Caroline Wei Shan Hoong, Stephen M Broski, Jad G Sfeir, Bart Lyman Clarke
{"title":"正常钙血症甲状旁腺功能亢进症的自然病史和并发症:一项回顾性队列研究。","authors":"Caroline Wei Shan Hoong, Stephen M Broski, Jad G Sfeir, Bart Lyman Clarke","doi":"10.1093/jbmrpl/ziae074","DOIUrl":null,"url":null,"abstract":"<p><p>Normocalcemic hyperparathyroidism (NHPT) is variably defined, and information regarding complications and natural history are scarce. We aimed to describe the phenotype of NHPT in relation to hypercalcemic hyperparathyroidism (PHPT) and controls, to determine risk of progression, and to develop a predictive model for progression to PHPT. This is a retrospective chart review of 232 patients at a tertiary medical center, comparing 75 controls, 73 patients with NHPT, and 84 with PHPT. NHPT was intermediate in biochemical profile between controls and PHPT with respect to cCa, iPTH, intraindividual coefficient of variant of cCa, phosphorus, and 25(OH)D. NHPT patients had an increased adjusted risk of urolithiasis (OR 5.34, 95%CI, 2.41-12.71, <i>P</i> < .001) and fragility fractures (OR 4.53, 95%CI, 1.63-14.84, <i>P</i> = .006) versus controls, after adjustment for age, sex, and BMI. Fewer NHPT compared with PHPTH patients achieved cure with parathyroidectomy (<i>P</i> = .001). NHPT more often had nonlocalizing imaging or polyglandular disease (<i>P</i> = .005). Parathyroidectomy improved biochemical but not BMD parameters in NHPT. Over a median follow-up of 4.23 (IQR 1.76-5.31) years, NHPT patients managed expectantly experienced no change in iPTH, and progression to PHPT occurred in 9%. An XGBoost model combining 6 factors for progression (mean index 2 iPTH, mean index 2 cCa, 24-h urinary calcium, age, 25(OH)D, and presence of urolithiasis) had an area under the curve 1.00 (95%CI, 1.00-1.00, <i>P</i> < .001) for predicting combined progression. NHPT is a mild variant of PHPT at intermediate risk of urolithiasis and fragility fractures. Cure was less often achieved with parathyroidectomy, which did not improve BMD parameters. Progression was infrequent with conservative management. Because only a minority progressed to PHPT, in addition to lower surgical success rates, we suggest conservative management for the majority of NHPT unless risk factors for progression are identified.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 7","pages":"ziae074"},"PeriodicalIF":2.4000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11406159/pdf/","citationCount":"0","resultStr":"{\"title\":\"Natural history and complications of normocalcemic hyperparathyroidism: a retrospective cohort study.\",\"authors\":\"Caroline Wei Shan Hoong, Stephen M Broski, Jad G Sfeir, Bart Lyman Clarke\",\"doi\":\"10.1093/jbmrpl/ziae074\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Normocalcemic hyperparathyroidism (NHPT) is variably defined, and information regarding complications and natural history are scarce. We aimed to describe the phenotype of NHPT in relation to hypercalcemic hyperparathyroidism (PHPT) and controls, to determine risk of progression, and to develop a predictive model for progression to PHPT. This is a retrospective chart review of 232 patients at a tertiary medical center, comparing 75 controls, 73 patients with NHPT, and 84 with PHPT. NHPT was intermediate in biochemical profile between controls and PHPT with respect to cCa, iPTH, intraindividual coefficient of variant of cCa, phosphorus, and 25(OH)D. NHPT patients had an increased adjusted risk of urolithiasis (OR 5.34, 95%CI, 2.41-12.71, <i>P</i> < .001) and fragility fractures (OR 4.53, 95%CI, 1.63-14.84, <i>P</i> = .006) versus controls, after adjustment for age, sex, and BMI. Fewer NHPT compared with PHPTH patients achieved cure with parathyroidectomy (<i>P</i> = .001). NHPT more often had nonlocalizing imaging or polyglandular disease (<i>P</i> = .005). Parathyroidectomy improved biochemical but not BMD parameters in NHPT. Over a median follow-up of 4.23 (IQR 1.76-5.31) years, NHPT patients managed expectantly experienced no change in iPTH, and progression to PHPT occurred in 9%. An XGBoost model combining 6 factors for progression (mean index 2 iPTH, mean index 2 cCa, 24-h urinary calcium, age, 25(OH)D, and presence of urolithiasis) had an area under the curve 1.00 (95%CI, 1.00-1.00, <i>P</i> < .001) for predicting combined progression. NHPT is a mild variant of PHPT at intermediate risk of urolithiasis and fragility fractures. Cure was less often achieved with parathyroidectomy, which did not improve BMD parameters. Progression was infrequent with conservative management. Because only a minority progressed to PHPT, in addition to lower surgical success rates, we suggest conservative management for the majority of NHPT unless risk factors for progression are identified.</p>\",\"PeriodicalId\":14611,\"journal\":{\"name\":\"JBMR Plus\",\"volume\":\"8 7\",\"pages\":\"ziae074\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11406159/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBMR Plus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jbmrpl/ziae074\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Natural history and complications of normocalcemic hyperparathyroidism: a retrospective cohort study.
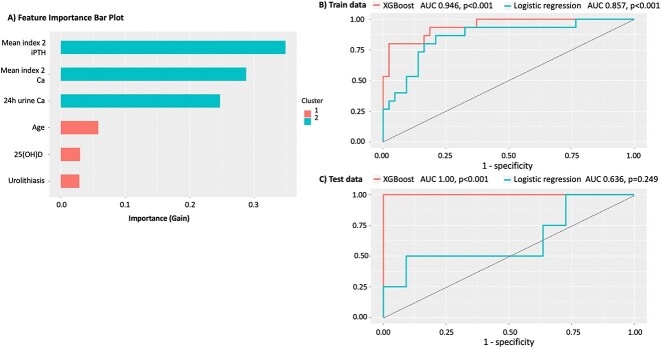
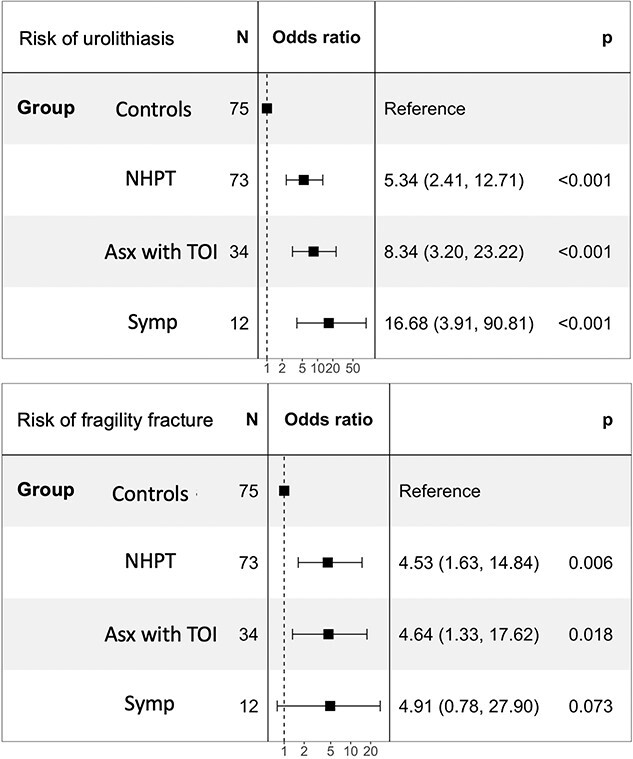
Normocalcemic hyperparathyroidism (NHPT) is variably defined, and information regarding complications and natural history are scarce. We aimed to describe the phenotype of NHPT in relation to hypercalcemic hyperparathyroidism (PHPT) and controls, to determine risk of progression, and to develop a predictive model for progression to PHPT. This is a retrospective chart review of 232 patients at a tertiary medical center, comparing 75 controls, 73 patients with NHPT, and 84 with PHPT. NHPT was intermediate in biochemical profile between controls and PHPT with respect to cCa, iPTH, intraindividual coefficient of variant of cCa, phosphorus, and 25(OH)D. NHPT patients had an increased adjusted risk of urolithiasis (OR 5.34, 95%CI, 2.41-12.71, P < .001) and fragility fractures (OR 4.53, 95%CI, 1.63-14.84, P = .006) versus controls, after adjustment for age, sex, and BMI. Fewer NHPT compared with PHPTH patients achieved cure with parathyroidectomy (P = .001). NHPT more often had nonlocalizing imaging or polyglandular disease (P = .005). Parathyroidectomy improved biochemical but not BMD parameters in NHPT. Over a median follow-up of 4.23 (IQR 1.76-5.31) years, NHPT patients managed expectantly experienced no change in iPTH, and progression to PHPT occurred in 9%. An XGBoost model combining 6 factors for progression (mean index 2 iPTH, mean index 2 cCa, 24-h urinary calcium, age, 25(OH)D, and presence of urolithiasis) had an area under the curve 1.00 (95%CI, 1.00-1.00, P < .001) for predicting combined progression. NHPT is a mild variant of PHPT at intermediate risk of urolithiasis and fragility fractures. Cure was less often achieved with parathyroidectomy, which did not improve BMD parameters. Progression was infrequent with conservative management. Because only a minority progressed to PHPT, in addition to lower surgical success rates, we suggest conservative management for the majority of NHPT unless risk factors for progression are identified.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
