Caroline Dinesen, Simon Tilma Vistisen, Peter Juhl-Olsen
{"title":"传感器位置的微小变化会导致心输出量读数的系统性变化:对临床实践的影响。","authors":"Caroline Dinesen, Simon Tilma Vistisen, Peter Juhl-Olsen","doi":"10.1007/s10877-024-01230-6","DOIUrl":null,"url":null,"abstract":"<p><p>To systematically evaluate the effect of small changes in transducer position on key hemodynamic variables including CO generated by 4th generation FloTrac software. After cardiac surgery, cardiac output, mean arterial pressure, systemic vascular resistance, and stroke volume variation were measured with 4 generation Flotrac software. The transducer position was randomly placed at the midaxillary plane, 4 cm higher than the midaxillary plane or 4 cm lower than the midaxillary plane. Averages of three measurements were used. Data was available from 20 patients. Cardiac output increased from 4.59 L/min (± 0.92) to 4.78 L/min (± 0.99) with the transducer position at the midaxillary plane to 4 cm higher than the midaxillary plane, and cardiac output decreased to 4.43 L/min (± 0.90) with the transducer 4 cm lower than midaxillary plane (P < 0.001). On the relative scale, CO increased 4.1% (95% CI 3.1-5.0) when comparing the higher transducer level with the midaxillary plane position, and CO decreased 3.4% (95% CI 2.4-4.4) when comparing the midaxillary plane position with the lower transducer level, correspondiong to changes in CO of ≈ 1% per 1 cm change in transducer position. Mean arterial pressure and systemic vascular resistance both changed significantly with transducer position (both P < 0.001), whereas no statistically or clinically significant effect was seen on stroke volume variation (P = 0.98). A four-centimeter change in vertical transducer position induced clinically significant changes in cardiac output measurements by 4th generation FloTrac software. Definitions of optimal cardiac output in goal-directed therapy algorithms require meticulous transducer adjustment and can only be used in the reference patient position.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"365-369"},"PeriodicalIF":2.6000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049297/pdf/","citationCount":"0","resultStr":"{\"title\":\"Small changes in the transducer position cause a systematic change in cardiac output readings: implications for clinical practice.\",\"authors\":\"Caroline Dinesen, Simon Tilma Vistisen, Peter Juhl-Olsen\",\"doi\":\"10.1007/s10877-024-01230-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>To systematically evaluate the effect of small changes in transducer position on key hemodynamic variables including CO generated by 4th generation FloTrac software. After cardiac surgery, cardiac output, mean arterial pressure, systemic vascular resistance, and stroke volume variation were measured with 4 generation Flotrac software. The transducer position was randomly placed at the midaxillary plane, 4 cm higher than the midaxillary plane or 4 cm lower than the midaxillary plane. Averages of three measurements were used. Data was available from 20 patients. Cardiac output increased from 4.59 L/min (± 0.92) to 4.78 L/min (± 0.99) with the transducer position at the midaxillary plane to 4 cm higher than the midaxillary plane, and cardiac output decreased to 4.43 L/min (± 0.90) with the transducer 4 cm lower than midaxillary plane (P < 0.001). On the relative scale, CO increased 4.1% (95% CI 3.1-5.0) when comparing the higher transducer level with the midaxillary plane position, and CO decreased 3.4% (95% CI 2.4-4.4) when comparing the midaxillary plane position with the lower transducer level, correspondiong to changes in CO of ≈ 1% per 1 cm change in transducer position. Mean arterial pressure and systemic vascular resistance both changed significantly with transducer position (both P < 0.001), whereas no statistically or clinically significant effect was seen on stroke volume variation (P = 0.98). A four-centimeter change in vertical transducer position induced clinically significant changes in cardiac output measurements by 4th generation FloTrac software. Definitions of optimal cardiac output in goal-directed therapy algorithms require meticulous transducer adjustment and can only be used in the reference patient position.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"365-369\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049297/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-024-01230-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01230-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Small changes in the transducer position cause a systematic change in cardiac output readings: implications for clinical practice.
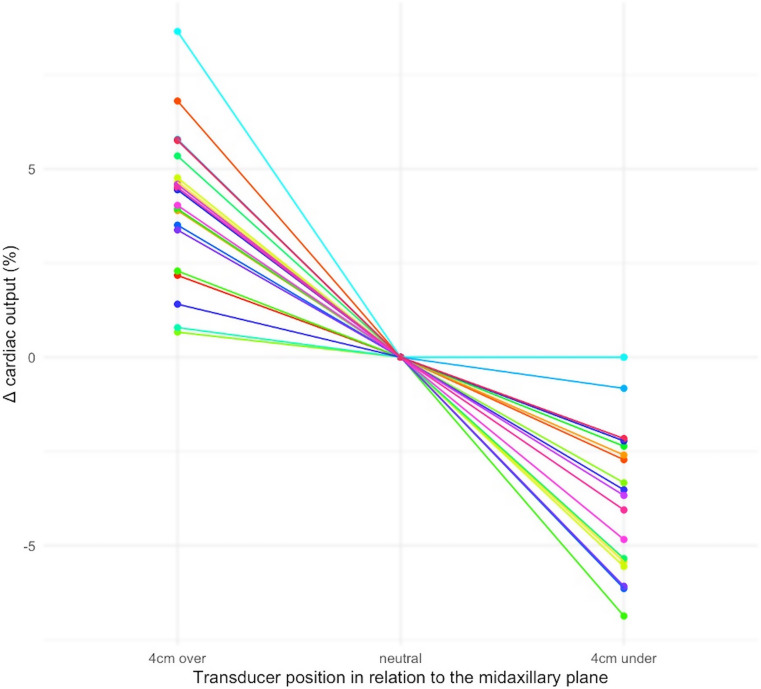
To systematically evaluate the effect of small changes in transducer position on key hemodynamic variables including CO generated by 4th generation FloTrac software. After cardiac surgery, cardiac output, mean arterial pressure, systemic vascular resistance, and stroke volume variation were measured with 4 generation Flotrac software. The transducer position was randomly placed at the midaxillary plane, 4 cm higher than the midaxillary plane or 4 cm lower than the midaxillary plane. Averages of three measurements were used. Data was available from 20 patients. Cardiac output increased from 4.59 L/min (± 0.92) to 4.78 L/min (± 0.99) with the transducer position at the midaxillary plane to 4 cm higher than the midaxillary plane, and cardiac output decreased to 4.43 L/min (± 0.90) with the transducer 4 cm lower than midaxillary plane (P < 0.001). On the relative scale, CO increased 4.1% (95% CI 3.1-5.0) when comparing the higher transducer level with the midaxillary plane position, and CO decreased 3.4% (95% CI 2.4-4.4) when comparing the midaxillary plane position with the lower transducer level, correspondiong to changes in CO of ≈ 1% per 1 cm change in transducer position. Mean arterial pressure and systemic vascular resistance both changed significantly with transducer position (both P < 0.001), whereas no statistically or clinically significant effect was seen on stroke volume variation (P = 0.98). A four-centimeter change in vertical transducer position induced clinically significant changes in cardiac output measurements by 4th generation FloTrac software. Definitions of optimal cardiac output in goal-directed therapy algorithms require meticulous transducer adjustment and can only be used in the reference patient position.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
