Xiaowen Han, Xiaodong Huang, Jiayi Zhang, Weidong Li, Zhen Ma, Bin Ma, Ewestse Paul Maswikiti, Zhenyu Yin, Yuhan Wang, Lei Gao, Hao Chen
{"title":"病例报告:直肠癌患者接受系统靶向治疗后出现坏死性筋膜炎是否与肿瘤部位有关?- 来自一名肝癌患者的证据。","authors":"Xiaowen Han, Xiaodong Huang, Jiayi Zhang, Weidong Li, Zhen Ma, Bin Ma, Ewestse Paul Maswikiti, Zhenyu Yin, Yuhan Wang, Lei Gao, Hao Chen","doi":"10.1186/s13027-024-00607-1","DOIUrl":null,"url":null,"abstract":"<p><p>Necrotizing fasciitis (NF) is a rare and life-threatening serious infectious disease, characterized by acute onset and rapid progress, leading to extensive necrosis of skin, soft tissue as well as fascia by a variety of aerobic and anaerobic bacteria, localized on external genitalia, scrotum, groin and perianal areas in males. There exist numerous common etiologies for NF, yet NF induced by malignant neoplasms is exceedingly rare. Several studies have reported that NF may be associated with tumor site (rectal/sigmoid colon cancer) and blood supply dysfunction caused by targeted therapy drugs (bevacizumab, aflibercept, ramucirumab). The perforation of colorectal cancer poses a unique risk factor for NF. However, in our two cases, the patient with rectal cancer received CapeOX (oxaliplatin + capecitabine) + bevacizumab + tislelizumab for 3 cycles without perforation but did develop NF. One month after debridement, the patient continued immunotherapy with tislelizumab alone for the fourth cycle and maintained for an additional 3 cycles without any recurrence of NF. Therefore, does the occurrence of NF correlate with the tumor site (rectum) and targeted immunotherapy? Another patient with hepatocellular carcinoma also developed NF after receiving 2 cycles of lenvatinib + sintilimab treatment. The third cycle of sintilimab immunotherapy was administered on the 13th day after operation, which was subsequently maintained for an additional 2 cycles without recurrence of NF. The absence of a direct correlation between hepatocellular carcinoma and rectal tumor location as well as immunotherapy, suggests that NF may be closely linked to targeted therapy.</p>","PeriodicalId":13568,"journal":{"name":"Infectious Agents and Cancer","volume":"19 1","pages":"45"},"PeriodicalIF":2.8000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11414244/pdf/","citationCount":"0","resultStr":"{\"title\":\"Case report: is necrotizing fasciitis in a rectal cancer patient after targeted systemic therapy related to the tumor site? - evidence from a hepatocellular carcinoma patient.\",\"authors\":\"Xiaowen Han, Xiaodong Huang, Jiayi Zhang, Weidong Li, Zhen Ma, Bin Ma, Ewestse Paul Maswikiti, Zhenyu Yin, Yuhan Wang, Lei Gao, Hao Chen\",\"doi\":\"10.1186/s13027-024-00607-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Necrotizing fasciitis (NF) is a rare and life-threatening serious infectious disease, characterized by acute onset and rapid progress, leading to extensive necrosis of skin, soft tissue as well as fascia by a variety of aerobic and anaerobic bacteria, localized on external genitalia, scrotum, groin and perianal areas in males. There exist numerous common etiologies for NF, yet NF induced by malignant neoplasms is exceedingly rare. Several studies have reported that NF may be associated with tumor site (rectal/sigmoid colon cancer) and blood supply dysfunction caused by targeted therapy drugs (bevacizumab, aflibercept, ramucirumab). The perforation of colorectal cancer poses a unique risk factor for NF. However, in our two cases, the patient with rectal cancer received CapeOX (oxaliplatin + capecitabine) + bevacizumab + tislelizumab for 3 cycles without perforation but did develop NF. One month after debridement, the patient continued immunotherapy with tislelizumab alone for the fourth cycle and maintained for an additional 3 cycles without any recurrence of NF. Therefore, does the occurrence of NF correlate with the tumor site (rectum) and targeted immunotherapy? Another patient with hepatocellular carcinoma also developed NF after receiving 2 cycles of lenvatinib + sintilimab treatment. The third cycle of sintilimab immunotherapy was administered on the 13th day after operation, which was subsequently maintained for an additional 2 cycles without recurrence of NF. The absence of a direct correlation between hepatocellular carcinoma and rectal tumor location as well as immunotherapy, suggests that NF may be closely linked to targeted therapy.</p>\",\"PeriodicalId\":13568,\"journal\":{\"name\":\"Infectious Agents and Cancer\",\"volume\":\"19 1\",\"pages\":\"45\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11414244/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Agents and Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13027-024-00607-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Agents and Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13027-024-00607-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Case report: is necrotizing fasciitis in a rectal cancer patient after targeted systemic therapy related to the tumor site? - evidence from a hepatocellular carcinoma patient.
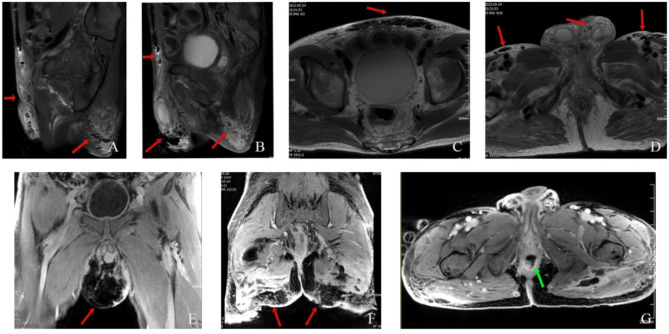
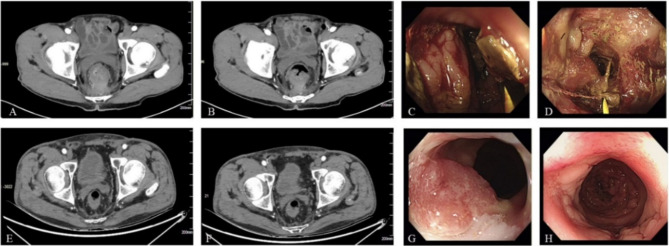
Necrotizing fasciitis (NF) is a rare and life-threatening serious infectious disease, characterized by acute onset and rapid progress, leading to extensive necrosis of skin, soft tissue as well as fascia by a variety of aerobic and anaerobic bacteria, localized on external genitalia, scrotum, groin and perianal areas in males. There exist numerous common etiologies for NF, yet NF induced by malignant neoplasms is exceedingly rare. Several studies have reported that NF may be associated with tumor site (rectal/sigmoid colon cancer) and blood supply dysfunction caused by targeted therapy drugs (bevacizumab, aflibercept, ramucirumab). The perforation of colorectal cancer poses a unique risk factor for NF. However, in our two cases, the patient with rectal cancer received CapeOX (oxaliplatin + capecitabine) + bevacizumab + tislelizumab for 3 cycles without perforation but did develop NF. One month after debridement, the patient continued immunotherapy with tislelizumab alone for the fourth cycle and maintained for an additional 3 cycles without any recurrence of NF. Therefore, does the occurrence of NF correlate with the tumor site (rectum) and targeted immunotherapy? Another patient with hepatocellular carcinoma also developed NF after receiving 2 cycles of lenvatinib + sintilimab treatment. The third cycle of sintilimab immunotherapy was administered on the 13th day after operation, which was subsequently maintained for an additional 2 cycles without recurrence of NF. The absence of a direct correlation between hepatocellular carcinoma and rectal tumor location as well as immunotherapy, suggests that NF may be closely linked to targeted therapy.
期刊介绍:
Infectious Agents and Cancer is an open access, peer-reviewed online journal that encompasses all aspects of basic, clinical, epidemiological and translational research providing an insight into the association between chronic infections and cancer.
The journal welcomes submissions in the pathogen-related cancer areas and other related topics, in particular:
• HPV and anogenital cancers, as well as head and neck cancers;
• EBV and Burkitt lymphoma;
• HCV/HBV and hepatocellular carcinoma as well as lymphoproliferative diseases;
• HHV8 and Kaposi sarcoma;
• HTLV and leukemia;
• Cancers in Low- and Middle-income countries.
The link between infection and cancer has become well established over the past 50 years, and infection-associated cancer contribute up to 16% of cancers in developed countries and 33% in less developed countries.
Preventive vaccines have been developed for only two cancer-causing viruses, highlighting both the opportunity to prevent infection-associated cancers by vaccination and the gaps that remain before vaccines can be developed for other cancer-causing agents. These gaps are due to incomplete understanding of the basic biology, natural history, epidemiology of many of the pathogens that cause cancer, the mechanisms they exploit to cause cancer, and how to interrupt progression to cancer in human populations. Early diagnosis or identification of lesions at high risk of progression represent the current most critical research area of the field supported by recent advances in genomics and proteomics technologies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
