{"title":"两个儿童期缓慢进展的胰岛素依赖型糖尿病病例的内源性胰岛素分泌能力和抗胰岛自身抗体滴度的变化趋势。","authors":"Dai Suzuki, Hirohito Shima, Sayaka Kawashima, Miki Kamimura, Atsuo Kikuchi, Junko Kanno","doi":"10.1297/cpe.2024-0039","DOIUrl":null,"url":null,"abstract":"<p><p>Slowly progressive insulin-dependent (type 1) diabetes mellitus (SPIDDM) is a subtype of type 1 diabetes. Although SPIDDM is not rare among Japanese children, there are few reports on endogenous insulin secretory capacity and anti-pancreatic islet autoantibodies in pediatric SPIDDM. We followed the trends in endogenous insulin secretory capacity and anti-pancreatic islet autoantibody titers in two pediatric SPIDDM cases over several years. Case 1 developed insulin deficiency eight months after diabetes diagnosis; as her insulinoma-associated antibody test result was positive, insulin therapy was initiated. Fourteen months after the diagnosis, she tested positive for glutamic acid decarboxylase autoantibodies (GADA) and was diagnosed with SPIDDM. Case 2 was mildly positive for GADA at the onset of diabetes, but became a high titer during the course of the disease. Fourteen months after the diagnosis of diabetes, he became mildly insulin deficient, and insulin therapy was initiated. However, his insulin secretory capacity was preserved for 60 mo after the onset. SPIDDM is generally indistinguishable from type 2 diabetes at diagnosis; therefore, repeated evaluation of the insulin secretory capacity and anti-islet autoantibodies facilitates early diagnosis and appropriate treatment, especially in nonobese children with type 2 diabetes.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":"33 4","pages":"238-243"},"PeriodicalIF":1.2000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11442699/pdf/","citationCount":"0","resultStr":"{\"title\":\"Trends in endogenous insulin secretion capacity and anti-islet autoantibody titers in two childhood-onset slowly progressive insulin-dependent diabetes mellitus cases.\",\"authors\":\"Dai Suzuki, Hirohito Shima, Sayaka Kawashima, Miki Kamimura, Atsuo Kikuchi, Junko Kanno\",\"doi\":\"10.1297/cpe.2024-0039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Slowly progressive insulin-dependent (type 1) diabetes mellitus (SPIDDM) is a subtype of type 1 diabetes. Although SPIDDM is not rare among Japanese children, there are few reports on endogenous insulin secretory capacity and anti-pancreatic islet autoantibodies in pediatric SPIDDM. We followed the trends in endogenous insulin secretory capacity and anti-pancreatic islet autoantibody titers in two pediatric SPIDDM cases over several years. Case 1 developed insulin deficiency eight months after diabetes diagnosis; as her insulinoma-associated antibody test result was positive, insulin therapy was initiated. Fourteen months after the diagnosis, she tested positive for glutamic acid decarboxylase autoantibodies (GADA) and was diagnosed with SPIDDM. Case 2 was mildly positive for GADA at the onset of diabetes, but became a high titer during the course of the disease. Fourteen months after the diagnosis of diabetes, he became mildly insulin deficient, and insulin therapy was initiated. However, his insulin secretory capacity was preserved for 60 mo after the onset. SPIDDM is generally indistinguishable from type 2 diabetes at diagnosis; therefore, repeated evaluation of the insulin secretory capacity and anti-islet autoantibodies facilitates early diagnosis and appropriate treatment, especially in nonobese children with type 2 diabetes.</p>\",\"PeriodicalId\":10678,\"journal\":{\"name\":\"Clinical Pediatric Endocrinology\",\"volume\":\"33 4\",\"pages\":\"238-243\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11442699/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pediatric Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1297/cpe.2024-0039\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2024-0039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/13 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Trends in endogenous insulin secretion capacity and anti-islet autoantibody titers in two childhood-onset slowly progressive insulin-dependent diabetes mellitus cases.
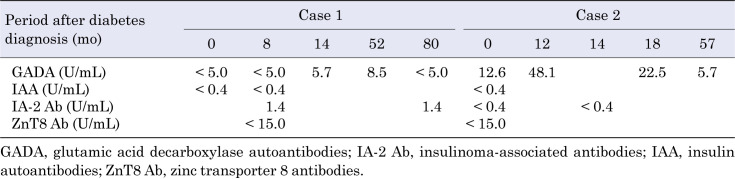
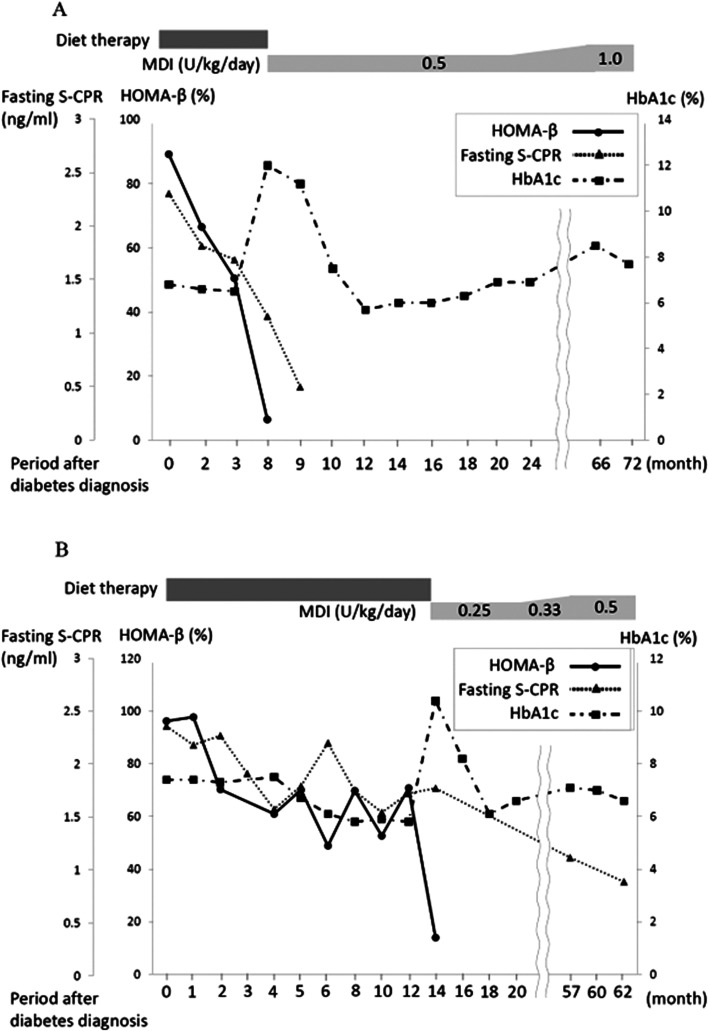
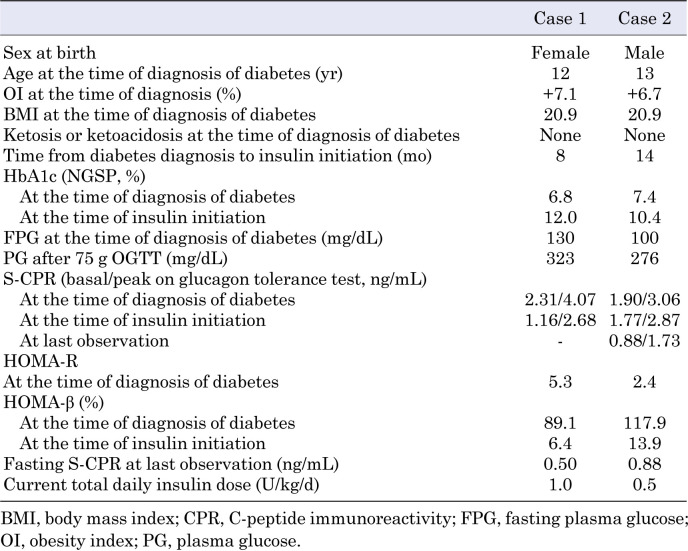
Slowly progressive insulin-dependent (type 1) diabetes mellitus (SPIDDM) is a subtype of type 1 diabetes. Although SPIDDM is not rare among Japanese children, there are few reports on endogenous insulin secretory capacity and anti-pancreatic islet autoantibodies in pediatric SPIDDM. We followed the trends in endogenous insulin secretory capacity and anti-pancreatic islet autoantibody titers in two pediatric SPIDDM cases over several years. Case 1 developed insulin deficiency eight months after diabetes diagnosis; as her insulinoma-associated antibody test result was positive, insulin therapy was initiated. Fourteen months after the diagnosis, she tested positive for glutamic acid decarboxylase autoantibodies (GADA) and was diagnosed with SPIDDM. Case 2 was mildly positive for GADA at the onset of diabetes, but became a high titer during the course of the disease. Fourteen months after the diagnosis of diabetes, he became mildly insulin deficient, and insulin therapy was initiated. However, his insulin secretory capacity was preserved for 60 mo after the onset. SPIDDM is generally indistinguishable from type 2 diabetes at diagnosis; therefore, repeated evaluation of the insulin secretory capacity and anti-islet autoantibodies facilitates early diagnosis and appropriate treatment, especially in nonobese children with type 2 diabetes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
