{"title":"异常胃息肉","authors":"Kai-Jie Lin, I-Min Tsai, Yi-Ting Chen, Chun-Chi Hsu, Wen-Hung Hsu","doi":"10.1002/aid2.13402","DOIUrl":null,"url":null,"abstract":"<p>A 56-year-old male had a history of tongue and hypopharyngeal cancers following surgery as well as early esophageal squamous cell neoplasm detected after endoscopic submucosal dissection (ESD). His head and neck cancers and esophageal neoplasm stabilized and he underwent esophagogastroduodenoscopy (EGD) follow-up annually. During one such follow-up, a Type 0-Isp whitish protruding mucosal lesion, 1.5 cm, below esophagogastric junction (EG junction) (Figures 1A,B) was discovered. One month later, during follow-up EGD (Figure 1C), the lesion appeared more fragile and irregular with its texture revealed as having a rigid base after endoscopic biopsy. Computed tomography (CT) revealed subtle gastric mucosa thickening (Figure 1D). Despite six endoscopic biopsies, histological examination only showed ulcer and atypical cells.</p><p>What is the next step? What is the diagnosis?</p><p>Due to suspicion of malignancy, a diagnostic treatment with ESD was performed for a complete pathology examination. During the ESD procedure, performed using Dual knife, an IT-nano knife, a polypoid lesion with fragility was noted below the EG junction, extending to the cardiac region. The procedure revealed that the lesion was separated from the muscular propria (Figure 2A). En-bloc resection was achieved without major complication. Pathologic examination revealed interlacing fascicles of spindle-shaped cells with increased cellularity (Figures 2B,C). The special stain showed SMA(+) (Figure 2D), focal positivity for Desmin and caldesmon, and negativity for CD34, CD117, S-100 and Dog-1. Based on these morphological and immunohistochemical studies, leiomyosarcoma was considered. Surgical esophagectomy was suggested but the patient rejected this; as a result, adjuvant radiotherapy with a dosage of 6000 cGy/30fr was administered. Subsequent years of treatment involved endoscopy and CT follow-ups, and complete remission was achieved.</p><p>Leiomyosarcomas of the stomach are rare malignant tumors derived from smooth muscle tissue,<span><sup>1</sup></span> derived not only from muscularis propria, but could also be from muscularis mucosa. Image surveillance with endoscopic ultrasound and computed tomography would be helpful for clarification.<span><sup>2</sup></span> Surgical treatment such as esophagectomy is often the preferred choice<span><sup>3</sup></span>; however, based on our experience, ESD has been found to be useful for proper pathological examination, and salvage radiotherapy is a reasonable option if patient is unsuited for esophagectomy.</p><p>The authors declare no conflicts of interest.</p><p>Informed consent was obtained from the patient to publish this article and images.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 3","pages":"170-171"},"PeriodicalIF":0.4000,"publicationDate":"2024-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13402","citationCount":"0","resultStr":"{\"title\":\"Unusual gastric polyp\",\"authors\":\"Kai-Jie Lin, I-Min Tsai, Yi-Ting Chen, Chun-Chi Hsu, Wen-Hung Hsu\",\"doi\":\"10.1002/aid2.13402\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 56-year-old male had a history of tongue and hypopharyngeal cancers following surgery as well as early esophageal squamous cell neoplasm detected after endoscopic submucosal dissection (ESD). His head and neck cancers and esophageal neoplasm stabilized and he underwent esophagogastroduodenoscopy (EGD) follow-up annually. During one such follow-up, a Type 0-Isp whitish protruding mucosal lesion, 1.5 cm, below esophagogastric junction (EG junction) (Figures 1A,B) was discovered. One month later, during follow-up EGD (Figure 1C), the lesion appeared more fragile and irregular with its texture revealed as having a rigid base after endoscopic biopsy. Computed tomography (CT) revealed subtle gastric mucosa thickening (Figure 1D). Despite six endoscopic biopsies, histological examination only showed ulcer and atypical cells.</p><p>What is the next step? What is the diagnosis?</p><p>Due to suspicion of malignancy, a diagnostic treatment with ESD was performed for a complete pathology examination. During the ESD procedure, performed using Dual knife, an IT-nano knife, a polypoid lesion with fragility was noted below the EG junction, extending to the cardiac region. The procedure revealed that the lesion was separated from the muscular propria (Figure 2A). En-bloc resection was achieved without major complication. Pathologic examination revealed interlacing fascicles of spindle-shaped cells with increased cellularity (Figures 2B,C). The special stain showed SMA(+) (Figure 2D), focal positivity for Desmin and caldesmon, and negativity for CD34, CD117, S-100 and Dog-1. Based on these morphological and immunohistochemical studies, leiomyosarcoma was considered. Surgical esophagectomy was suggested but the patient rejected this; as a result, adjuvant radiotherapy with a dosage of 6000 cGy/30fr was administered. Subsequent years of treatment involved endoscopy and CT follow-ups, and complete remission was achieved.</p><p>Leiomyosarcomas of the stomach are rare malignant tumors derived from smooth muscle tissue,<span><sup>1</sup></span> derived not only from muscularis propria, but could also be from muscularis mucosa. Image surveillance with endoscopic ultrasound and computed tomography would be helpful for clarification.<span><sup>2</sup></span> Surgical treatment such as esophagectomy is often the preferred choice<span><sup>3</sup></span>; however, based on our experience, ESD has been found to be useful for proper pathological examination, and salvage radiotherapy is a reasonable option if patient is unsuited for esophagectomy.</p><p>The authors declare no conflicts of interest.</p><p>Informed consent was obtained from the patient to publish this article and images.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"11 3\",\"pages\":\"170-171\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2024-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13402\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13402\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13402","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
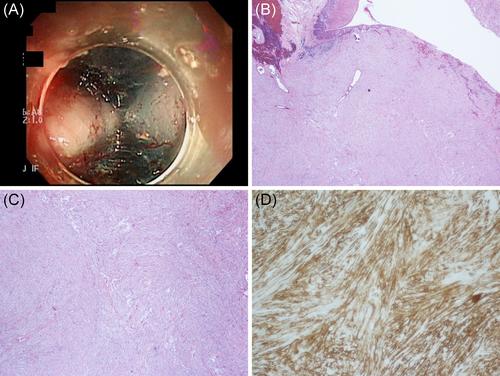
A 56-year-old male had a history of tongue and hypopharyngeal cancers following surgery as well as early esophageal squamous cell neoplasm detected after endoscopic submucosal dissection (ESD). His head and neck cancers and esophageal neoplasm stabilized and he underwent esophagogastroduodenoscopy (EGD) follow-up annually. During one such follow-up, a Type 0-Isp whitish protruding mucosal lesion, 1.5 cm, below esophagogastric junction (EG junction) (Figures 1A,B) was discovered. One month later, during follow-up EGD (Figure 1C), the lesion appeared more fragile and irregular with its texture revealed as having a rigid base after endoscopic biopsy. Computed tomography (CT) revealed subtle gastric mucosa thickening (Figure 1D). Despite six endoscopic biopsies, histological examination only showed ulcer and atypical cells.
What is the next step? What is the diagnosis?
Due to suspicion of malignancy, a diagnostic treatment with ESD was performed for a complete pathology examination. During the ESD procedure, performed using Dual knife, an IT-nano knife, a polypoid lesion with fragility was noted below the EG junction, extending to the cardiac region. The procedure revealed that the lesion was separated from the muscular propria (Figure 2A). En-bloc resection was achieved without major complication. Pathologic examination revealed interlacing fascicles of spindle-shaped cells with increased cellularity (Figures 2B,C). The special stain showed SMA(+) (Figure 2D), focal positivity for Desmin and caldesmon, and negativity for CD34, CD117, S-100 and Dog-1. Based on these morphological and immunohistochemical studies, leiomyosarcoma was considered. Surgical esophagectomy was suggested but the patient rejected this; as a result, adjuvant radiotherapy with a dosage of 6000 cGy/30fr was administered. Subsequent years of treatment involved endoscopy and CT follow-ups, and complete remission was achieved.
Leiomyosarcomas of the stomach are rare malignant tumors derived from smooth muscle tissue,1 derived not only from muscularis propria, but could also be from muscularis mucosa. Image surveillance with endoscopic ultrasound and computed tomography would be helpful for clarification.2 Surgical treatment such as esophagectomy is often the preferred choice3; however, based on our experience, ESD has been found to be useful for proper pathological examination, and salvage radiotherapy is a reasonable option if patient is unsuited for esophagectomy.
The authors declare no conflicts of interest.
Informed consent was obtained from the patient to publish this article and images.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
