Augusto Cama-Olivares, Tianqi Ouyang, Tomonori Takeuchi, Shelsea A St Hillien, Jevon E Robinson, Raymond T Chung, Giuseppe Cullaro, Constantine J Karvellas, Josh Levitsky, Eric S Orman, Kavish R Patidar, Kevin R Regner, Danielle L Saly, Deirdre Sawinski, Pratima Sharma, J Pedro Teixeira, Nneka N Ufere, Juan Carlos Q Velez, Hani M Wadei, Nabeel Wahid, Andrew S Allegretti, Javier A Neyra, Justin M Belcher
{"title":"HRS-AKI 与需要肾脏替代治疗的肝硬化患者死亡率的关系:HRS-HARMONY 联合会的研究结果。","authors":"Augusto Cama-Olivares, Tianqi Ouyang, Tomonori Takeuchi, Shelsea A St Hillien, Jevon E Robinson, Raymond T Chung, Giuseppe Cullaro, Constantine J Karvellas, Josh Levitsky, Eric S Orman, Kavish R Patidar, Kevin R Regner, Danielle L Saly, Deirdre Sawinski, Pratima Sharma, J Pedro Teixeira, Nneka N Ufere, Juan Carlos Q Velez, Hani M Wadei, Nabeel Wahid, Andrew S Allegretti, Javier A Neyra, Justin M Belcher","doi":"10.34067/KID.0000000589","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":17882,"journal":{"name":"Kidney360","volume":" ","pages":"247-256"},"PeriodicalIF":3.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11882256/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of Hepatorenal Syndrome-Acute Kidney Injury with Mortality in Patients with Cirrhosis Requiring Renal Replacement Therapy: Results from the HRS-HARMONY Consortium.\",\"authors\":\"Augusto Cama-Olivares, Tianqi Ouyang, Tomonori Takeuchi, Shelsea A St Hillien, Jevon E Robinson, Raymond T Chung, Giuseppe Cullaro, Constantine J Karvellas, Josh Levitsky, Eric S Orman, Kavish R Patidar, Kevin R Regner, Danielle L Saly, Deirdre Sawinski, Pratima Sharma, J Pedro Teixeira, Nneka N Ufere, Juan Carlos Q Velez, Hani M Wadei, Nabeel Wahid, Andrew S Allegretti, Javier A Neyra, Justin M Belcher\",\"doi\":\"10.34067/KID.0000000589\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"\",\"PeriodicalId\":17882,\"journal\":{\"name\":\"Kidney360\",\"volume\":\" \",\"pages\":\"247-256\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11882256/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.34067/KID.0000000589\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34067/KID.0000000589","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
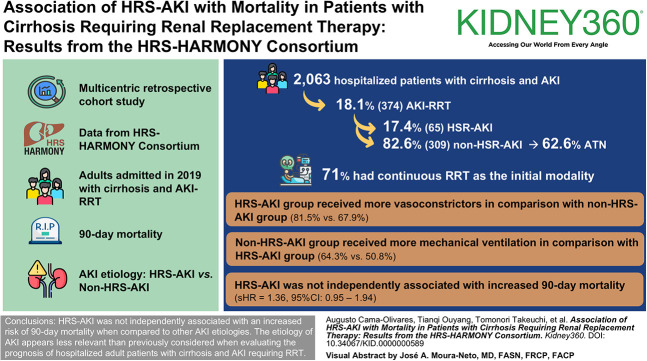
Association of Hepatorenal Syndrome-Acute Kidney Injury with Mortality in Patients with Cirrhosis Requiring Renal Replacement Therapy: Results from the HRS-HARMONY Consortium.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
