{"title":"股骨骨矿物质密度是治疗类风湿性关节炎的个性化医疗工具:白细胞介素-6抑制剂适用于低密度患者,而肿瘤坏死因子抑制剂适用于高密度患者?","authors":"Hirokazu Takaoka, Tomohiro Miyamura, Kota Shimada","doi":"10.1177/20503121241277498","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>There is a lack of indicators to distinguish between interleukin-6 inhibitors responders and tumor necrosis factor inhibitors responders in the treatment of rheumatoid arthritis. Osteoporosis is a complication of rheumatoid arthritis and is closely related to inflammatory pathology. The purpose of this study was to evaluate whether bone mineral density can distinguish interleukin-6 inhibitors responders from tumor necrosis factor inhibitors responders in rheumatoid arthritis.</p><p><strong>Methods: </strong>Either interleukin-6 inhibitors or tumor necrosis factor inhibitors was introduced as the first biologics to patients naïve to both corticosteroid and osteoporosis treatment. Correlations between baseline bone mineral density and Clinical Disease Activity Index after 3 months were analyzed.</p><p><strong>Results: </strong>The subjects were 26 rheumatoid arthritis patients with a median age of 60 years old, disease duration of 1.4 years, Clinical Disease Activity Index of 13.7, and C-reactive protein of 1.69 mg/dL. The subjects were divided into two groups (high (H) and low (L)) according to their femoral bone mineral density with a cutoff of young adult mean of 80%. Six in group H and 11 in group L received interleukin-6 inhibitors, and nine in group H received tumor necrosis factor inhibitors. Clinical Disease Activity Index remission rate by interleukin-6 inhibitors was significantly greater in group L (8/11 (72.7%)) than in group H (1/6 (16.7%); <i>p</i> < 0.05). In the whole group H, significantly more patients obtained Clinical Disease Activity Index remission by tumor necrosis factor inhibitors (7/9, 77.8%) than by interleukin-6 inhibitors (1/6 (16.7%); <i>p</i> = 0.04).</p><p><strong>Conclusions: </strong>In patients with rheumatoid arthritis, interleukin-6 inhibitors may be more beneficial for patients with low femoral bone mineral density, whereas tumor necrosis factor inhibitors may be advantageous for those with preserved bone mineral density.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"12 ","pages":"20503121241277498"},"PeriodicalIF":2.2000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11418348/pdf/","citationCount":"0","resultStr":"{\"title\":\"Femoral bone mineral density as a tool of personalized medicine for rheumatoid arthritis: Interleukin-6 inhibitors for patients with low density whereas tumor necrosis factor inhibitor for patients with preserved density?\",\"authors\":\"Hirokazu Takaoka, Tomohiro Miyamura, Kota Shimada\",\"doi\":\"10.1177/20503121241277498\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>There is a lack of indicators to distinguish between interleukin-6 inhibitors responders and tumor necrosis factor inhibitors responders in the treatment of rheumatoid arthritis. Osteoporosis is a complication of rheumatoid arthritis and is closely related to inflammatory pathology. The purpose of this study was to evaluate whether bone mineral density can distinguish interleukin-6 inhibitors responders from tumor necrosis factor inhibitors responders in rheumatoid arthritis.</p><p><strong>Methods: </strong>Either interleukin-6 inhibitors or tumor necrosis factor inhibitors was introduced as the first biologics to patients naïve to both corticosteroid and osteoporosis treatment. Correlations between baseline bone mineral density and Clinical Disease Activity Index after 3 months were analyzed.</p><p><strong>Results: </strong>The subjects were 26 rheumatoid arthritis patients with a median age of 60 years old, disease duration of 1.4 years, Clinical Disease Activity Index of 13.7, and C-reactive protein of 1.69 mg/dL. The subjects were divided into two groups (high (H) and low (L)) according to their femoral bone mineral density with a cutoff of young adult mean of 80%. Six in group H and 11 in group L received interleukin-6 inhibitors, and nine in group H received tumor necrosis factor inhibitors. Clinical Disease Activity Index remission rate by interleukin-6 inhibitors was significantly greater in group L (8/11 (72.7%)) than in group H (1/6 (16.7%); <i>p</i> < 0.05). In the whole group H, significantly more patients obtained Clinical Disease Activity Index remission by tumor necrosis factor inhibitors (7/9, 77.8%) than by interleukin-6 inhibitors (1/6 (16.7%); <i>p</i> = 0.04).</p><p><strong>Conclusions: </strong>In patients with rheumatoid arthritis, interleukin-6 inhibitors may be more beneficial for patients with low femoral bone mineral density, whereas tumor necrosis factor inhibitors may be advantageous for those with preserved bone mineral density.</p>\",\"PeriodicalId\":21398,\"journal\":{\"name\":\"SAGE Open Medicine\",\"volume\":\"12 \",\"pages\":\"20503121241277498\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11418348/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAGE Open Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20503121241277498\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121241277498","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Femoral bone mineral density as a tool of personalized medicine for rheumatoid arthritis: Interleukin-6 inhibitors for patients with low density whereas tumor necrosis factor inhibitor for patients with preserved density?
Objectives: There is a lack of indicators to distinguish between interleukin-6 inhibitors responders and tumor necrosis factor inhibitors responders in the treatment of rheumatoid arthritis. Osteoporosis is a complication of rheumatoid arthritis and is closely related to inflammatory pathology. The purpose of this study was to evaluate whether bone mineral density can distinguish interleukin-6 inhibitors responders from tumor necrosis factor inhibitors responders in rheumatoid arthritis.
Methods: Either interleukin-6 inhibitors or tumor necrosis factor inhibitors was introduced as the first biologics to patients naïve to both corticosteroid and osteoporosis treatment. Correlations between baseline bone mineral density and Clinical Disease Activity Index after 3 months were analyzed.
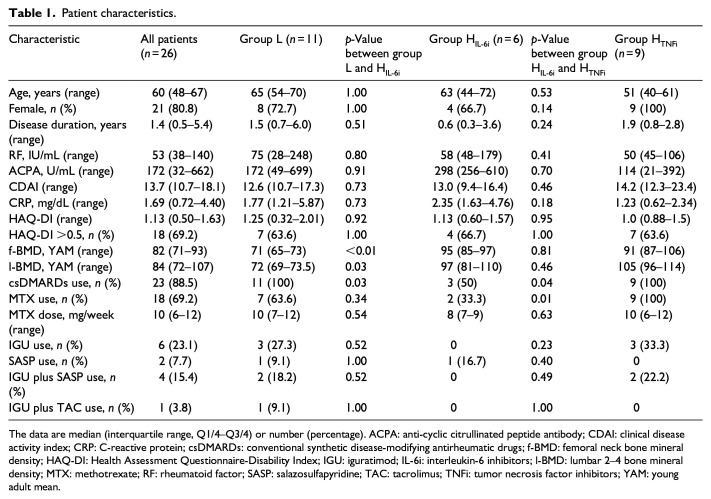
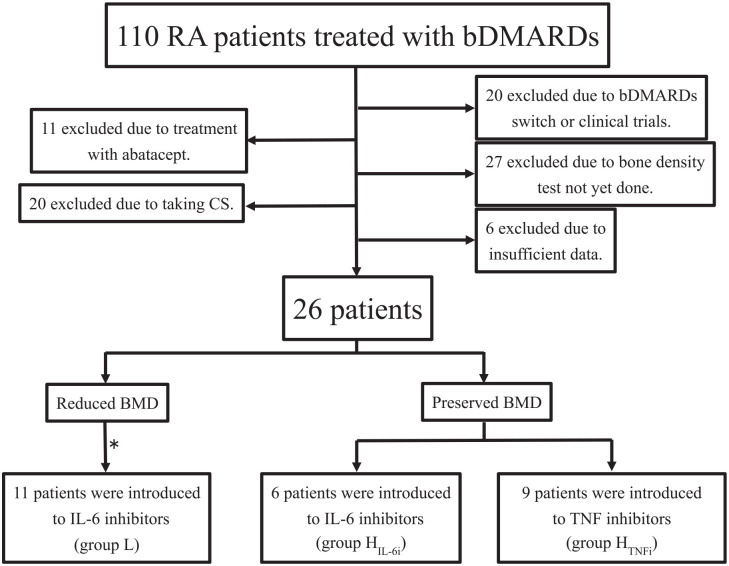
Results: The subjects were 26 rheumatoid arthritis patients with a median age of 60 years old, disease duration of 1.4 years, Clinical Disease Activity Index of 13.7, and C-reactive protein of 1.69 mg/dL. The subjects were divided into two groups (high (H) and low (L)) according to their femoral bone mineral density with a cutoff of young adult mean of 80%. Six in group H and 11 in group L received interleukin-6 inhibitors, and nine in group H received tumor necrosis factor inhibitors. Clinical Disease Activity Index remission rate by interleukin-6 inhibitors was significantly greater in group L (8/11 (72.7%)) than in group H (1/6 (16.7%); p < 0.05). In the whole group H, significantly more patients obtained Clinical Disease Activity Index remission by tumor necrosis factor inhibitors (7/9, 77.8%) than by interleukin-6 inhibitors (1/6 (16.7%); p = 0.04).
Conclusions: In patients with rheumatoid arthritis, interleukin-6 inhibitors may be more beneficial for patients with low femoral bone mineral density, whereas tumor necrosis factor inhibitors may be advantageous for those with preserved bone mineral density.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
