Peter Z Du, Gurmit Singh, Spencer Smith, Travis Philipp, Jonathan Kark, Clifford Lin, Jung U Yoo
{"title":"器械脊柱融合术后骶髂关节融合的风险因素。","authors":"Peter Z Du, Gurmit Singh, Spencer Smith, Travis Philipp, Jonathan Kark, Clifford Lin, Jung U Yoo","doi":"10.1177/21925682241286458","DOIUrl":null,"url":null,"abstract":"<p><p>Study DesignRetrospective Cohort Study.ObjectiveTo identify risk factors for sacroiliac (SI) joint fusion after instrumented spinal fusion.MethodsPatients were identified from the PearlDiver BiscayneBay database. Patients who underwent 1 level (CPT: 22840), 3-6 vertebral segment (22842), and 7+ vertebral segment spinal fusions (22843 and 22844) were identified. Patients were separated based on whether they received an SI joint fusion (27280 and 27279) after their spinal fusion. A univariate analysis and multivariate logistic regression was performed to evaluate the associations between patient factors and incidence of SI joint fusion.Results549,625 patients who underwent posterior spinal fusions were identified, 6068 of whom underwent subsequent SI joint fusion (1.1%). Factors associated with future SI joint fusion included female gender, patients with obesity, fibromyalgia, diabetes, tobacco use, increased construct length, and prior SI joint injection. Prior SI joint injection had the highest odds ratio (OR: 8.70; 95% CI: 8.25-9.16; <i>P</i> < 0.001), followed by 7+ vertebral segment (OR: 2.17; 95% CI: 2.03-2.33; <i>P</i> < 0.001) and 3-6 vertebral segment fusion (OR: 1.49; 95% CI: 1.42-1.57; <i>P</i> < 0.001).ConclusionsThe highest predictor of requiring subsequent SI joint fusion is a prior SI joint injection. We also found that longer fusion constructs are associated with increased risk for future SI joint fusion.</p>","PeriodicalId":12680,"journal":{"name":"Global Spine Journal","volume":" ","pages":"2096-2101"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11559710/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors for Sacroiliac Joint Fusion after Instrumented Spinal Fusion.\",\"authors\":\"Peter Z Du, Gurmit Singh, Spencer Smith, Travis Philipp, Jonathan Kark, Clifford Lin, Jung U Yoo\",\"doi\":\"10.1177/21925682241286458\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Study DesignRetrospective Cohort Study.ObjectiveTo identify risk factors for sacroiliac (SI) joint fusion after instrumented spinal fusion.MethodsPatients were identified from the PearlDiver BiscayneBay database. Patients who underwent 1 level (CPT: 22840), 3-6 vertebral segment (22842), and 7+ vertebral segment spinal fusions (22843 and 22844) were identified. Patients were separated based on whether they received an SI joint fusion (27280 and 27279) after their spinal fusion. A univariate analysis and multivariate logistic regression was performed to evaluate the associations between patient factors and incidence of SI joint fusion.Results549,625 patients who underwent posterior spinal fusions were identified, 6068 of whom underwent subsequent SI joint fusion (1.1%). Factors associated with future SI joint fusion included female gender, patients with obesity, fibromyalgia, diabetes, tobacco use, increased construct length, and prior SI joint injection. Prior SI joint injection had the highest odds ratio (OR: 8.70; 95% CI: 8.25-9.16; <i>P</i> < 0.001), followed by 7+ vertebral segment (OR: 2.17; 95% CI: 2.03-2.33; <i>P</i> < 0.001) and 3-6 vertebral segment fusion (OR: 1.49; 95% CI: 1.42-1.57; <i>P</i> < 0.001).ConclusionsThe highest predictor of requiring subsequent SI joint fusion is a prior SI joint injection. We also found that longer fusion constructs are associated with increased risk for future SI joint fusion.</p>\",\"PeriodicalId\":12680,\"journal\":{\"name\":\"Global Spine Journal\",\"volume\":\" \",\"pages\":\"2096-2101\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11559710/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Spine Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/21925682241286458\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Spine Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21925682241286458","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
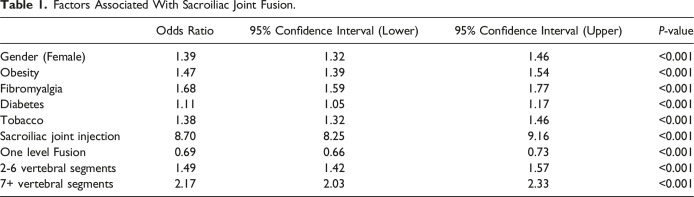
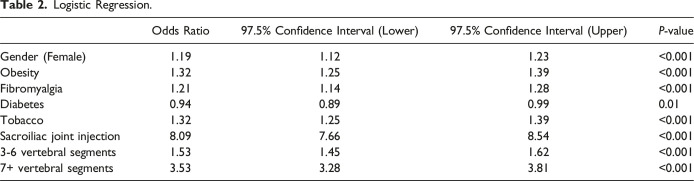
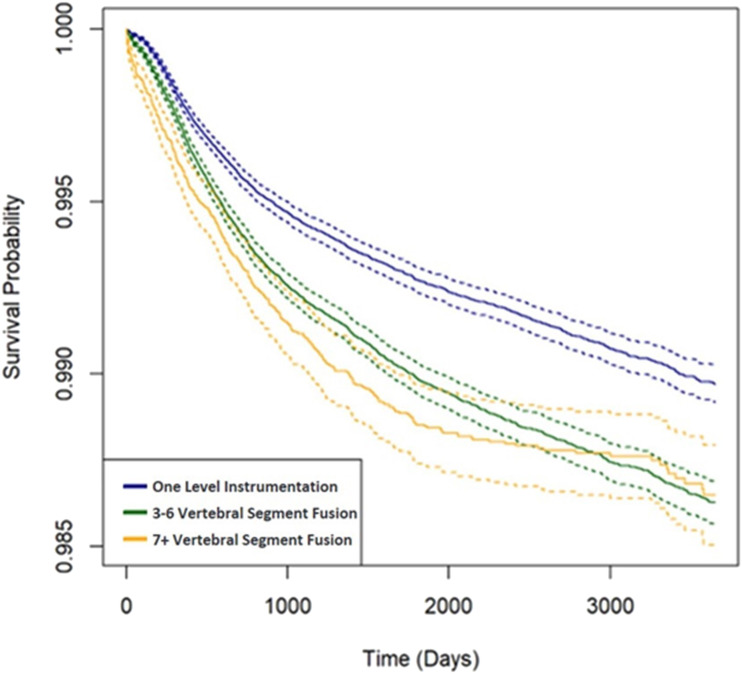
研究设计回顾性队列研究:确定器械脊柱融合术后骶髂关节(SI)融合的风险因素:从PearlDiver BiscayneBay数据库中识别患者。确定了接受 1 级(CPT:22840)、3-6 椎节(22842)和 7+ 椎节脊柱融合术(22843 和 22844)的患者。根据患者在脊柱融合术后是否接受了 SI 关节融合术(27280 和 27279)将其分开。通过单变量分析和多变量逻辑回归来评估患者因素与 SI 关节融合术发生率之间的关系:结果:共发现了 549,625 名接受脊柱后路融合术的患者,其中 6068 人随后接受了 SI 关节融合术(1.1%)。与未来SI关节融合术相关的因素包括:女性、肥胖、纤维肌痛、糖尿病、吸烟、构造长度增加以及曾接受过SI关节注射。曾进行SI关节注射的几率比最高(OR:8.70;95% CI:8.25-9.16;P<0.001),其次是7+椎节(OR:2.17;95% CI:2.03-2.33;P<0.001)和3-6椎节融合(OR:1.49;95% CI:1.42-1.57;P<0.001):结论:预测后续 SI 关节融合需要的最高指标是之前的 SI 关节注射。我们还发现,较长的融合结构与未来 SI 关节融合的风险增加有关。
Risk Factors for Sacroiliac Joint Fusion after Instrumented Spinal Fusion.
Study DesignRetrospective Cohort Study.ObjectiveTo identify risk factors for sacroiliac (SI) joint fusion after instrumented spinal fusion.MethodsPatients were identified from the PearlDiver BiscayneBay database. Patients who underwent 1 level (CPT: 22840), 3-6 vertebral segment (22842), and 7+ vertebral segment spinal fusions (22843 and 22844) were identified. Patients were separated based on whether they received an SI joint fusion (27280 and 27279) after their spinal fusion. A univariate analysis and multivariate logistic regression was performed to evaluate the associations between patient factors and incidence of SI joint fusion.Results549,625 patients who underwent posterior spinal fusions were identified, 6068 of whom underwent subsequent SI joint fusion (1.1%). Factors associated with future SI joint fusion included female gender, patients with obesity, fibromyalgia, diabetes, tobacco use, increased construct length, and prior SI joint injection. Prior SI joint injection had the highest odds ratio (OR: 8.70; 95% CI: 8.25-9.16; P < 0.001), followed by 7+ vertebral segment (OR: 2.17; 95% CI: 2.03-2.33; P < 0.001) and 3-6 vertebral segment fusion (OR: 1.49; 95% CI: 1.42-1.57; P < 0.001).ConclusionsThe highest predictor of requiring subsequent SI joint fusion is a prior SI joint injection. We also found that longer fusion constructs are associated with increased risk for future SI joint fusion.
期刊介绍:
Global Spine Journal (GSJ) is the official scientific publication of AOSpine. A peer-reviewed, open access journal, devoted to the study and treatment of spinal disorders, including diagnosis, operative and non-operative treatment options, surgical techniques, and emerging research and clinical developments.GSJ is indexed in PubMedCentral, SCOPUS, and Emerging Sources Citation Index (ESCI).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
