Raj Sahajanandan, A V Varsha, Vinay M Rao, Ben B Kurien, Korah Kuruvilla, Roy Thankachen, Madhu A Philip
{"title":"探索心脏外科重症监护室中的累犯问题:这种理解能否改善患者的治疗效果?","authors":"Raj Sahajanandan, A V Varsha, Vinay M Rao, Ben B Kurien, Korah Kuruvilla, Roy Thankachen, Madhu A Philip","doi":"10.4103/aca.aca_68_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The need for reinstitution of intensive care unit (ICU) care (\"recidivism\") in post-cardiac surgery patients is associated with increased morbidity, mortality, resource use, and healthcare costs. Recidivism is propounded as a quality indicator of ICU care. There is a paucity of studies from India regarding cardiac surgical ICU readmissions, their outcomes, and risk factors.</p><p><strong>Methods: </strong>Nested case-control study including 1,711 consecutive adult patients who underwent cardiac surgery over a two-year period at a tertiary care institute. The patients were grouped into recidival (R) and control (C) groups. The reasons for readmission, outcomes, and predictive risk factors were analyzed.</p><p><strong>Results: </strong>Fifty-four of 1,711 (3.1%) patients were readmitted to ICU, main reasons being cardiac arrhythmias (24, 41%), pericardial effusion (9, 15.2%), and infection (8, 13.5%). Readmission was significantly higher for valvular interventions (39 patients, 24.3%, mitral valve 25 patients) than coronary artery bypass grafting (13, 10.6%), P value 0.003*. On multivariate analysis, EuroSCORE 2 (>5), age, surgical reexploration, postoperative pulmonary complications, and infections were independently associated with a need for ICU readmission. The mortality rate among the readmitted patients was 7.4% compared to 1.4% overall mortality. The mean total postoperative length of stay was significantly longer for recidival patients (17.6 ± 14 days vs 7.6 ± 2.4 days; P < 0.0001).</p><p><strong>Conclusions: </strong>Recidivism is associated with longer hospital stay, suboptimal outcomes as well higher risk of mortality. Postoperative cardiac dysrhythmia was the most common cause of recidivism in our cohort. Early identification of patients at risk for recidivism and timely management of cardiopulmonary complications can translate to better outcomes.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"27 4","pages":"330-336"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11610776/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploring Recidivism in Cardiac Surgical ICU: Can this Understanding Translate to Enhanced Patient Outcomes?\",\"authors\":\"Raj Sahajanandan, A V Varsha, Vinay M Rao, Ben B Kurien, Korah Kuruvilla, Roy Thankachen, Madhu A Philip\",\"doi\":\"10.4103/aca.aca_68_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The need for reinstitution of intensive care unit (ICU) care (\\\"recidivism\\\") in post-cardiac surgery patients is associated with increased morbidity, mortality, resource use, and healthcare costs. Recidivism is propounded as a quality indicator of ICU care. There is a paucity of studies from India regarding cardiac surgical ICU readmissions, their outcomes, and risk factors.</p><p><strong>Methods: </strong>Nested case-control study including 1,711 consecutive adult patients who underwent cardiac surgery over a two-year period at a tertiary care institute. The patients were grouped into recidival (R) and control (C) groups. The reasons for readmission, outcomes, and predictive risk factors were analyzed.</p><p><strong>Results: </strong>Fifty-four of 1,711 (3.1%) patients were readmitted to ICU, main reasons being cardiac arrhythmias (24, 41%), pericardial effusion (9, 15.2%), and infection (8, 13.5%). Readmission was significantly higher for valvular interventions (39 patients, 24.3%, mitral valve 25 patients) than coronary artery bypass grafting (13, 10.6%), P value 0.003*. On multivariate analysis, EuroSCORE 2 (>5), age, surgical reexploration, postoperative pulmonary complications, and infections were independently associated with a need for ICU readmission. The mortality rate among the readmitted patients was 7.4% compared to 1.4% overall mortality. The mean total postoperative length of stay was significantly longer for recidival patients (17.6 ± 14 days vs 7.6 ± 2.4 days; P < 0.0001).</p><p><strong>Conclusions: </strong>Recidivism is associated with longer hospital stay, suboptimal outcomes as well higher risk of mortality. Postoperative cardiac dysrhythmia was the most common cause of recidivism in our cohort. Early identification of patients at risk for recidivism and timely management of cardiopulmonary complications can translate to better outcomes.</p>\",\"PeriodicalId\":7997,\"journal\":{\"name\":\"Annals of Cardiac Anaesthesia\",\"volume\":\"27 4\",\"pages\":\"330-336\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11610776/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Cardiac Anaesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/aca.aca_68_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_68_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Exploring Recidivism in Cardiac Surgical ICU: Can this Understanding Translate to Enhanced Patient Outcomes?
Objective: The need for reinstitution of intensive care unit (ICU) care ("recidivism") in post-cardiac surgery patients is associated with increased morbidity, mortality, resource use, and healthcare costs. Recidivism is propounded as a quality indicator of ICU care. There is a paucity of studies from India regarding cardiac surgical ICU readmissions, their outcomes, and risk factors.
Methods: Nested case-control study including 1,711 consecutive adult patients who underwent cardiac surgery over a two-year period at a tertiary care institute. The patients were grouped into recidival (R) and control (C) groups. The reasons for readmission, outcomes, and predictive risk factors were analyzed.
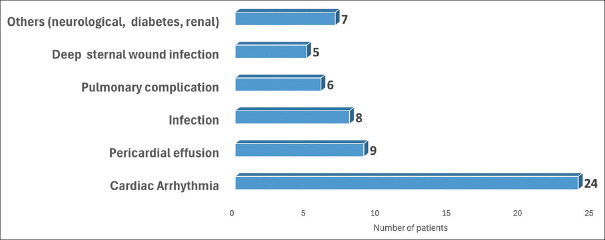
Results: Fifty-four of 1,711 (3.1%) patients were readmitted to ICU, main reasons being cardiac arrhythmias (24, 41%), pericardial effusion (9, 15.2%), and infection (8, 13.5%). Readmission was significantly higher for valvular interventions (39 patients, 24.3%, mitral valve 25 patients) than coronary artery bypass grafting (13, 10.6%), P value 0.003*. On multivariate analysis, EuroSCORE 2 (>5), age, surgical reexploration, postoperative pulmonary complications, and infections were independently associated with a need for ICU readmission. The mortality rate among the readmitted patients was 7.4% compared to 1.4% overall mortality. The mean total postoperative length of stay was significantly longer for recidival patients (17.6 ± 14 days vs 7.6 ± 2.4 days; P < 0.0001).
Conclusions: Recidivism is associated with longer hospital stay, suboptimal outcomes as well higher risk of mortality. Postoperative cardiac dysrhythmia was the most common cause of recidivism in our cohort. Early identification of patients at risk for recidivism and timely management of cardiopulmonary complications can translate to better outcomes.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
