Stephen Schmit, Kamil Malshy, Alexander Homer, Borivoj Golijanin, Christopher Tucci, Rebecca Ortiz, Sari Khaleel, Elias Hyams, Dragan Golijanin
{"title":"微创手术时代肾切除术前机械肠道准备的评估:美国国家数据库分析的启示。","authors":"Stephen Schmit, Kamil Malshy, Alexander Homer, Borivoj Golijanin, Christopher Tucci, Rebecca Ortiz, Sari Khaleel, Elias Hyams, Dragan Golijanin","doi":"10.7602/jmis.2024.27.3.165","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study was performed to evaluate the association between mechanical bowel preparation (MBP) and perioperative outcomes following nephrectomy in the minimally invasive surgery (MIS) era.</p><p><strong>Methods: </strong>All partial and radical nephrectomies between 2019 and 2021 from the National Surgical Quality Improvement Program database were evaluated. Thirty-day perioperative outcomes were compared between groups where MBP was performed vs. not, in both the MIS and open surgery (OS) cohorts. A propensity score matching technique was utilized within MIS cases to control for covariates. The chi-square and <i>t</i> tests were used to determine significance.</p><p><strong>Results: </strong>A total of 11,869 cases met the inclusion criteria and were included in the analysis. Of these, 8,204 (69.1%; comprising 65.3% robotic and 34.7% laparoscopic) underwent MIS, while 3,665 (30.9%) underwent OS. The rate of MBP was higher in the MIS group (16.0% vs. 10.0%, <i>p</i> < 0.001). Within the MIS group, MBP was associated with reduced rates of postoperative ileus (0.9% vs. 1.9%, <i>p</i> = 0.02), while other complications were comparable. Propensity score matching showed no association between MBP and postoperative ileus. However, a lower rate of 30-day readmission in the MBP group became statistically significant (4.4% vs. 6.4%, <i>p</i> = 0.01). Conversely, patients in the MBP group also demonstrated higher rates of pneumonia (1.3% vs. 0.5%, <i>p</i> = 0.002) and pulmonary embolism (0.6% vs. 0%, <i>p</i> < 0.001) after matching.</p><p><strong>Conclusion: </strong>MBP practice prior to nephrectomy is infrequent in both OS and MIS cases, with minor differences in perioperative outcomes for patients undergoing MIS. Routine MBP should continue to be excluded from the standard of care for nephrectomy in the MIS era.</p>","PeriodicalId":73832,"journal":{"name":"Journal of minimally invasive surgery","volume":"27 3","pages":"165-171"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11416889/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessment of mechanical bowel preparation prior to nephrectomy in the minimally invasive surgery era: insights from a national database analysis in the United States.\",\"authors\":\"Stephen Schmit, Kamil Malshy, Alexander Homer, Borivoj Golijanin, Christopher Tucci, Rebecca Ortiz, Sari Khaleel, Elias Hyams, Dragan Golijanin\",\"doi\":\"10.7602/jmis.2024.27.3.165\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study was performed to evaluate the association between mechanical bowel preparation (MBP) and perioperative outcomes following nephrectomy in the minimally invasive surgery (MIS) era.</p><p><strong>Methods: </strong>All partial and radical nephrectomies between 2019 and 2021 from the National Surgical Quality Improvement Program database were evaluated. Thirty-day perioperative outcomes were compared between groups where MBP was performed vs. not, in both the MIS and open surgery (OS) cohorts. A propensity score matching technique was utilized within MIS cases to control for covariates. The chi-square and <i>t</i> tests were used to determine significance.</p><p><strong>Results: </strong>A total of 11,869 cases met the inclusion criteria and were included in the analysis. Of these, 8,204 (69.1%; comprising 65.3% robotic and 34.7% laparoscopic) underwent MIS, while 3,665 (30.9%) underwent OS. The rate of MBP was higher in the MIS group (16.0% vs. 10.0%, <i>p</i> < 0.001). Within the MIS group, MBP was associated with reduced rates of postoperative ileus (0.9% vs. 1.9%, <i>p</i> = 0.02), while other complications were comparable. Propensity score matching showed no association between MBP and postoperative ileus. However, a lower rate of 30-day readmission in the MBP group became statistically significant (4.4% vs. 6.4%, <i>p</i> = 0.01). Conversely, patients in the MBP group also demonstrated higher rates of pneumonia (1.3% vs. 0.5%, <i>p</i> = 0.002) and pulmonary embolism (0.6% vs. 0%, <i>p</i> < 0.001) after matching.</p><p><strong>Conclusion: </strong>MBP practice prior to nephrectomy is infrequent in both OS and MIS cases, with minor differences in perioperative outcomes for patients undergoing MIS. Routine MBP should continue to be excluded from the standard of care for nephrectomy in the MIS era.</p>\",\"PeriodicalId\":73832,\"journal\":{\"name\":\"Journal of minimally invasive surgery\",\"volume\":\"27 3\",\"pages\":\"165-171\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11416889/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of minimally invasive surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7602/jmis.2024.27.3.165\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of minimally invasive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7602/jmis.2024.27.3.165","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究旨在评估微创手术(MIS)时代机械肠道准备(MBP)与肾切除术后围手术期结果之间的关联:对国家外科质量改进计划数据库中2019年至2021年间的所有肾部分切除术和根治性肾切除术进行了评估。在 MIS 和开放手术 (OS) 两组中,比较了实施 MBP 与未实施 MBP 两组的 30 天围手术期结果。在 MIS 病例中使用了倾向得分匹配技术来控制协变量。结果:共有 11,869 个病例符合纳入标准并纳入分析。其中,8204例(69.1%;包括65.3%的机器人手术和34.7%的腹腔镜手术)接受了MIS手术,3655例(30.9%)接受了OS手术。MIS 组的 MBP 发生率更高(16.0% 对 10.0%,P < 0.001)。在 MIS 组中,MBP 与术后回肠瘘发生率降低有关(0.9% 对 1.9%,p = 0.02),而其他并发症的发生率相当。倾向评分匹配显示 MBP 与术后回肠梗阻之间没有关联。不过,MBP 组 30 天再入院率较低,这在统计学上具有显著意义(4.4% 对 6.4%,P = 0.01)。相反,MBP 组患者在匹配后的肺炎(1.29% 对 0.46%,p = 0.002)和肺栓塞(0.6% 对 0%,p < 0.001)发生率也较高:肾切除术前的 MBP 在 OS 和 MIS 病例中都不常见,MIS 患者的围手术期结果差异较小。在 MIS 时代,常规 MBP 应继续排除在肾切除术标准护理之外。
Assessment of mechanical bowel preparation prior to nephrectomy in the minimally invasive surgery era: insights from a national database analysis in the United States.
Purpose: This study was performed to evaluate the association between mechanical bowel preparation (MBP) and perioperative outcomes following nephrectomy in the minimally invasive surgery (MIS) era.
Methods: All partial and radical nephrectomies between 2019 and 2021 from the National Surgical Quality Improvement Program database were evaluated. Thirty-day perioperative outcomes were compared between groups where MBP was performed vs. not, in both the MIS and open surgery (OS) cohorts. A propensity score matching technique was utilized within MIS cases to control for covariates. The chi-square and t tests were used to determine significance.
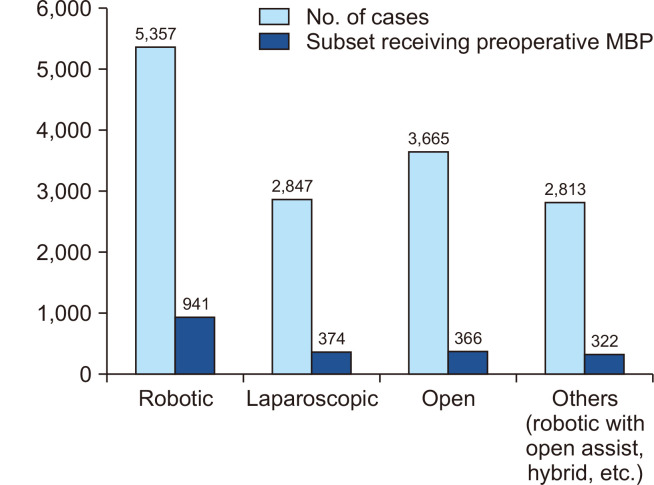
Results: A total of 11,869 cases met the inclusion criteria and were included in the analysis. Of these, 8,204 (69.1%; comprising 65.3% robotic and 34.7% laparoscopic) underwent MIS, while 3,665 (30.9%) underwent OS. The rate of MBP was higher in the MIS group (16.0% vs. 10.0%, p < 0.001). Within the MIS group, MBP was associated with reduced rates of postoperative ileus (0.9% vs. 1.9%, p = 0.02), while other complications were comparable. Propensity score matching showed no association between MBP and postoperative ileus. However, a lower rate of 30-day readmission in the MBP group became statistically significant (4.4% vs. 6.4%, p = 0.01). Conversely, patients in the MBP group also demonstrated higher rates of pneumonia (1.3% vs. 0.5%, p = 0.002) and pulmonary embolism (0.6% vs. 0%, p < 0.001) after matching.
Conclusion: MBP practice prior to nephrectomy is infrequent in both OS and MIS cases, with minor differences in perioperative outcomes for patients undergoing MIS. Routine MBP should continue to be excluded from the standard of care for nephrectomy in the MIS era.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
