Jonathan Kochav, Michael P DiLorenzo, Matthew J Lewis, Maarten Groenink, Malou van den Boogaard, Barbara Mulder, Marlon Rosenbaum
{"title":"通过心血管磁共振成像评估大血管转位成人患者全身右心室重塑的纵向变化。","authors":"Jonathan Kochav, Michael P DiLorenzo, Matthew J Lewis, Maarten Groenink, Malou van den Boogaard, Barbara Mulder, Marlon Rosenbaum","doi":"10.1016/j.jocmr.2024.101107","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Systemic right ventricular (sRV) physiology occurs in patients with congenitally corrected transposition of the great arteries (ccTGA) and D-TGA post atrial switch repair, and the natural history is of progressive sRV dysfunction. No study has assessed longitudinal changes in sRV remodeling by serial cardiovascular magnetic resonance (CMR).</p><p><strong>Methods: </strong>Patients evaluated at two adult congenital heart disease centers and who underwent ≥2 CMR exams were studied. Indexed sRV end-diastolic volume (sRVEDVi), end-systolic volume (sRVESVi), and ejection fraction (sRVEF) were determined by a core laboratory. Concurrent echocardiograms were assessed for degree of systemic tricuspid regurgitation (sTR). Tricuspid valve events were defined as ≥moderate sTR, or interval tricuspid valve replacement (TVR). Generally, the earliest and most recent studies were compared. A subset of patients were followed with ≥moderate sTR, and then subsequently underwent interval TVR. For these patients, two study time intervals were defined to analyze the impact of each event independently.</p><p><strong>Results: </strong>Sixty-seven patients were studied (33 ± 11 years, 48% [32/67] male, 33% [22/67] ccTGA), with 72 total time intervals studied (median interval 9.0 years [interquartile range 4.6-13.3]). There was a small increase in sRVEDVi over time (ΔsRVEDVi 5.5 ± 15.8 mL/m<sup>2</sup>, p < 0.001), but mean change in sRVEF was not significant (ΔsRVEF 0.1 ± 6.9%, p = 0.86); notably, confidence intervals (CI) were wide for both. ccTGA patients had a trend toward greater decrement in sRVEF (ΔsRVEF -1.7 ± 6.8 vs 1.3 ± 6.7%, p = 0.06). For each 25 mL/m<sup>2</sup> increase in baseline sRVEDVi, there was a 1.8% decrease in sRVEF (95% CI -3.2% to -0.5%, p = 0.01). Patients without significant sTR had lesser deterioration in sRVEF compared to those with ≥moderate sTR or with interval TR intervention (ΔsRVEF 1.8 ± 6.9% vs -2.1 ± 6.6% and -2.6 ± 4.5, p < 0.05). Interval sRV conduction delay was associated with a trend toward greater decrements in sRVEF (ΔsRVEF -3.9 ± 6.3 vs 0.9 ± 6.8%, p = 0.07). Overall, underlying congenital anatomy, baseline sRVEDVi, advanced sTR or interval TVR, and sRV conduction delay explained only 16% of the variability in ΔsRVEF over time.</p><p><strong>Conclusion: </strong>Longitudinal changes in sRV remodeling were small, with great heterogeneity. Apparent risk factors in our study, namely underlying congenital anatomy, baseline sRVEDVi, TR events, and sRV conduction disease accounted for only 16% of the variability seen in the longitudinal change of sRVEF.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101107"},"PeriodicalIF":6.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11652919/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal changes in systemic right ventricular remodeling in adult patients with transposition of the great vessels as assessed by cardiovascular magnetic resonance imaging.\",\"authors\":\"Jonathan Kochav, Michael P DiLorenzo, Matthew J Lewis, Maarten Groenink, Malou van den Boogaard, Barbara Mulder, Marlon Rosenbaum\",\"doi\":\"10.1016/j.jocmr.2024.101107\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Systemic right ventricular (sRV) physiology occurs in patients with congenitally corrected transposition of the great arteries (ccTGA) and D-TGA post atrial switch repair, and the natural history is of progressive sRV dysfunction. No study has assessed longitudinal changes in sRV remodeling by serial cardiovascular magnetic resonance (CMR).</p><p><strong>Methods: </strong>Patients evaluated at two adult congenital heart disease centers and who underwent ≥2 CMR exams were studied. Indexed sRV end-diastolic volume (sRVEDVi), end-systolic volume (sRVESVi), and ejection fraction (sRVEF) were determined by a core laboratory. Concurrent echocardiograms were assessed for degree of systemic tricuspid regurgitation (sTR). Tricuspid valve events were defined as ≥moderate sTR, or interval tricuspid valve replacement (TVR). Generally, the earliest and most recent studies were compared. A subset of patients were followed with ≥moderate sTR, and then subsequently underwent interval TVR. For these patients, two study time intervals were defined to analyze the impact of each event independently.</p><p><strong>Results: </strong>Sixty-seven patients were studied (33 ± 11 years, 48% [32/67] male, 33% [22/67] ccTGA), with 72 total time intervals studied (median interval 9.0 years [interquartile range 4.6-13.3]). There was a small increase in sRVEDVi over time (ΔsRVEDVi 5.5 ± 15.8 mL/m<sup>2</sup>, p < 0.001), but mean change in sRVEF was not significant (ΔsRVEF 0.1 ± 6.9%, p = 0.86); notably, confidence intervals (CI) were wide for both. ccTGA patients had a trend toward greater decrement in sRVEF (ΔsRVEF -1.7 ± 6.8 vs 1.3 ± 6.7%, p = 0.06). For each 25 mL/m<sup>2</sup> increase in baseline sRVEDVi, there was a 1.8% decrease in sRVEF (95% CI -3.2% to -0.5%, p = 0.01). Patients without significant sTR had lesser deterioration in sRVEF compared to those with ≥moderate sTR or with interval TR intervention (ΔsRVEF 1.8 ± 6.9% vs -2.1 ± 6.6% and -2.6 ± 4.5, p < 0.05). Interval sRV conduction delay was associated with a trend toward greater decrements in sRVEF (ΔsRVEF -3.9 ± 6.3 vs 0.9 ± 6.8%, p = 0.07). Overall, underlying congenital anatomy, baseline sRVEDVi, advanced sTR or interval TVR, and sRV conduction delay explained only 16% of the variability in ΔsRVEF over time.</p><p><strong>Conclusion: </strong>Longitudinal changes in sRV remodeling were small, with great heterogeneity. Apparent risk factors in our study, namely underlying congenital anatomy, baseline sRVEDVi, TR events, and sRV conduction disease accounted for only 16% of the variability seen in the longitudinal change of sRVEF.</p>\",\"PeriodicalId\":15221,\"journal\":{\"name\":\"Journal of Cardiovascular Magnetic Resonance\",\"volume\":\" \",\"pages\":\"101107\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11652919/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Magnetic Resonance\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jocmr.2024.101107\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2024.101107","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Longitudinal changes in systemic right ventricular remodeling in adult patients with transposition of the great vessels as assessed by cardiovascular magnetic resonance imaging.
Background: Systemic right ventricular (sRV) physiology occurs in patients with congenitally corrected transposition of the great arteries (ccTGA) and D-TGA post atrial switch repair, and the natural history is of progressive sRV dysfunction. No study has assessed longitudinal changes in sRV remodeling by serial cardiovascular magnetic resonance (CMR).
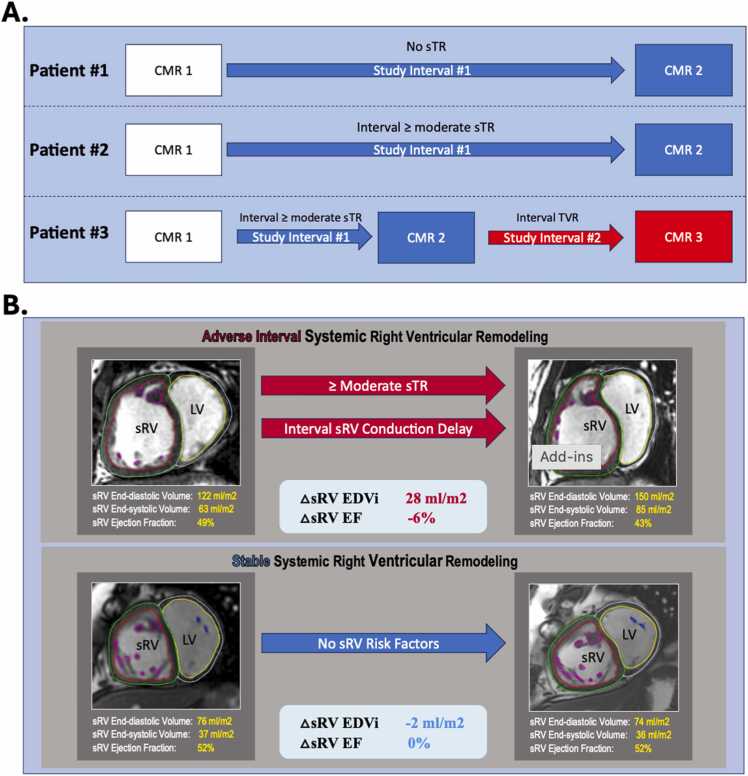
Methods: Patients evaluated at two adult congenital heart disease centers and who underwent ≥2 CMR exams were studied. Indexed sRV end-diastolic volume (sRVEDVi), end-systolic volume (sRVESVi), and ejection fraction (sRVEF) were determined by a core laboratory. Concurrent echocardiograms were assessed for degree of systemic tricuspid regurgitation (sTR). Tricuspid valve events were defined as ≥moderate sTR, or interval tricuspid valve replacement (TVR). Generally, the earliest and most recent studies were compared. A subset of patients were followed with ≥moderate sTR, and then subsequently underwent interval TVR. For these patients, two study time intervals were defined to analyze the impact of each event independently.
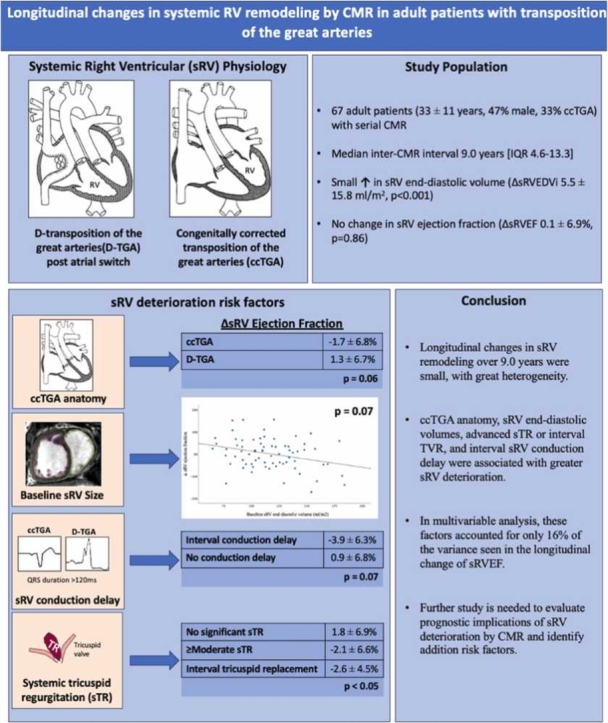
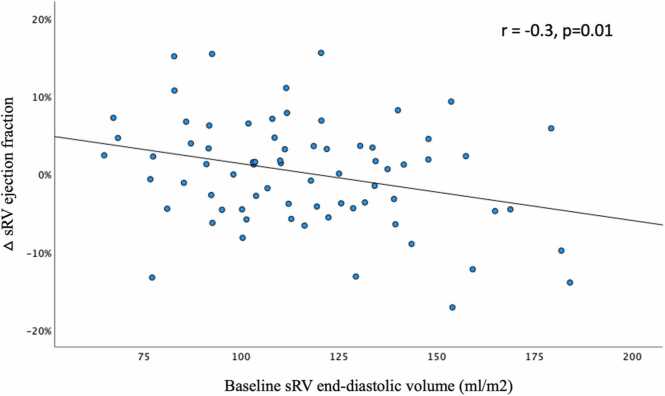
Results: Sixty-seven patients were studied (33 ± 11 years, 48% [32/67] male, 33% [22/67] ccTGA), with 72 total time intervals studied (median interval 9.0 years [interquartile range 4.6-13.3]). There was a small increase in sRVEDVi over time (ΔsRVEDVi 5.5 ± 15.8 mL/m2, p < 0.001), but mean change in sRVEF was not significant (ΔsRVEF 0.1 ± 6.9%, p = 0.86); notably, confidence intervals (CI) were wide for both. ccTGA patients had a trend toward greater decrement in sRVEF (ΔsRVEF -1.7 ± 6.8 vs 1.3 ± 6.7%, p = 0.06). For each 25 mL/m2 increase in baseline sRVEDVi, there was a 1.8% decrease in sRVEF (95% CI -3.2% to -0.5%, p = 0.01). Patients without significant sTR had lesser deterioration in sRVEF compared to those with ≥moderate sTR or with interval TR intervention (ΔsRVEF 1.8 ± 6.9% vs -2.1 ± 6.6% and -2.6 ± 4.5, p < 0.05). Interval sRV conduction delay was associated with a trend toward greater decrements in sRVEF (ΔsRVEF -3.9 ± 6.3 vs 0.9 ± 6.8%, p = 0.07). Overall, underlying congenital anatomy, baseline sRVEDVi, advanced sTR or interval TVR, and sRV conduction delay explained only 16% of the variability in ΔsRVEF over time.
Conclusion: Longitudinal changes in sRV remodeling were small, with great heterogeneity. Apparent risk factors in our study, namely underlying congenital anatomy, baseline sRVEDVi, TR events, and sRV conduction disease accounted for only 16% of the variability seen in the longitudinal change of sRVEF.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
