Hyoshin Kwon, Zoya Sandhu, Zoona Sarwar, Oya M Andacoglu
{"title":"医疗补助扩展对俄克拉荷马州肾移植的影响。","authors":"Hyoshin Kwon, Zoya Sandhu, Zoona Sarwar, Oya M Andacoglu","doi":"10.5500/wjt.v14.i3.92981","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no data evaluating the impact of Medicaid expansion on kidney transplants (KT) in Oklahoma.</p><p><strong>Aim: </strong>To investigate the impact of Medicaid expansion on KT patients in Oklahoma.</p><p><strong>Methods: </strong>The UNOS database was utilized to evaluate data pertaining to adult KT recipients in Oklahoma in the pre-and post-Medicaid eras. Bivariate analysis, Kaplan Meier analysis was used to estimate, and cox proportional models were utilized.</p><p><strong>Results: </strong>There were 2758 pre- and 141 recipients in the post-Medicaid expansion era. Post-expansion patients were more often non-United States citizens (2.3% <i>vs</i> 5.7%), American Indian, Alaskan, or Pacific Islander (7.8% <i>vs</i> 9.2%), Hispanic (7.4% <i>vs</i> 12.8%), or Asian (2.5% <i>vs</i> 8.5%) (<i>P</i> < 0.0001). Waitlist time was shorter in the post-expansion era (410 <i>vs</i> 253 d) (<i>P</i> = 0.0011). Living donor rates, pre-emptive transplants, re-do transplants, delayed graft function rates, kidney donor profile index values, panel reactive antibodies levels, and insurance types were similar. Patients with public insurance were more frail. Despite increased early (< 6 months) rejection rates, 1-year patient and graft survival were similar. In Cox proportional hazards model, male sex, American Indian, Alaskan or Pacific Islander race, public insurance, and frailty category were independent risk factors for death at 1 year. Medicaid expansion was not associated with graft failure or patient survival (adjusted hazard ratio: 1.07; 95%CI: 0.26-4.41).</p><p><strong>Conclusion: </strong>Medicaid expansion in Oklahoma is associated with increased KT access for non-White/non-Black and non-United States citizen patients with shorter wait times. 1-year graft and patient survival rates were similar before and after expansion. Medicaid expansion itself was not independently associated with graft or patient survival outcomes. Ongoing research is necessary to determine the long-term effects of Medicaid expansion.</p>","PeriodicalId":65557,"journal":{"name":"世界移植杂志","volume":"14 3","pages":"92981"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11317850/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Medicaid expansion on kidney transplantation in the State Oklahoma.\",\"authors\":\"Hyoshin Kwon, Zoya Sandhu, Zoona Sarwar, Oya M Andacoglu\",\"doi\":\"10.5500/wjt.v14.i3.92981\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is no data evaluating the impact of Medicaid expansion on kidney transplants (KT) in Oklahoma.</p><p><strong>Aim: </strong>To investigate the impact of Medicaid expansion on KT patients in Oklahoma.</p><p><strong>Methods: </strong>The UNOS database was utilized to evaluate data pertaining to adult KT recipients in Oklahoma in the pre-and post-Medicaid eras. Bivariate analysis, Kaplan Meier analysis was used to estimate, and cox proportional models were utilized.</p><p><strong>Results: </strong>There were 2758 pre- and 141 recipients in the post-Medicaid expansion era. Post-expansion patients were more often non-United States citizens (2.3% <i>vs</i> 5.7%), American Indian, Alaskan, or Pacific Islander (7.8% <i>vs</i> 9.2%), Hispanic (7.4% <i>vs</i> 12.8%), or Asian (2.5% <i>vs</i> 8.5%) (<i>P</i> < 0.0001). Waitlist time was shorter in the post-expansion era (410 <i>vs</i> 253 d) (<i>P</i> = 0.0011). Living donor rates, pre-emptive transplants, re-do transplants, delayed graft function rates, kidney donor profile index values, panel reactive antibodies levels, and insurance types were similar. Patients with public insurance were more frail. Despite increased early (< 6 months) rejection rates, 1-year patient and graft survival were similar. In Cox proportional hazards model, male sex, American Indian, Alaskan or Pacific Islander race, public insurance, and frailty category were independent risk factors for death at 1 year. Medicaid expansion was not associated with graft failure or patient survival (adjusted hazard ratio: 1.07; 95%CI: 0.26-4.41).</p><p><strong>Conclusion: </strong>Medicaid expansion in Oklahoma is associated with increased KT access for non-White/non-Black and non-United States citizen patients with shorter wait times. 1-year graft and patient survival rates were similar before and after expansion. Medicaid expansion itself was not independently associated with graft or patient survival outcomes. Ongoing research is necessary to determine the long-term effects of Medicaid expansion.</p>\",\"PeriodicalId\":65557,\"journal\":{\"name\":\"世界移植杂志\",\"volume\":\"14 3\",\"pages\":\"92981\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11317850/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界移植杂志\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5500/wjt.v14.i3.92981\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5500/wjt.v14.i3.92981","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:目的:调查医疗补助扩展对俄克拉荷马州肾移植患者的影响:方法: 利用 UNOS 数据库评估俄克拉荷马州成年 KT 患者在医疗补助计划实施前后的相关数据。采用双变量分析、卡普兰-梅耶尔分析进行估算,并使用考克斯比例模型:结果:医疗补助扩展前有 2758 名患者,扩展后有 141 名患者。扩大后的患者多为非美国公民(2.3% vs 5.7%)、美国印第安人、阿拉斯加人或太平洋岛民(7.8% vs 9.2%)、西班牙裔(7.4% vs 12.8%)或亚裔(2.5% vs 8.5%)(P < 0.0001)。扩大后的等待时间更短(410 天 vs 253 天)(P = 0.0011)。活体捐献率、抢先移植、再次移植、移植功能延迟率、肾脏捐献者档案指数值、面板反应性抗体水平和保险类型相似。参加公共保险的患者更加虚弱。尽管早期(< 6 个月)排斥率增加,但患者和移植物的 1 年存活率相似。在 Cox 比例危险模型中,男性、美国印第安人、阿拉斯加或太平洋岛民、公共保险和虚弱类别是导致 1 年死亡的独立危险因素。医疗补助计划的扩大与移植失败或患者存活率无关(调整后危险比:1.07;95%CI:0.26-4.41):结论:俄克拉荷马州扩大医疗补助计划与非白人/非黑人和非美国公民患者接受 KT 的机会增加以及等待时间缩短有关。扩建前后的 1 年移植物存活率和患者存活率相似。医疗补助计划的扩大本身与移植物或患者的存活率并无独立关联。要确定扩大医疗补助计划的长期影响,还需要进行持续的研究。
Impact of Medicaid expansion on kidney transplantation in the State Oklahoma.
Background: There is no data evaluating the impact of Medicaid expansion on kidney transplants (KT) in Oklahoma.
Aim: To investigate the impact of Medicaid expansion on KT patients in Oklahoma.
Methods: The UNOS database was utilized to evaluate data pertaining to adult KT recipients in Oklahoma in the pre-and post-Medicaid eras. Bivariate analysis, Kaplan Meier analysis was used to estimate, and cox proportional models were utilized.
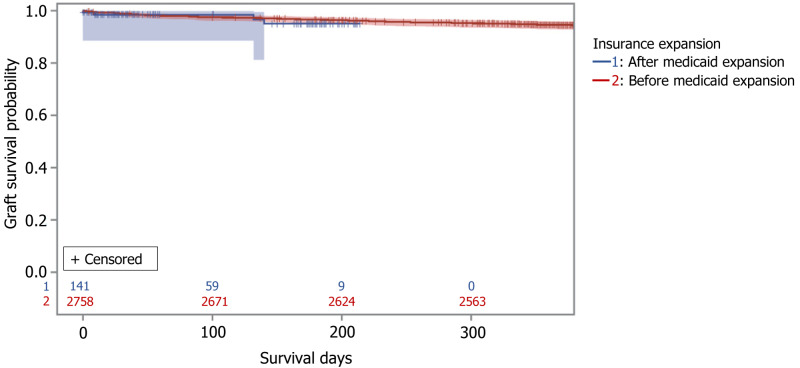
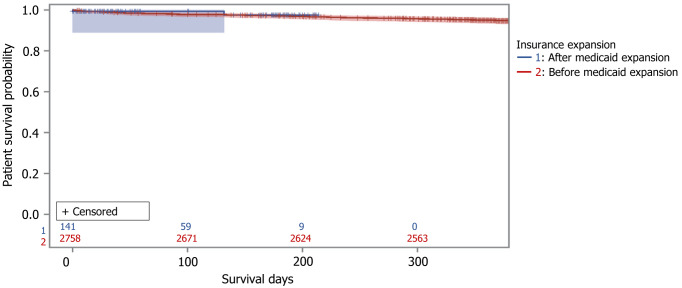
Results: There were 2758 pre- and 141 recipients in the post-Medicaid expansion era. Post-expansion patients were more often non-United States citizens (2.3% vs 5.7%), American Indian, Alaskan, or Pacific Islander (7.8% vs 9.2%), Hispanic (7.4% vs 12.8%), or Asian (2.5% vs 8.5%) (P < 0.0001). Waitlist time was shorter in the post-expansion era (410 vs 253 d) (P = 0.0011). Living donor rates, pre-emptive transplants, re-do transplants, delayed graft function rates, kidney donor profile index values, panel reactive antibodies levels, and insurance types were similar. Patients with public insurance were more frail. Despite increased early (< 6 months) rejection rates, 1-year patient and graft survival were similar. In Cox proportional hazards model, male sex, American Indian, Alaskan or Pacific Islander race, public insurance, and frailty category were independent risk factors for death at 1 year. Medicaid expansion was not associated with graft failure or patient survival (adjusted hazard ratio: 1.07; 95%CI: 0.26-4.41).
Conclusion: Medicaid expansion in Oklahoma is associated with increased KT access for non-White/non-Black and non-United States citizen patients with shorter wait times. 1-year graft and patient survival rates were similar before and after expansion. Medicaid expansion itself was not independently associated with graft or patient survival outcomes. Ongoing research is necessary to determine the long-term effects of Medicaid expansion.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
