Gabriel Kanhouche, Jose Carlos Nicolau, Remo Holanda de Mendonça Furtado, Luiz Sérgio Carvalho, Talia Falcão Dalçoquio, Brunna Pileggi, Mauricio Felippi de Sa Marchi, Pedro Abi-Kair, Neuza Lopes, Roberto Rocha Giraldez, Luciano Moreira Baracioli, Felipe Gallego Lima, Ludhmila Abrahão Hajjar, Roberto Kalil Filho, Fábio Sandoli de Brito Junior, Alexandre Abizaid, Henrique Barbosa Ribeiro
{"title":"ST段抬高型心肌梗死并发心源性休克和心脏骤停的长期预后取决于发生时间。","authors":"Gabriel Kanhouche, Jose Carlos Nicolau, Remo Holanda de Mendonça Furtado, Luiz Sérgio Carvalho, Talia Falcão Dalçoquio, Brunna Pileggi, Mauricio Felippi de Sa Marchi, Pedro Abi-Kair, Neuza Lopes, Roberto Rocha Giraldez, Luciano Moreira Baracioli, Felipe Gallego Lima, Ludhmila Abrahão Hajjar, Roberto Kalil Filho, Fábio Sandoli de Brito Junior, Alexandre Abizaid, Henrique Barbosa Ribeiro","doi":"10.1093/ehjopen/oeae075","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiogenic shock (CS) and cardiac arrest (CA) are serious complications in ST-elevation myocardial infarction (STEMI) patients, with lack of long-term data according to their timing of occurrence. This study sought to determine the incidence and relationship between the timing of occurrence and prognostic impact of CS and CA complicating STEMI in the long-term follow-up.</p><p><strong>Methods and results: </strong>We conducted a retrospective analysis of consecutive STEMI patients treated between 2004 and 2017. Patients were divided into four groups based on the occurrence of neither CA nor CS, CA only, CS only, and both CA and CS (CA-CS-, CA+, CS+, and CA+CS+, respectively). Adjusted Cox regression analysis was used to assess the independent association between the CS and CA categories and mortality. A total of 1603 STEMI patients were followed for a median of 3.6 years. CA and CS occurred in the 12.2% and 15.9% of patients, and both impacted long-term mortality [adjusted hazard ratio (HR) = 2.59, 95% confidence interval (CI): 1.53-4.41, <i>P</i> < 0.001; HR = 3.16, 95% CI: 2.21-4.53, <i>P</i> < 0.001, respectively). CA+CS+ occurred in 7.3%, with the strongest association with higher mortality (adjusted HR = 5.36; 95% CI: 3.80-7.55, <i>P</i> < 0.001). Using flexible parametric models with B-splines, the increased mortality was restricted to the first ∼10 months. In addition, overall mortality rates were higher at all timings (all with <i>P</i> < 0.001), except for CA during initial cardiac catheterization (<i>P</i> < 0.183).</p><p><strong>Conclusion: </strong>CS and CA complicating patients presenting with STEMI were associated with higher long-term mortality rate, especially in the first 10 months. Both CS+ and CA+ at any timeframe impacted outcomes, except for CA+ during the initial cardiac catheterization, although this will have to be confirmed in larger future studies, given the relatively small number of patients.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 5","pages":"oeae075"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11430270/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term outcomes of cardiogenic shock and cardiac arrest complicating ST-elevation myocardial infarction according to timing of occurrence.\",\"authors\":\"Gabriel Kanhouche, Jose Carlos Nicolau, Remo Holanda de Mendonça Furtado, Luiz Sérgio Carvalho, Talia Falcão Dalçoquio, Brunna Pileggi, Mauricio Felippi de Sa Marchi, Pedro Abi-Kair, Neuza Lopes, Roberto Rocha Giraldez, Luciano Moreira Baracioli, Felipe Gallego Lima, Ludhmila Abrahão Hajjar, Roberto Kalil Filho, Fábio Sandoli de Brito Junior, Alexandre Abizaid, Henrique Barbosa Ribeiro\",\"doi\":\"10.1093/ehjopen/oeae075\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Cardiogenic shock (CS) and cardiac arrest (CA) are serious complications in ST-elevation myocardial infarction (STEMI) patients, with lack of long-term data according to their timing of occurrence. This study sought to determine the incidence and relationship between the timing of occurrence and prognostic impact of CS and CA complicating STEMI in the long-term follow-up.</p><p><strong>Methods and results: </strong>We conducted a retrospective analysis of consecutive STEMI patients treated between 2004 and 2017. Patients were divided into four groups based on the occurrence of neither CA nor CS, CA only, CS only, and both CA and CS (CA-CS-, CA+, CS+, and CA+CS+, respectively). Adjusted Cox regression analysis was used to assess the independent association between the CS and CA categories and mortality. A total of 1603 STEMI patients were followed for a median of 3.6 years. CA and CS occurred in the 12.2% and 15.9% of patients, and both impacted long-term mortality [adjusted hazard ratio (HR) = 2.59, 95% confidence interval (CI): 1.53-4.41, <i>P</i> < 0.001; HR = 3.16, 95% CI: 2.21-4.53, <i>P</i> < 0.001, respectively). CA+CS+ occurred in 7.3%, with the strongest association with higher mortality (adjusted HR = 5.36; 95% CI: 3.80-7.55, <i>P</i> < 0.001). Using flexible parametric models with B-splines, the increased mortality was restricted to the first ∼10 months. In addition, overall mortality rates were higher at all timings (all with <i>P</i> < 0.001), except for CA during initial cardiac catheterization (<i>P</i> < 0.183).</p><p><strong>Conclusion: </strong>CS and CA complicating patients presenting with STEMI were associated with higher long-term mortality rate, especially in the first 10 months. Both CS+ and CA+ at any timeframe impacted outcomes, except for CA+ during the initial cardiac catheterization, although this will have to be confirmed in larger future studies, given the relatively small number of patients.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"4 5\",\"pages\":\"oeae075\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11430270/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeae075\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae075","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
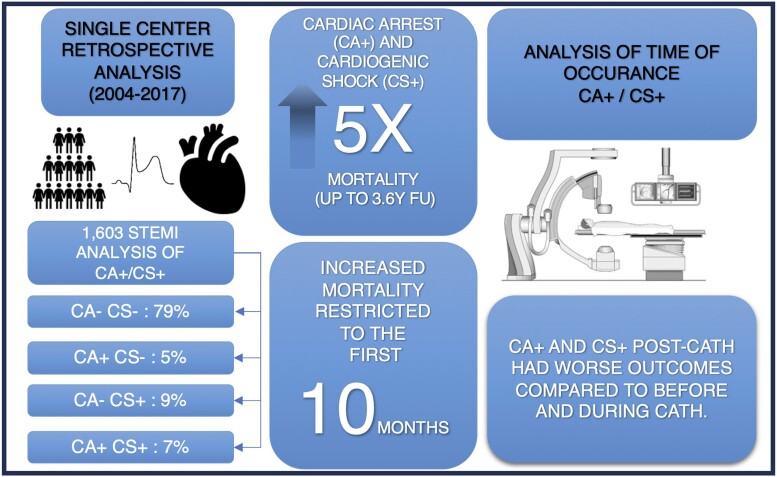
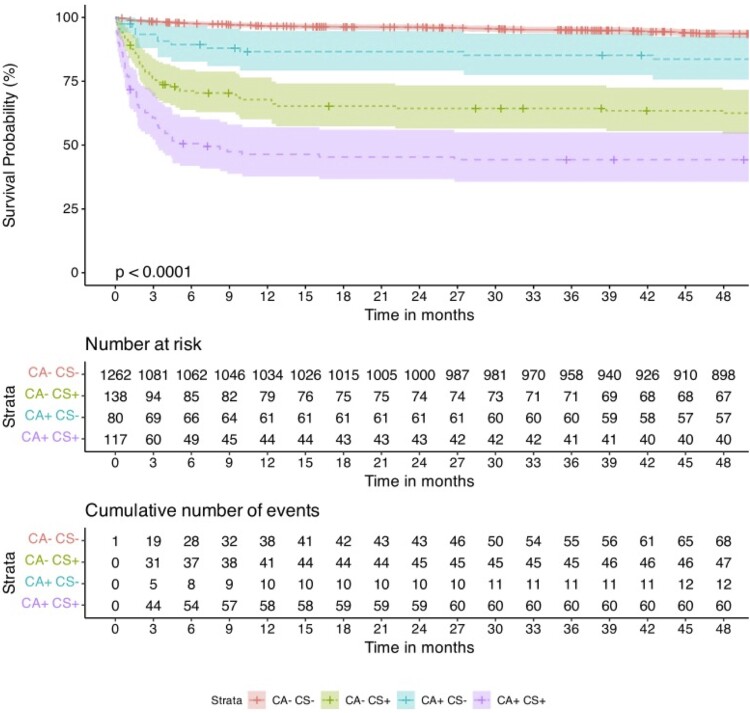
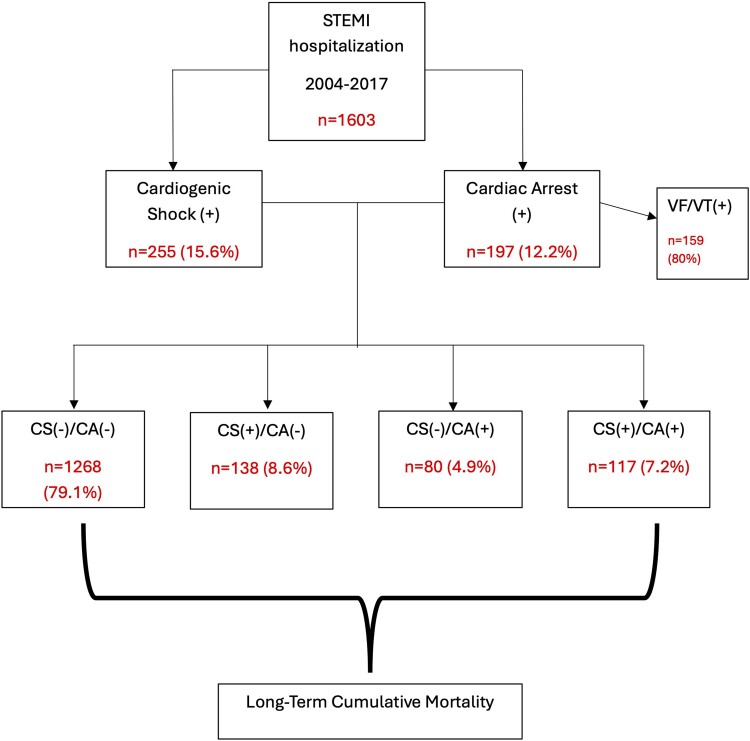
目的:心源性休克(CS)和心脏骤停(CA)是ST段抬高型心肌梗死(STEMI)患者的严重并发症,但缺乏根据其发生时间划分的长期数据。本研究旨在确定 STEMI 并发 CS 和 CA 的发生率、发生时间之间的关系以及长期随访对预后的影响:我们对 2004 年至 2017 年间接受治疗的 STEMI 患者进行了回顾性分析。根据既未发生 CA 也未发生 CS、仅发生 CA、仅发生 CS 以及同时发生 CA 和 CS(分别为 CA-CS-、CA+、CS+ 和 CA+CS+),将患者分为四组。调整后的 Cox 回归分析用于评估 CS 和 CA 类别与死亡率之间的独立关联。共对1603名STEMI患者进行了中位3.6年的随访。12.2%和15.9%的患者发生了CA和CS,这两种情况都会影响长期死亡率[调整后的危险比(HR)=2.59,95%置信区间(CI):1.53-4.41,P < 0.001;HR=3.16,95%置信区间(CI):2.21-4.53,P < 0.001]。CA+CS+发生率为7.3%,与死亡率升高的关系最为密切(调整后HR = 5.36;95% CI:3.80-7.55,P < 0.001)。通过使用 B-样条曲线的灵活参数模型,死亡率的增加仅限于最初的 10 个月。此外,除首次心导管检查期间的 CA 外(P < 0.183),所有时间段的总死亡率均较高(P < 0.001):结论:STEMI 患者并发 CS 和 CA 与较高的长期死亡率有关,尤其是在前 10 个月。任何时间段的CS+和CA+都会影响预后,但初次心导管检查时的CA+除外,不过由于患者人数相对较少,这一点还需要在今后更大规模的研究中得到证实。
Long-term outcomes of cardiogenic shock and cardiac arrest complicating ST-elevation myocardial infarction according to timing of occurrence.
Aims: Cardiogenic shock (CS) and cardiac arrest (CA) are serious complications in ST-elevation myocardial infarction (STEMI) patients, with lack of long-term data according to their timing of occurrence. This study sought to determine the incidence and relationship between the timing of occurrence and prognostic impact of CS and CA complicating STEMI in the long-term follow-up.
Methods and results: We conducted a retrospective analysis of consecutive STEMI patients treated between 2004 and 2017. Patients were divided into four groups based on the occurrence of neither CA nor CS, CA only, CS only, and both CA and CS (CA-CS-, CA+, CS+, and CA+CS+, respectively). Adjusted Cox regression analysis was used to assess the independent association between the CS and CA categories and mortality. A total of 1603 STEMI patients were followed for a median of 3.6 years. CA and CS occurred in the 12.2% and 15.9% of patients, and both impacted long-term mortality [adjusted hazard ratio (HR) = 2.59, 95% confidence interval (CI): 1.53-4.41, P < 0.001; HR = 3.16, 95% CI: 2.21-4.53, P < 0.001, respectively). CA+CS+ occurred in 7.3%, with the strongest association with higher mortality (adjusted HR = 5.36; 95% CI: 3.80-7.55, P < 0.001). Using flexible parametric models with B-splines, the increased mortality was restricted to the first ∼10 months. In addition, overall mortality rates were higher at all timings (all with P < 0.001), except for CA during initial cardiac catheterization (P < 0.183).
Conclusion: CS and CA complicating patients presenting with STEMI were associated with higher long-term mortality rate, especially in the first 10 months. Both CS+ and CA+ at any timeframe impacted outcomes, except for CA+ during the initial cardiac catheterization, although this will have to be confirmed in larger future studies, given the relatively small number of patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
