Anthony J Kanelidis, Michael J Randazzo, Sara Kalantari, Bryan Smith, Ann Nguyen, Ben B Chung, Stanley Swat, Nitasha Sarswat, Christopher Salerno, Valluvan Jeevanandam, Gene Kim, Mark N Belkin, Jonathan Grinstein
{"title":"动态评估心源性休克患者的左心室耦联和心肌储备。","authors":"Anthony J Kanelidis, Michael J Randazzo, Sara Kalantari, Bryan Smith, Ann Nguyen, Ben B Chung, Stanley Swat, Nitasha Sarswat, Christopher Salerno, Valluvan Jeevanandam, Gene Kim, Mark N Belkin, Jonathan Grinstein","doi":"10.1093/ehjopen/oeae072","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Pulmonary artery catheter haemodynamics are associated with improved survival in cardiogenic shock (CS). We investigated the utility of aortic pulsatility index (API) and cardiac power output (CPO) as surrogates for left ventricular (LV) coupling and myocardial reserve, respectively, in patients with CS undergoing dynamic assessment after a milrinone bolus.</p><p><strong>Methods and results: </strong>Patients with SCAI Stage C CS underwent a milrinone drug study (50 mcg/kg bolus infused over 10 min) to assess inotropic response. Haemodynamic measurements were obtained at baseline and following the bolus. Aortic pulsatility index and CPO were used to risk-stratify patients with the incidence of LV assist device (LVAD), orthotopic heart transplantation (OHT), or death at 1 year as the primary composite endpoint. Two hundred and twenty-four patients in SCAI Stage C CS underwent haemodynamics prior to milrinone bolus, and 117 patients had low baseline API < 1.45. Of the 117 patients, 88 had a final API < 2.2 after milrinone load, consistent with LV decoupling, in which 73% met the composite endpoint. The remaining 29 patients had a final API ≥ 2.2 consistent with LV recoupling, and only 55% met the composite endpoint (<i>P</i> = 0.046). Of the 117 patients, 40 patients had low myocardial reserve (final CPO < 0.77 W), in which 78% met the composite endpoint. Of the 77 patients who demonstrated myocardial reserve (final CPO ≥ 0.77 W), only 64% met the composite endpoint (<i>P</i> = 0.039).</p><p><strong>Conclusion: </strong>The use of API and CPO in a dynamic assessment after provocative testing led to improved risk stratification in patients with SCAI Stage C CS for clinical outcomes including LVAD, OHT, or death at 1 year.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 5","pages":"oeae072"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11425697/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dynamic assessment of left ventricular coupling and myocardial reserve in patients with cardiogenic shock.\",\"authors\":\"Anthony J Kanelidis, Michael J Randazzo, Sara Kalantari, Bryan Smith, Ann Nguyen, Ben B Chung, Stanley Swat, Nitasha Sarswat, Christopher Salerno, Valluvan Jeevanandam, Gene Kim, Mark N Belkin, Jonathan Grinstein\",\"doi\":\"10.1093/ehjopen/oeae072\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Pulmonary artery catheter haemodynamics are associated with improved survival in cardiogenic shock (CS). We investigated the utility of aortic pulsatility index (API) and cardiac power output (CPO) as surrogates for left ventricular (LV) coupling and myocardial reserve, respectively, in patients with CS undergoing dynamic assessment after a milrinone bolus.</p><p><strong>Methods and results: </strong>Patients with SCAI Stage C CS underwent a milrinone drug study (50 mcg/kg bolus infused over 10 min) to assess inotropic response. Haemodynamic measurements were obtained at baseline and following the bolus. Aortic pulsatility index and CPO were used to risk-stratify patients with the incidence of LV assist device (LVAD), orthotopic heart transplantation (OHT), or death at 1 year as the primary composite endpoint. Two hundred and twenty-four patients in SCAI Stage C CS underwent haemodynamics prior to milrinone bolus, and 117 patients had low baseline API < 1.45. Of the 117 patients, 88 had a final API < 2.2 after milrinone load, consistent with LV decoupling, in which 73% met the composite endpoint. The remaining 29 patients had a final API ≥ 2.2 consistent with LV recoupling, and only 55% met the composite endpoint (<i>P</i> = 0.046). Of the 117 patients, 40 patients had low myocardial reserve (final CPO < 0.77 W), in which 78% met the composite endpoint. Of the 77 patients who demonstrated myocardial reserve (final CPO ≥ 0.77 W), only 64% met the composite endpoint (<i>P</i> = 0.039).</p><p><strong>Conclusion: </strong>The use of API and CPO in a dynamic assessment after provocative testing led to improved risk stratification in patients with SCAI Stage C CS for clinical outcomes including LVAD, OHT, or death at 1 year.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"4 5\",\"pages\":\"oeae072\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11425697/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeae072\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Dynamic assessment of left ventricular coupling and myocardial reserve in patients with cardiogenic shock.
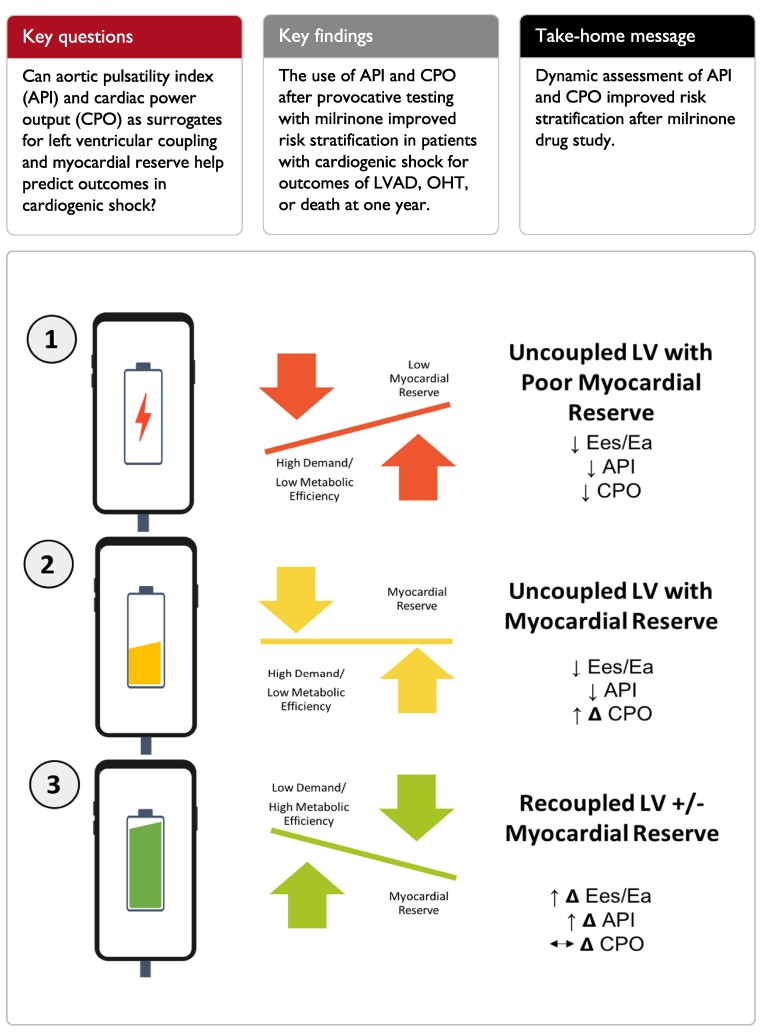
Aims: Pulmonary artery catheter haemodynamics are associated with improved survival in cardiogenic shock (CS). We investigated the utility of aortic pulsatility index (API) and cardiac power output (CPO) as surrogates for left ventricular (LV) coupling and myocardial reserve, respectively, in patients with CS undergoing dynamic assessment after a milrinone bolus.
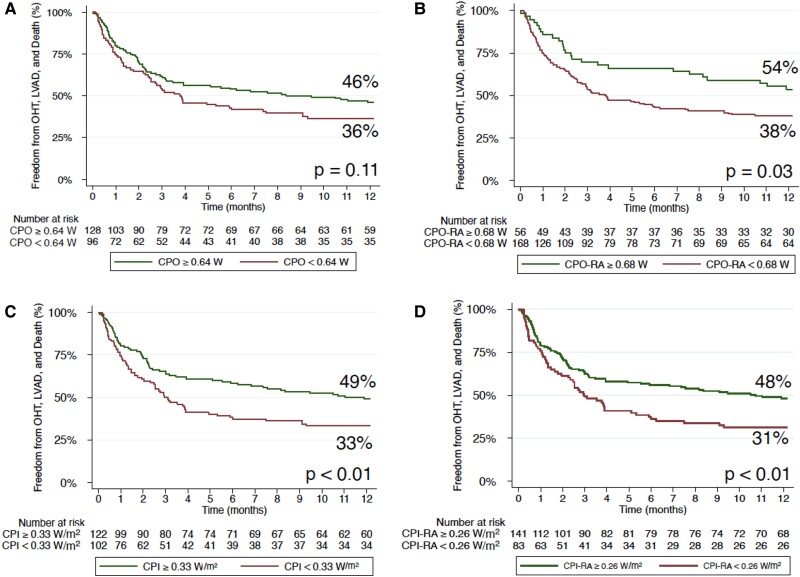
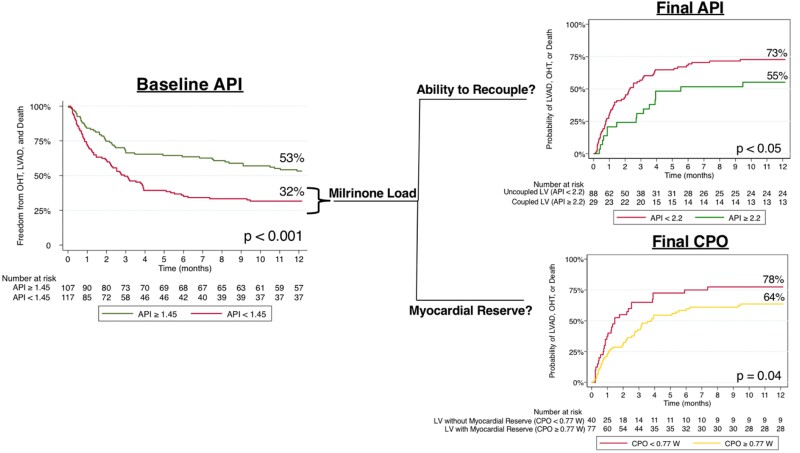
Methods and results: Patients with SCAI Stage C CS underwent a milrinone drug study (50 mcg/kg bolus infused over 10 min) to assess inotropic response. Haemodynamic measurements were obtained at baseline and following the bolus. Aortic pulsatility index and CPO were used to risk-stratify patients with the incidence of LV assist device (LVAD), orthotopic heart transplantation (OHT), or death at 1 year as the primary composite endpoint. Two hundred and twenty-four patients in SCAI Stage C CS underwent haemodynamics prior to milrinone bolus, and 117 patients had low baseline API < 1.45. Of the 117 patients, 88 had a final API < 2.2 after milrinone load, consistent with LV decoupling, in which 73% met the composite endpoint. The remaining 29 patients had a final API ≥ 2.2 consistent with LV recoupling, and only 55% met the composite endpoint (P = 0.046). Of the 117 patients, 40 patients had low myocardial reserve (final CPO < 0.77 W), in which 78% met the composite endpoint. Of the 77 patients who demonstrated myocardial reserve (final CPO ≥ 0.77 W), only 64% met the composite endpoint (P = 0.039).
Conclusion: The use of API and CPO in a dynamic assessment after provocative testing led to improved risk stratification in patients with SCAI Stage C CS for clinical outcomes including LVAD, OHT, or death at 1 year.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
