J McGee, A McClure, S Ilnitsky, A Vilos, B Abu-Rafea, G Vilos
{"title":"安大略省子宫内膜消融术后的子宫切除率:对 76,446 名患者的队列分析。","authors":"J McGee, A McClure, S Ilnitsky, A Vilos, B Abu-Rafea, G Vilos","doi":"10.52054/FVVO.13.3.028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endometrial Ablation (EA) is an alternative to hysterectomy for the management of abnormal uterine bleeding (AUB); however, it does not eliminate the need for future surgical re-intervention.</p><p><strong>Objectives: </strong>The primary objective of this study was to establish long-term clinical outcomes including the risk of hysterectomy in women who had undergone a primary EA.</p><p><strong>Materials and methods: </strong>This is a retrospective population-based cohort study utilising administrative data from the Canadian province of Ontario. This study assesses patients undergoing surgery in a publicly funded health care system.</p><p><strong>Main outcome measures: </strong>We assessed women in Ontario undergoing a primary EA over a 15-year period. The primary outcome was hysterectomy within 5 years of primary EA. Secondary outcomes included myomectomy and repeat EA. All outcomes were also reported for 1, 3, 5, 10 and 15 years of follow-up. Logistic regression was used to establish predictors of hysterectomy within 5 years of primary EA.</p><p><strong>Results: </strong>A total of 76,446 primary EAs were evaluated from 2002-2017, with 16,480 (21.56%) undergoing a subsequent surgical intervention. The average age of primary EA was 43.8 (+/- 6.3) years. Within 5 years, the evaluable cohort was 52,464, with 8,635 (16.46%) of women having proceeded to hysterectomy, 664 (1.27%) to myomectomy, and 2,468 (2.8%) to repeat ablation. By 15-years follow-up, the evaluable cohort was 1,788, with 28.75% had undergone a hysterectomy, 2.01% a myomectomy, and 5.20% a repeat EA. On logistic regression analysis, advancing age at time of EA was associated with significantly decreased odds of hysterectomy (OR=0.94, 95% CI 0.935-0.944, p<.0001) as was increasing surgical experience (OR=0.997, 95% CI 0.994-1.000, p=.022). Conversely, complex diagnosis (OR=1.102, 95% CI 1.042-1.164, p<.0001) and previous abdominal surgery (OR=1.288, 95% CI 1.222-1.357, p<0.0001) were associated with increased risk of subsequent hysterectomy.</p><p><strong>Conclusion: </strong>Primary EA is associated with a high risk of progression to subsequent hysterectomy or other surgical intervention, without evidence of plateau of risk with long term follow-up.</p><p><strong>What is new?: </strong>This study has the longest follow-up assessing hysterectomy outcomes in women undergoing a primary EA, with 28.75% of women having undergone a hysterectomy within 15 years of their EA.</p>","PeriodicalId":46400,"journal":{"name":"Facts Views and Vision in ObGyn","volume":"16 3","pages":"311-316"},"PeriodicalIF":1.4000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11569427/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hysterectomy Rate Following Endometrial Ablation in Ontario: A Cohort Analysis of 76,446 Patients.\",\"authors\":\"J McGee, A McClure, S Ilnitsky, A Vilos, B Abu-Rafea, G Vilos\",\"doi\":\"10.52054/FVVO.13.3.028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Endometrial Ablation (EA) is an alternative to hysterectomy for the management of abnormal uterine bleeding (AUB); however, it does not eliminate the need for future surgical re-intervention.</p><p><strong>Objectives: </strong>The primary objective of this study was to establish long-term clinical outcomes including the risk of hysterectomy in women who had undergone a primary EA.</p><p><strong>Materials and methods: </strong>This is a retrospective population-based cohort study utilising administrative data from the Canadian province of Ontario. This study assesses patients undergoing surgery in a publicly funded health care system.</p><p><strong>Main outcome measures: </strong>We assessed women in Ontario undergoing a primary EA over a 15-year period. The primary outcome was hysterectomy within 5 years of primary EA. Secondary outcomes included myomectomy and repeat EA. All outcomes were also reported for 1, 3, 5, 10 and 15 years of follow-up. Logistic regression was used to establish predictors of hysterectomy within 5 years of primary EA.</p><p><strong>Results: </strong>A total of 76,446 primary EAs were evaluated from 2002-2017, with 16,480 (21.56%) undergoing a subsequent surgical intervention. The average age of primary EA was 43.8 (+/- 6.3) years. Within 5 years, the evaluable cohort was 52,464, with 8,635 (16.46%) of women having proceeded to hysterectomy, 664 (1.27%) to myomectomy, and 2,468 (2.8%) to repeat ablation. By 15-years follow-up, the evaluable cohort was 1,788, with 28.75% had undergone a hysterectomy, 2.01% a myomectomy, and 5.20% a repeat EA. On logistic regression analysis, advancing age at time of EA was associated with significantly decreased odds of hysterectomy (OR=0.94, 95% CI 0.935-0.944, p<.0001) as was increasing surgical experience (OR=0.997, 95% CI 0.994-1.000, p=.022). Conversely, complex diagnosis (OR=1.102, 95% CI 1.042-1.164, p<.0001) and previous abdominal surgery (OR=1.288, 95% CI 1.222-1.357, p<0.0001) were associated with increased risk of subsequent hysterectomy.</p><p><strong>Conclusion: </strong>Primary EA is associated with a high risk of progression to subsequent hysterectomy or other surgical intervention, without evidence of plateau of risk with long term follow-up.</p><p><strong>What is new?: </strong>This study has the longest follow-up assessing hysterectomy outcomes in women undergoing a primary EA, with 28.75% of women having undergone a hysterectomy within 15 years of their EA.</p>\",\"PeriodicalId\":46400,\"journal\":{\"name\":\"Facts Views and Vision in ObGyn\",\"volume\":\"16 3\",\"pages\":\"311-316\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11569427/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Facts Views and Vision in ObGyn\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.52054/FVVO.13.3.028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Facts Views and Vision in ObGyn","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52054/FVVO.13.3.028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:子宫内膜消融术(EA)是治疗异常子宫出血(AUB)的子宫切除术的替代疗法,但它并不能消除将来再次手术干预的需要:本研究的主要目的是确定接受过初级 EA 的妇女的长期临床结果,包括子宫切除术的风险:这是一项基于人群的回顾性队列研究,利用的是加拿大安大略省的行政数据。这项研究评估了在公共医疗保健系统中接受手术的患者:我们对安大略省 15 年间接受初级 EA 的妇女进行了评估。主要结果是接受初级 EA 后 5 年内的子宫切除术。次要结果包括子宫肌瘤切除术和重复 EA。所有结果还报告了 1、3、5、10 和 15 年的随访情况。逻辑回归用于确定原发性 EA 5 年内子宫切除术的预测因素:2002-2017年间,共评估了76446例原发性EA,其中16480例(21.56%)接受了后续手术干预。原发性 EA 的平均年龄为 43.8 (+/- 6.3)岁。5 年内,可评估队列为 52,464 人,其中 8,635 人(16.46%)接受了子宫切除术,664 人(1.27%)接受了肌瘤切除术,2,468 人(2.8%)接受了重复消融术。在 15 年的随访中,可评估组群共有 1,788 人,其中 28.75% 接受了子宫切除术,2.01% 接受了子宫肌瘤切除术,5.20% 重复接受了 EA。在逻辑回归分析中,EA发生时年龄的增加与子宫切除术几率的显著降低有关(OR=0.94,95% CI 0.935-0.944,p):原发性EA与随后进展为子宫切除术或其他手术干预的高风险相关,但长期随访无证据显示风险趋于平稳:该研究对接受原发性EA的妇女进行了最长时间的随访,评估了子宫切除术的结果,其中28.75%的妇女在接受EA后15年内接受了子宫切除术。
Hysterectomy Rate Following Endometrial Ablation in Ontario: A Cohort Analysis of 76,446 Patients.
Background: Endometrial Ablation (EA) is an alternative to hysterectomy for the management of abnormal uterine bleeding (AUB); however, it does not eliminate the need for future surgical re-intervention.
Objectives: The primary objective of this study was to establish long-term clinical outcomes including the risk of hysterectomy in women who had undergone a primary EA.
Materials and methods: This is a retrospective population-based cohort study utilising administrative data from the Canadian province of Ontario. This study assesses patients undergoing surgery in a publicly funded health care system.
Main outcome measures: We assessed women in Ontario undergoing a primary EA over a 15-year period. The primary outcome was hysterectomy within 5 years of primary EA. Secondary outcomes included myomectomy and repeat EA. All outcomes were also reported for 1, 3, 5, 10 and 15 years of follow-up. Logistic regression was used to establish predictors of hysterectomy within 5 years of primary EA.
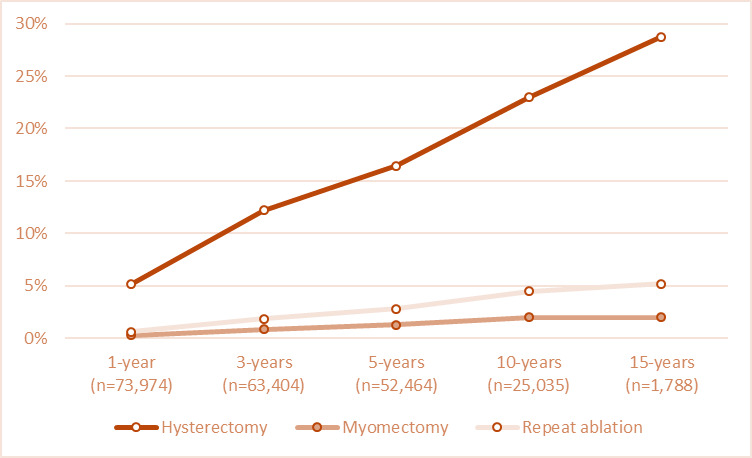
Results: A total of 76,446 primary EAs were evaluated from 2002-2017, with 16,480 (21.56%) undergoing a subsequent surgical intervention. The average age of primary EA was 43.8 (+/- 6.3) years. Within 5 years, the evaluable cohort was 52,464, with 8,635 (16.46%) of women having proceeded to hysterectomy, 664 (1.27%) to myomectomy, and 2,468 (2.8%) to repeat ablation. By 15-years follow-up, the evaluable cohort was 1,788, with 28.75% had undergone a hysterectomy, 2.01% a myomectomy, and 5.20% a repeat EA. On logistic regression analysis, advancing age at time of EA was associated with significantly decreased odds of hysterectomy (OR=0.94, 95% CI 0.935-0.944, p<.0001) as was increasing surgical experience (OR=0.997, 95% CI 0.994-1.000, p=.022). Conversely, complex diagnosis (OR=1.102, 95% CI 1.042-1.164, p<.0001) and previous abdominal surgery (OR=1.288, 95% CI 1.222-1.357, p<0.0001) were associated with increased risk of subsequent hysterectomy.
Conclusion: Primary EA is associated with a high risk of progression to subsequent hysterectomy or other surgical intervention, without evidence of plateau of risk with long term follow-up.
What is new?: This study has the longest follow-up assessing hysterectomy outcomes in women undergoing a primary EA, with 28.75% of women having undergone a hysterectomy within 15 years of their EA.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
