{"title":"血清 25- 羟维生素 D 与勃起功能障碍之间没有双向关联:孟德尔随机化和遗传关联研究。","authors":"Xiang Liu, Longhua Luo, Cong Peng, Zixin Wang, Jiaming Zhou, Xiang Sun","doi":"10.1093/sexmed/qfae061","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The causal relationship between the level of serum 25-hydroxyvitamin D [25(OH)D] and the risk of erectile dysfunction (ED) is still unclear.</p><p><strong>Aim: </strong>We tried to determine the causal relationship between the level of serum 25(OH)D and ED risk.</p><p><strong>Methods: </strong>In this study, we used genome-wide association study data from the UK Biobank to analyse the relationship between serum 25(OH)D (as the exposure) and ED (as the outcome). Linkage disequilibrium score regression (LDSC) was used to assess the genetic correlation between 2 traits. The CAUSE (Causal Analysis using Summary Effect estimates) method and Mendelian randomization (MR) were employed to evaluate the bidirectional causal relationship. The MRlap method was utilized to assess the impact of sample overlap on the results. To assess potential heterogeneity and horizontal pleiotropy, we utilized methods such as MR-Egger, MR-PRESSO (Mendelian Randomization Pleiotropy Residual Sum and Outlier), weighted median, and others.</p><p><strong>Outcomes: </strong>The primary outcome was defined as self or physician-reported ED, or using oral ED medication, or a history of surgery related to ED.</p><p><strong>Results: </strong>The LDSC analysis did not reveal a significant genetic correlation between serum 25(OH)D and ED (r<sub>g</sub> = 0.2787, <i>P =</i> .3536). Additionally, the CAUSE (<i>P</i> value testing that the causal model is a better fit >.05) and MR analyses (odds ratio, 0.8951; 95% confidence interval, 0.7480-1.0710; <i>P =</i> .2260) did not support a causal relationship between 25(OH)D and ED, and our study did not detect any heterogeneity and pleiotropy.</p><p><strong>Clinical implications: </strong>This study provides evidence on whether vitamin D needs to be ingested to prevent or treat ED.</p><p><strong>Strengths and limitations: </strong>We used LDSC and MR to avoid bias. However, the population in this study was limited to European ancestry.</p><p><strong>Conclusion: </strong>No causal relationship was found between 25(OH)D and ED.</p>","PeriodicalId":21782,"journal":{"name":"Sexual Medicine","volume":"12 4","pages":"qfae061"},"PeriodicalIF":2.0000,"publicationDate":"2024-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411456/pdf/","citationCount":"0","resultStr":"{\"title\":\"No bidirectional association between serum 25-hydroxyvitamin D and erectile dysfunction: Mendelian randomization and genetic association studies.\",\"authors\":\"Xiang Liu, Longhua Luo, Cong Peng, Zixin Wang, Jiaming Zhou, Xiang Sun\",\"doi\":\"10.1093/sexmed/qfae061\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The causal relationship between the level of serum 25-hydroxyvitamin D [25(OH)D] and the risk of erectile dysfunction (ED) is still unclear.</p><p><strong>Aim: </strong>We tried to determine the causal relationship between the level of serum 25(OH)D and ED risk.</p><p><strong>Methods: </strong>In this study, we used genome-wide association study data from the UK Biobank to analyse the relationship between serum 25(OH)D (as the exposure) and ED (as the outcome). Linkage disequilibrium score regression (LDSC) was used to assess the genetic correlation between 2 traits. The CAUSE (Causal Analysis using Summary Effect estimates) method and Mendelian randomization (MR) were employed to evaluate the bidirectional causal relationship. The MRlap method was utilized to assess the impact of sample overlap on the results. To assess potential heterogeneity and horizontal pleiotropy, we utilized methods such as MR-Egger, MR-PRESSO (Mendelian Randomization Pleiotropy Residual Sum and Outlier), weighted median, and others.</p><p><strong>Outcomes: </strong>The primary outcome was defined as self or physician-reported ED, or using oral ED medication, or a history of surgery related to ED.</p><p><strong>Results: </strong>The LDSC analysis did not reveal a significant genetic correlation between serum 25(OH)D and ED (r<sub>g</sub> = 0.2787, <i>P =</i> .3536). Additionally, the CAUSE (<i>P</i> value testing that the causal model is a better fit >.05) and MR analyses (odds ratio, 0.8951; 95% confidence interval, 0.7480-1.0710; <i>P =</i> .2260) did not support a causal relationship between 25(OH)D and ED, and our study did not detect any heterogeneity and pleiotropy.</p><p><strong>Clinical implications: </strong>This study provides evidence on whether vitamin D needs to be ingested to prevent or treat ED.</p><p><strong>Strengths and limitations: </strong>We used LDSC and MR to avoid bias. However, the population in this study was limited to European ancestry.</p><p><strong>Conclusion: </strong>No causal relationship was found between 25(OH)D and ED.</p>\",\"PeriodicalId\":21782,\"journal\":{\"name\":\"Sexual Medicine\",\"volume\":\"12 4\",\"pages\":\"qfae061\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411456/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Sexual Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/sexmed/qfae061\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sexual Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/sexmed/qfae061","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:目的:我们试图确定血清25-羟基维生素D[25(OH)D]水平与勃起功能障碍(ED)风险之间的因果关系:在这项研究中,我们利用英国生物库(UK Biobank)的全基因组关联研究数据分析了血清 25(OH)D(作为暴露量)与 ED(作为结果)之间的关系。链接不平衡得分回归(LDSC)用于评估两个性状之间的遗传相关性。采用 CAUSE(使用摘要效应估计的因果分析)方法和孟德尔随机化(MR)来评估双向因果关系。MRlap 方法用于评估样本重叠对结果的影响。为了评估潜在的异质性和水平褶皱,我们采用了 MR-Egger、MR-PRESSO(孟德尔随机褶皱残差和离群值)、加权中位数等方法:主要结果定义为自我或医生报告的 ED,或使用口服 ED 药物,或与 ED 相关的手术史:LDSC分析未发现血清25(OH)D与ED之间存在显著的遗传相关性(rg = 0.2787,P = .3536)。此外,CAUSE分析(检验因果模型拟合度更高的P值>.05)和MR分析(几率比0.8951;95%置信区间0.7480-1.0710;P = .2260)也不支持25(OH)D与ED之间存在因果关系,而且我们的研究没有检测到任何异质性和多义性:本研究为预防或治疗 ED 是否需要摄入维生素 D 提供了证据:我们使用了LDSC和MR以避免偏倚。然而,本研究的人群仅限于欧洲血统:结论:25(OH)D与ED之间没有因果关系。
No bidirectional association between serum 25-hydroxyvitamin D and erectile dysfunction: Mendelian randomization and genetic association studies.
Background: The causal relationship between the level of serum 25-hydroxyvitamin D [25(OH)D] and the risk of erectile dysfunction (ED) is still unclear.
Aim: We tried to determine the causal relationship between the level of serum 25(OH)D and ED risk.
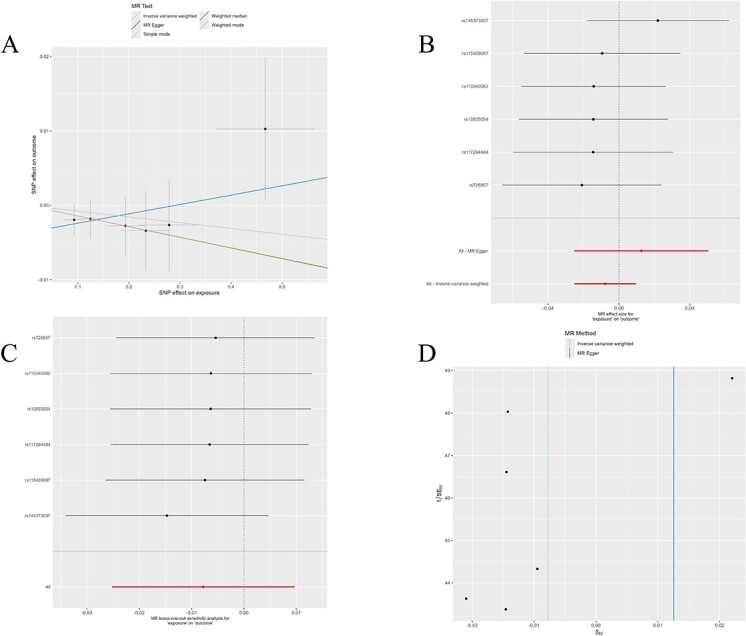
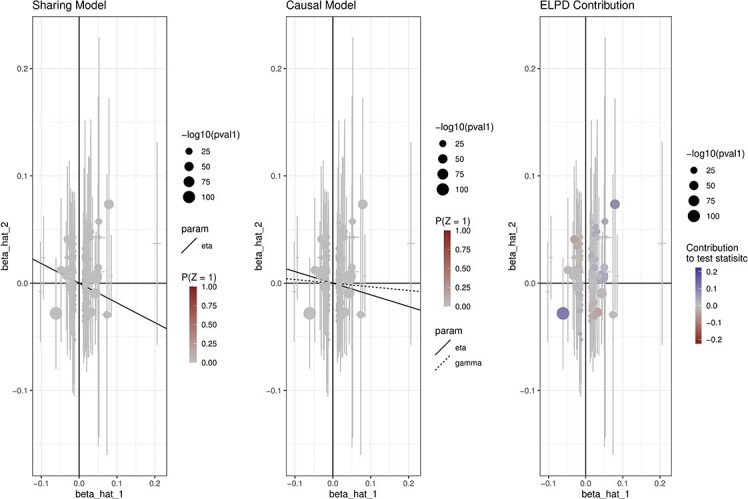
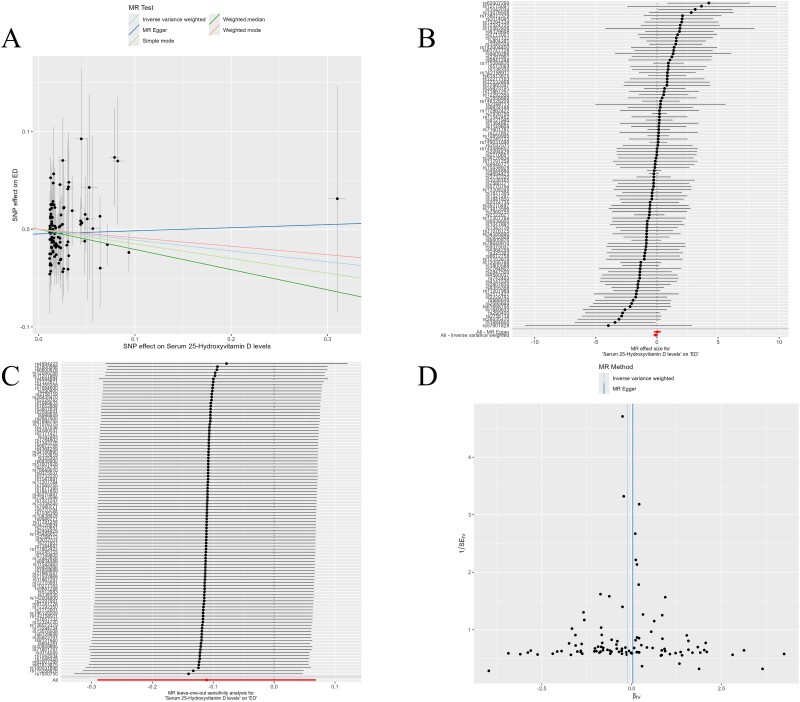
Methods: In this study, we used genome-wide association study data from the UK Biobank to analyse the relationship between serum 25(OH)D (as the exposure) and ED (as the outcome). Linkage disequilibrium score regression (LDSC) was used to assess the genetic correlation between 2 traits. The CAUSE (Causal Analysis using Summary Effect estimates) method and Mendelian randomization (MR) were employed to evaluate the bidirectional causal relationship. The MRlap method was utilized to assess the impact of sample overlap on the results. To assess potential heterogeneity and horizontal pleiotropy, we utilized methods such as MR-Egger, MR-PRESSO (Mendelian Randomization Pleiotropy Residual Sum and Outlier), weighted median, and others.
Outcomes: The primary outcome was defined as self or physician-reported ED, or using oral ED medication, or a history of surgery related to ED.
Results: The LDSC analysis did not reveal a significant genetic correlation between serum 25(OH)D and ED (rg = 0.2787, P = .3536). Additionally, the CAUSE (P value testing that the causal model is a better fit >.05) and MR analyses (odds ratio, 0.8951; 95% confidence interval, 0.7480-1.0710; P = .2260) did not support a causal relationship between 25(OH)D and ED, and our study did not detect any heterogeneity and pleiotropy.
Clinical implications: This study provides evidence on whether vitamin D needs to be ingested to prevent or treat ED.
Strengths and limitations: We used LDSC and MR to avoid bias. However, the population in this study was limited to European ancestry.
Conclusion: No causal relationship was found between 25(OH)D and ED.
期刊介绍:
Sexual Medicine is an official publication of the International Society for Sexual Medicine, and serves the field as the peer-reviewed, open access journal for rapid dissemination of multidisciplinary clinical and basic research in all areas of global sexual medicine, and particularly acts as a venue for topics of regional or sub-specialty interest. The journal is focused on issues in clinical medicine and epidemiology but also publishes basic science papers with particular relevance to specific populations. Sexual Medicine offers clinicians and researchers a rapid route to publication and the opportunity to publish in a broadly distributed and highly visible global forum. The journal publishes high quality articles from all over the world and actively seeks submissions from countries with expanding sexual medicine communities. Sexual Medicine relies on the same expert panel of editors and reviewers as The Journal of Sexual Medicine and Sexual Medicine Reviews.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
