André Alexandre, David Sá-Couto, Mariana Brandão, Sofia Cabral, Tomás Fonseca, Rita Quelhas Costa, António Marinho, Carlos Vasconcelos, Betânia Ferreira, João Pedro Ferreira, Patrícia Rodrigues
{"title":"类风湿性关节炎亚临床左心室功能障碍:前瞻性 Porto-RA 队列的发现。","authors":"André Alexandre, David Sá-Couto, Mariana Brandão, Sofia Cabral, Tomás Fonseca, Rita Quelhas Costa, António Marinho, Carlos Vasconcelos, Betânia Ferreira, João Pedro Ferreira, Patrícia Rodrigues","doi":"10.1007/s00392-024-02548-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Patients with rheumatoid arthritis (RA) have an increased risk of cardiac dysfunction and heart failure (HF) due to a pro-inflammatory state. Detecting cardiac dysfunction in RA is challenging as these patients often present preserved ejection fraction (EF) but may have subclinical ventricular dysfunction. Echocardiographic strain analysis is a promising tool for early detection of subclinical left ventricular systolic dysfunction (LVSD). This study assesses the prognostic role of strain analysis in RA.</p><p><strong>Methods and results: </strong>Prospective study of 277 RA patients without known heart disease and preserved EF, categorized by left ventricular global longitudinal strain (GLS): normal GLS (≤ - 18%) vs. subclinical LVSD (> - 18%). Primary outcome was a composite of myocardial infarction, HF hospitalization, stroke, or cardiovascular death (MACE). Mean age was 57 years, 79% female. Although mean GLS was within normal (- 20 ± 3%), subclinical LVSD was observed in 24% of patients (n = 67) and was positively correlated with older age (OR 1.54 per 10 years; p < 0.001) and comorbid conditions, such as dyslipidemia (OR 2.27; p = 0.004), obesity (OR 2.29; p = 0.015), and chronic kidney disease (OR 8.39; p = 0.012). Subclinical LVSD was independently associated with a 3.9-fold higher risk of MACE (p = 0.003) and a 3.4-fold higher risk of HF hospitalization/cardiovascular death (p = 0.041). A GLS threshold of > - 18.5% provided optimal sensitivity (78%) and specificity (74%) in identifying patients at elevated MACE risk (AUC = 0.78; p < 0.001).</p><p><strong>Conclusion: </strong>Subclinical LVSD, identified by reduced GLS, was strongly associated with adverse cardiovascular events in RA. Whether these findings have therapeutic implications is worth exploring in clinical trials.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"1191-1203"},"PeriodicalIF":3.4000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408714/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subclinical left ventricular dysfunction in rheumatoid arthritis: findings from the prospective Porto-RA cohort.\",\"authors\":\"André Alexandre, David Sá-Couto, Mariana Brandão, Sofia Cabral, Tomás Fonseca, Rita Quelhas Costa, António Marinho, Carlos Vasconcelos, Betânia Ferreira, João Pedro Ferreira, Patrícia Rodrigues\",\"doi\":\"10.1007/s00392-024-02548-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>Patients with rheumatoid arthritis (RA) have an increased risk of cardiac dysfunction and heart failure (HF) due to a pro-inflammatory state. Detecting cardiac dysfunction in RA is challenging as these patients often present preserved ejection fraction (EF) but may have subclinical ventricular dysfunction. Echocardiographic strain analysis is a promising tool for early detection of subclinical left ventricular systolic dysfunction (LVSD). This study assesses the prognostic role of strain analysis in RA.</p><p><strong>Methods and results: </strong>Prospective study of 277 RA patients without known heart disease and preserved EF, categorized by left ventricular global longitudinal strain (GLS): normal GLS (≤ - 18%) vs. subclinical LVSD (> - 18%). Primary outcome was a composite of myocardial infarction, HF hospitalization, stroke, or cardiovascular death (MACE). Mean age was 57 years, 79% female. Although mean GLS was within normal (- 20 ± 3%), subclinical LVSD was observed in 24% of patients (n = 67) and was positively correlated with older age (OR 1.54 per 10 years; p < 0.001) and comorbid conditions, such as dyslipidemia (OR 2.27; p = 0.004), obesity (OR 2.29; p = 0.015), and chronic kidney disease (OR 8.39; p = 0.012). Subclinical LVSD was independently associated with a 3.9-fold higher risk of MACE (p = 0.003) and a 3.4-fold higher risk of HF hospitalization/cardiovascular death (p = 0.041). A GLS threshold of > - 18.5% provided optimal sensitivity (78%) and specificity (74%) in identifying patients at elevated MACE risk (AUC = 0.78; p < 0.001).</p><p><strong>Conclusion: </strong>Subclinical LVSD, identified by reduced GLS, was strongly associated with adverse cardiovascular events in RA. Whether these findings have therapeutic implications is worth exploring in clinical trials.</p>\",\"PeriodicalId\":10474,\"journal\":{\"name\":\"Clinical Research in Cardiology\",\"volume\":\" \",\"pages\":\"1191-1203\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Research in Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00392-024-02548-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02548-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:类风湿性关节炎(RA)患者由于处于促炎症状态,发生心功能障碍和心力衰竭(HF)的风险增加。检测类风湿性关节炎患者的心功能障碍具有挑战性,因为这些患者通常表现为射血分数(EF)保留,但可能存在亚临床心室功能障碍。超声心动图应变分析是早期检测亚临床左心室收缩功能障碍(LVSD)的有效工具。本研究评估了应变分析在 RA 中的预后作用:前瞻性研究对象为277例无已知心脏病且EF保留的RA患者,根据左心室整体纵向应变(GLS)进行分类:正常GLS(≤ - 18%)与亚临床LVSD(> - 18%)。主要结果是心肌梗死、高血压住院、中风或心血管死亡的复合结果(MACE)。平均年龄为 57 岁,79% 为女性。虽然平均 GLS 在正常范围内(- 20 ± 3%),但在 24% 的患者(n = 67)中观察到了亚临床 LVSD,且与年龄呈正相关(OR 1.54 per 10 years; p - 18.5%),为识别 MACE 风险升高的患者提供了最佳的灵敏度(78%)和特异度(74%)(AUC = 0.78; p 结论:亚临床 LVSD 与年龄呈正相关(OR 1.54 per 10 years; p - 18.5%),为识别 MACE 风险升高的患者提供了最佳的灵敏度(78%)和特异度(74%):通过 GLS 降低确定的亚临床 LVSD 与 RA 患者的不良心血管事件密切相关。这些发现是否具有治疗意义值得在临床试验中探讨。
Subclinical left ventricular dysfunction in rheumatoid arthritis: findings from the prospective Porto-RA cohort.
Aim: Patients with rheumatoid arthritis (RA) have an increased risk of cardiac dysfunction and heart failure (HF) due to a pro-inflammatory state. Detecting cardiac dysfunction in RA is challenging as these patients often present preserved ejection fraction (EF) but may have subclinical ventricular dysfunction. Echocardiographic strain analysis is a promising tool for early detection of subclinical left ventricular systolic dysfunction (LVSD). This study assesses the prognostic role of strain analysis in RA.
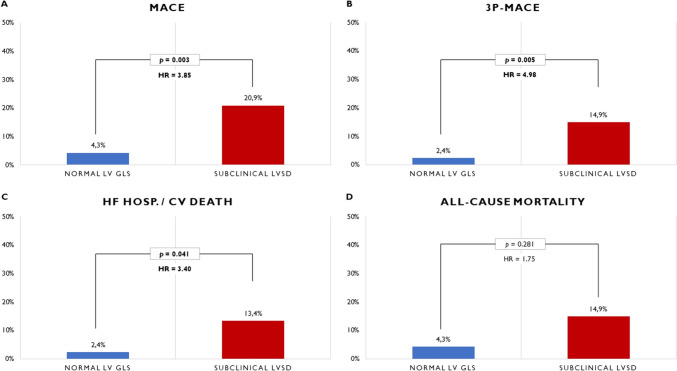
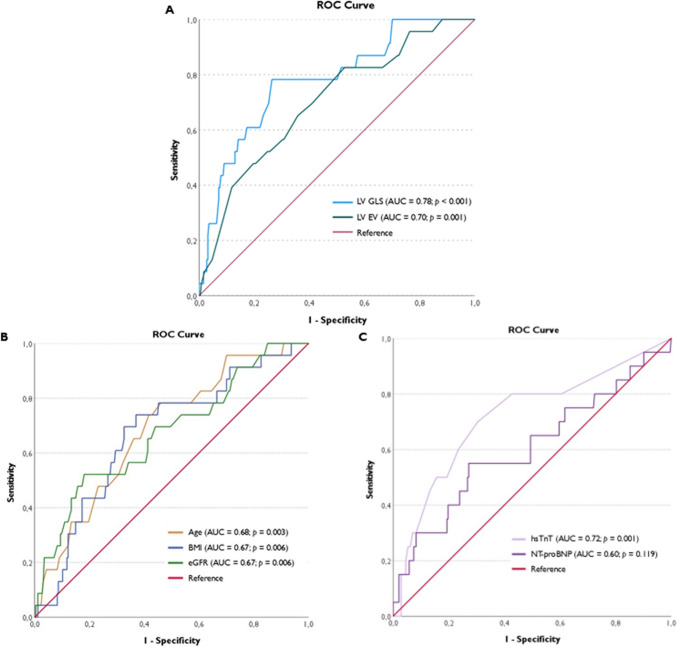
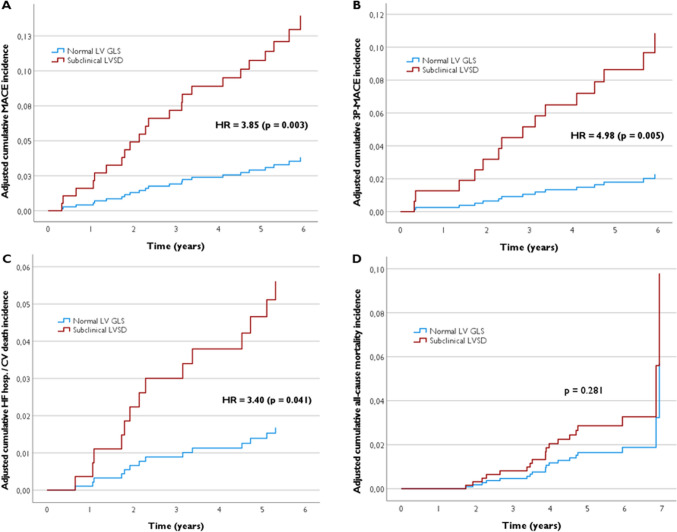
Methods and results: Prospective study of 277 RA patients without known heart disease and preserved EF, categorized by left ventricular global longitudinal strain (GLS): normal GLS (≤ - 18%) vs. subclinical LVSD (> - 18%). Primary outcome was a composite of myocardial infarction, HF hospitalization, stroke, or cardiovascular death (MACE). Mean age was 57 years, 79% female. Although mean GLS was within normal (- 20 ± 3%), subclinical LVSD was observed in 24% of patients (n = 67) and was positively correlated with older age (OR 1.54 per 10 years; p < 0.001) and comorbid conditions, such as dyslipidemia (OR 2.27; p = 0.004), obesity (OR 2.29; p = 0.015), and chronic kidney disease (OR 8.39; p = 0.012). Subclinical LVSD was independently associated with a 3.9-fold higher risk of MACE (p = 0.003) and a 3.4-fold higher risk of HF hospitalization/cardiovascular death (p = 0.041). A GLS threshold of > - 18.5% provided optimal sensitivity (78%) and specificity (74%) in identifying patients at elevated MACE risk (AUC = 0.78; p < 0.001).
Conclusion: Subclinical LVSD, identified by reduced GLS, was strongly associated with adverse cardiovascular events in RA. Whether these findings have therapeutic implications is worth exploring in clinical trials.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
