{"title":"使用透视引导和解剖标志在椎体系带术中准确放置螺钉。","authors":"Kevin M Neal, Kylie Krombholz, Mona Doshi","doi":"10.1007/s43390-024-00970-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To determine the accuracy of screw placement using fluoroscopy and anatomic landmarks during vertebral body tethering (VBT) surgery.</p><p><strong>Methods: </strong>Ten patients with 73 VBT screws were converted to posterior spinal fusion (PSF) after continued curve progression. The positions of each VBT screw were analyzed using intraoperative computed tomography (CT) scans performed for image guidance during VBT. Differences for screws placed using an open versus thoracoscopic approach were noted for the screw position in each vertebra, distance from the spinal canal, unicortical versus bicortical placement, the distance of screw tips from the thoracic aorta, and impingement of screws on adjacent rib heads.</p><p><strong>Results: </strong>Seventy three (73) screws in ten (10) patients were available for analysis. Only 21% of screws were placed traversing the middle one-third of the vertebral body, without spinal canal penetration, with the distal tip placed unicortically or bicortically as planned, and without touching the thoracic aorta. The rates of non-ideal screw placement were not significantly different for screws placed via thoracoscopic versus open approaches. Five (5) screws (6.8%) penetrated the spinal canal 1-2 mm, but without known clinical sequelae.</p><p><strong>Conclusion: </strong>The majority of VBT screws available for analysis were placed in non-ideal positions, suggesting that accurate screw placement using intraoperative fluoroscopy and anatomic landmarks can be challenging, but without adverse clinical consequences.</p>","PeriodicalId":21796,"journal":{"name":"Spine deformity","volume":" ","pages":"153-158"},"PeriodicalIF":1.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729129/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of screw placement during vertebral body tethering using fluoroscopic guidance and anatomic landmarks.\",\"authors\":\"Kevin M Neal, Kylie Krombholz, Mona Doshi\",\"doi\":\"10.1007/s43390-024-00970-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To determine the accuracy of screw placement using fluoroscopy and anatomic landmarks during vertebral body tethering (VBT) surgery.</p><p><strong>Methods: </strong>Ten patients with 73 VBT screws were converted to posterior spinal fusion (PSF) after continued curve progression. The positions of each VBT screw were analyzed using intraoperative computed tomography (CT) scans performed for image guidance during VBT. Differences for screws placed using an open versus thoracoscopic approach were noted for the screw position in each vertebra, distance from the spinal canal, unicortical versus bicortical placement, the distance of screw tips from the thoracic aorta, and impingement of screws on adjacent rib heads.</p><p><strong>Results: </strong>Seventy three (73) screws in ten (10) patients were available for analysis. Only 21% of screws were placed traversing the middle one-third of the vertebral body, without spinal canal penetration, with the distal tip placed unicortically or bicortically as planned, and without touching the thoracic aorta. The rates of non-ideal screw placement were not significantly different for screws placed via thoracoscopic versus open approaches. Five (5) screws (6.8%) penetrated the spinal canal 1-2 mm, but without known clinical sequelae.</p><p><strong>Conclusion: </strong>The majority of VBT screws available for analysis were placed in non-ideal positions, suggesting that accurate screw placement using intraoperative fluoroscopy and anatomic landmarks can be challenging, but without adverse clinical consequences.</p>\",\"PeriodicalId\":21796,\"journal\":{\"name\":\"Spine deformity\",\"volume\":\" \",\"pages\":\"153-158\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729129/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine deformity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s43390-024-00970-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine deformity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43390-024-00970-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Accuracy of screw placement during vertebral body tethering using fluoroscopic guidance and anatomic landmarks.
Purpose: To determine the accuracy of screw placement using fluoroscopy and anatomic landmarks during vertebral body tethering (VBT) surgery.
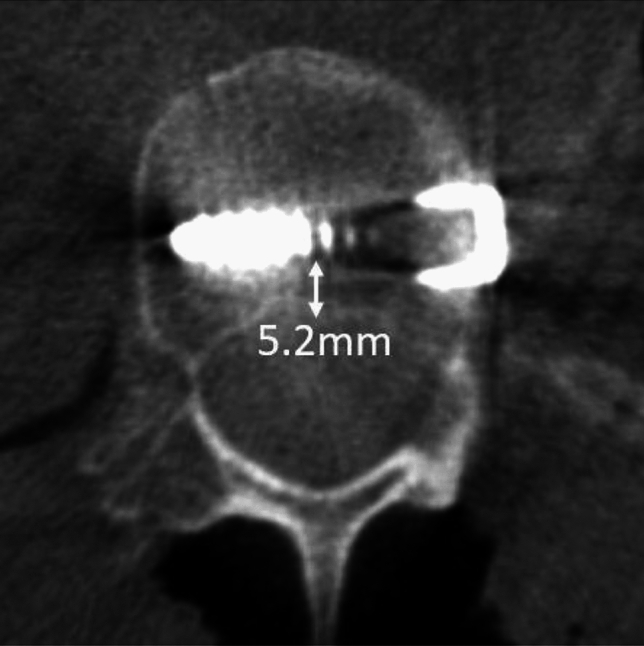
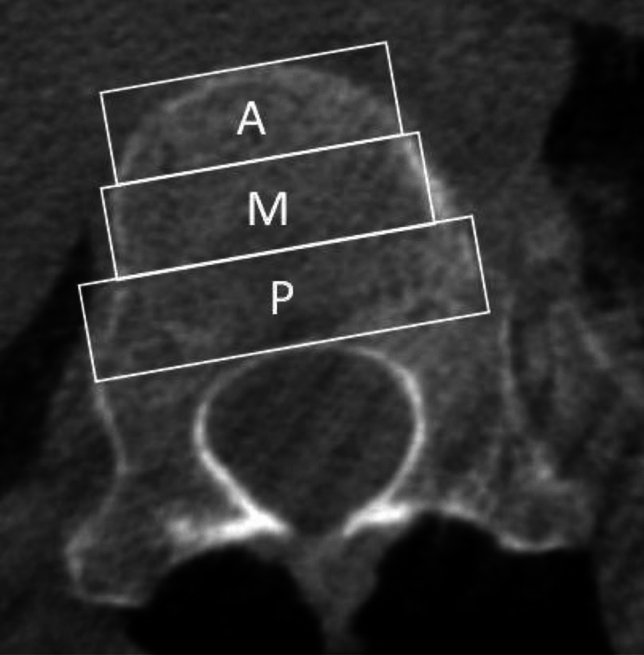
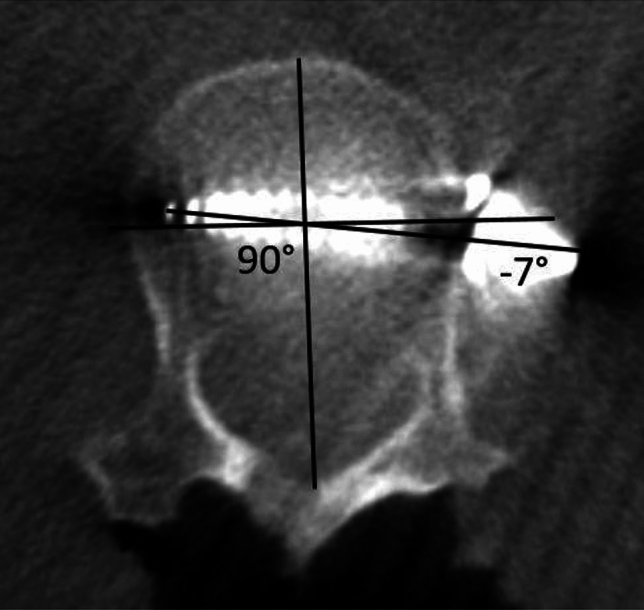
Methods: Ten patients with 73 VBT screws were converted to posterior spinal fusion (PSF) after continued curve progression. The positions of each VBT screw were analyzed using intraoperative computed tomography (CT) scans performed for image guidance during VBT. Differences for screws placed using an open versus thoracoscopic approach were noted for the screw position in each vertebra, distance from the spinal canal, unicortical versus bicortical placement, the distance of screw tips from the thoracic aorta, and impingement of screws on adjacent rib heads.
Results: Seventy three (73) screws in ten (10) patients were available for analysis. Only 21% of screws were placed traversing the middle one-third of the vertebral body, without spinal canal penetration, with the distal tip placed unicortically or bicortically as planned, and without touching the thoracic aorta. The rates of non-ideal screw placement were not significantly different for screws placed via thoracoscopic versus open approaches. Five (5) screws (6.8%) penetrated the spinal canal 1-2 mm, but without known clinical sequelae.
Conclusion: The majority of VBT screws available for analysis were placed in non-ideal positions, suggesting that accurate screw placement using intraoperative fluoroscopy and anatomic landmarks can be challenging, but without adverse clinical consequences.
期刊介绍:
Spine Deformity the official journal of the?Scoliosis Research Society is a peer-refereed publication to disseminate knowledge on basic science and clinical research into the?etiology?biomechanics?treatment?methods and outcomes of all types of?spinal deformities. The international members of the Editorial Board provide a worldwide perspective for the journal's area of interest.The?journal?will enhance the mission of the Society which is to foster the optimal care of all patients with?spine?deformities worldwide. Articles published in?Spine Deformity?are Medline indexed in PubMed.? The journal publishes original articles in the form of clinical and basic research. Spine Deformity will only publish studies that have institutional review board (IRB) or similar ethics committee approval for human and animal studies and have strictly observed these guidelines. The minimum follow-up period for follow-up clinical studies is 24 months.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
