bleeding (VB, 41.5%) or refractory ascites (RA, 58.5%) with available echocardiography and NT-proBNP results were included and retrospectively reviewed. Development of CD between time of TIPS placement and occurrence of liver transplantation, death or loss-to-follow-up was recorded. Competing risk regression analysis was performed to assess which baseline variables predicted occurrence of CD post-TIPS.</div></div><div><h3>Results</h3><div>A total of 12 patients (11.3%) developed CD after a median of 11.5 days (IQR 4 to 56.5) post-TIPS. Multivariate regression showed age (HR 1.06, <em>p</em> = 0.019), albumin (HR 1.10, <em>p</em> = 0.009) and NT-proBNP (HR 1.00, <em>p</em> = 0.023) at baseline predicted CD in the RA group. No clear predictors were found in those receiving TIPS for VB. Correspondingly, the Toulouse algorithm successfully identified patients at risk for CD, however only in the RA population (zero risk 0% vs. low risk 12.5% vs. high risk 35.3% with CD; <em>p</em> = 0.003).</div></div><div><h3>Conclusions</h3><div>CD is not an infrequent complication post-TIPS occurring in 1/10 patients. The Toulouse algorithm can identify patients at risk of CD, though only in patients receiving TIPS for RA. Allocation to the high-risk category warrants close monitoring but should not preclude TIPS placement.</div></div>\",\"PeriodicalId\":7979,\"journal\":{\"name\":\"Annals of hepatology\",\"volume\":\"30 1\",\"pages\":\"Article 101568\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S166526812400351X\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepatology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S166526812400351X","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
导言和目的:TIPS 置入术是治疗门静脉高压并发症的有效方法,也可能是挽救生命的方法。支架引起的压力转移可导致心脏失代偿(CD)。我们调查了 CD 的发生率、与 CD 相关的可能变量以及 TIPS 术后 CD 风险预测图卢兹算法的有效性:共纳入 106 名因静脉曲张出血(VB,41.5%)或难治性腹水(RA,58.5%)而接受 TIPS 的患者,并对其超声心动图和 NT-proBNP 结果进行回顾性分析。记录了从放置 TIPS 到发生肝移植、死亡或失去随访期间 CD 的发展情况。进行了竞争风险回归分析,以评估哪些基线变量可预测TIPS术后CD的发生:共有12名患者(11.3%)在TIPS术后中位11.5天(IQR为4-56.5)后出现CD。多变量回归显示,年龄(HR 1.06,p = 0.019)、白蛋白(HR 1.10,p = 0.009)和基线时的 NT-proBNP(HR 1.00,p = 0.023)可预测 RA 组的 CD。在因 VB 而接受 TIPS 的患者中未发现明确的预测因素。相应地,图卢兹算法成功识别了CD风险患者,但仅限于RA人群(零风险0% vs. 低风险12.5% vs. 高风险35.3%有CD;p = 0.003):结论:CD并非TIPS术后的罕见并发症,1/10的患者会出现CD。图卢兹算法可以识别有 CD 风险的患者,但仅限于接受 TIPS 治疗的 RA 患者。被归入高风险类别的患者需要密切监测,但不应排除 TIPS 置入。
The Toulouse algorithm identifies patients with increased risk of cardiac decompensation only in patients with TIPS for refractory ascites
Introduction and Objectives
TIPS placement is an effective, possibly life-saving, treatment for complications of portal hypertension. The pressure shift induced by the stent can lead to cardiac decompensation (CD). We investigated the incidence of CD, possible variables associated with CD and the validity of the Toulouse algorithm for risk prediction of CD post-TIPS.
Patients and Methods
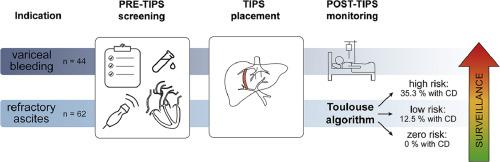
A total of 106 patients receiving TIPS for variceal bleeding (VB, 41.5%) or refractory ascites (RA, 58.5%) with available echocardiography and NT-proBNP results were included and retrospectively reviewed. Development of CD between time of TIPS placement and occurrence of liver transplantation, death or loss-to-follow-up was recorded. Competing risk regression analysis was performed to assess which baseline variables predicted occurrence of CD post-TIPS.
Results
A total of 12 patients (11.3%) developed CD after a median of 11.5 days (IQR 4 to 56.5) post-TIPS. Multivariate regression showed age (HR 1.06, p = 0.019), albumin (HR 1.10, p = 0.009) and NT-proBNP (HR 1.00, p = 0.023) at baseline predicted CD in the RA group. No clear predictors were found in those receiving TIPS for VB. Correspondingly, the Toulouse algorithm successfully identified patients at risk for CD, however only in the RA population (zero risk 0% vs. low risk 12.5% vs. high risk 35.3% with CD; p = 0.003).
Conclusions
CD is not an infrequent complication post-TIPS occurring in 1/10 patients. The Toulouse algorithm can identify patients at risk of CD, though only in patients receiving TIPS for RA. Allocation to the high-risk category warrants close monitoring but should not preclude TIPS placement.
期刊介绍:
Annals of Hepatology publishes original research on the biology and diseases of the liver in both humans and experimental models. Contributions may be submitted as regular articles. The journal also publishes concise reviews of both basic and clinical topics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
