{"title":"利用持续性心房颤动患者消融前和消融后左心房容积指数对主要不良临床事件进行风险分层的新方法","authors":"Hironori Ishiguchi, Yasuhiro Yoshiga, Akihiko Shimizu, Masakazu Fukuda, Ayumi Omuro, Masahiro Hisaoka, Yusuke Nakashima, Miho Fujita, Shintaro Hashimoto, Takuya Omuro, Toru Ariyoshi, Shigeki Kobayashi, Takayuki Okamura, Motoaki Sano","doi":"10.1253/circrep.CR-24-0062","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The relationship between changes in the left atrial volume index (LAVI) post-catheter ablation (CA) and long-term prognostic events in patients with persistent atrial fibrillation (AF) remains unclear. We evaluated the incidence of major adverse clinical events (MACE), including all-cause death, unplanned heart failure hospitalization, and unplanned cardiovascular hospitalization using pre- and post-CA LAVI.</p><p><strong>Methods and results: </strong>We collected data retrospectively from 150 patients with persistent AF who underwent their first CA. LAVI was calculated during preprocedural echocardiography under AF rhythm (pre-CA LAVI) and 3 months post-CA under sinus rhythm (post-CA LAVI). The cumulative incidence of MACE was compared among 3 subgroups based on the cutoff values of pre-CA (45.5 mL/m<sup>2</sup>) and post-CA (46.5 mL/m<sup>2</sup>; both determined using the c-statistic) LAVI. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI >46.5 mL/m<sup>2</sup> (n=45) had a significantly higher MACE incidence compared with other subgroups (P=0.002). Multivariate analysis identified this subgroup as independently at higher risk for MACE. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI ≤46.5 mL/m<sup>2</sup> (n=49) had an incidence comparable with those with pre-CA LAVI ≤45.5 mL/m<sup>2</sup> (n=56) and exhibited a significantly greater reduction in LAVI than other subgroups did (P<0.001).</p><p><strong>Conclusions: </strong>Combining pre-CA and post-CA LAVIs is valuable in stratifying long-term MACE development risk following CA.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"6 10","pages":"415-423"},"PeriodicalIF":1.1000,"publicationDate":"2024-09-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11464015/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel Method for Risk Stratification of Major Adverse Clinical Events Using Pre- and Post-Ablation Left Atrial Volume Index in Patients With Persistent Atrial Fibrillation.\",\"authors\":\"Hironori Ishiguchi, Yasuhiro Yoshiga, Akihiko Shimizu, Masakazu Fukuda, Ayumi Omuro, Masahiro Hisaoka, Yusuke Nakashima, Miho Fujita, Shintaro Hashimoto, Takuya Omuro, Toru Ariyoshi, Shigeki Kobayashi, Takayuki Okamura, Motoaki Sano\",\"doi\":\"10.1253/circrep.CR-24-0062\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The relationship between changes in the left atrial volume index (LAVI) post-catheter ablation (CA) and long-term prognostic events in patients with persistent atrial fibrillation (AF) remains unclear. We evaluated the incidence of major adverse clinical events (MACE), including all-cause death, unplanned heart failure hospitalization, and unplanned cardiovascular hospitalization using pre- and post-CA LAVI.</p><p><strong>Methods and results: </strong>We collected data retrospectively from 150 patients with persistent AF who underwent their first CA. LAVI was calculated during preprocedural echocardiography under AF rhythm (pre-CA LAVI) and 3 months post-CA under sinus rhythm (post-CA LAVI). The cumulative incidence of MACE was compared among 3 subgroups based on the cutoff values of pre-CA (45.5 mL/m<sup>2</sup>) and post-CA (46.5 mL/m<sup>2</sup>; both determined using the c-statistic) LAVI. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI >46.5 mL/m<sup>2</sup> (n=45) had a significantly higher MACE incidence compared with other subgroups (P=0.002). Multivariate analysis identified this subgroup as independently at higher risk for MACE. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI ≤46.5 mL/m<sup>2</sup> (n=49) had an incidence comparable with those with pre-CA LAVI ≤45.5 mL/m<sup>2</sup> (n=56) and exhibited a significantly greater reduction in LAVI than other subgroups did (P<0.001).</p><p><strong>Conclusions: </strong>Combining pre-CA and post-CA LAVIs is valuable in stratifying long-term MACE development risk following CA.</p>\",\"PeriodicalId\":94305,\"journal\":{\"name\":\"Circulation reports\",\"volume\":\"6 10\",\"pages\":\"415-423\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-09-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11464015/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1253/circrep.CR-24-0062\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/10 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-24-0062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Novel Method for Risk Stratification of Major Adverse Clinical Events Using Pre- and Post-Ablation Left Atrial Volume Index in Patients With Persistent Atrial Fibrillation.
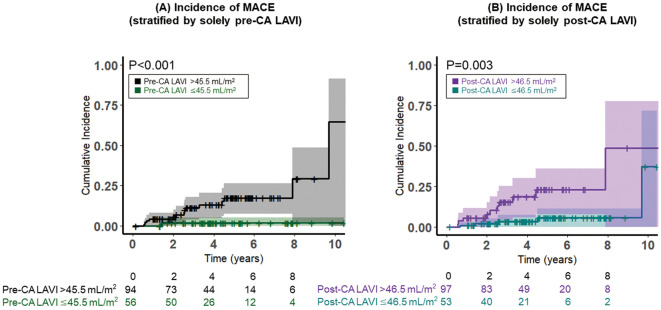
Background: The relationship between changes in the left atrial volume index (LAVI) post-catheter ablation (CA) and long-term prognostic events in patients with persistent atrial fibrillation (AF) remains unclear. We evaluated the incidence of major adverse clinical events (MACE), including all-cause death, unplanned heart failure hospitalization, and unplanned cardiovascular hospitalization using pre- and post-CA LAVI.
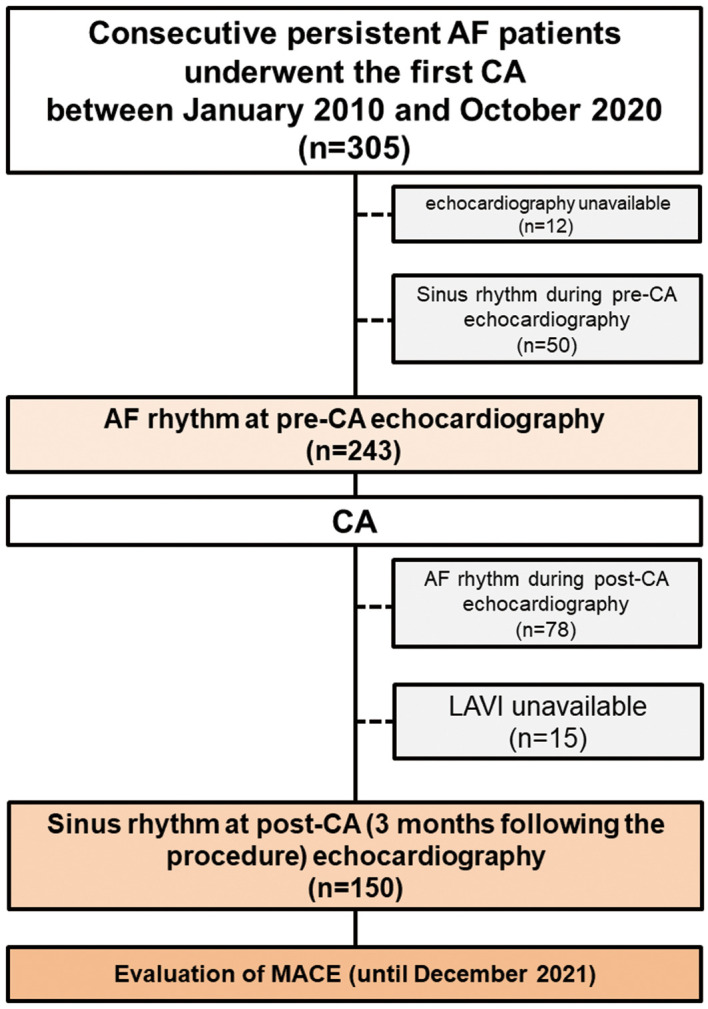
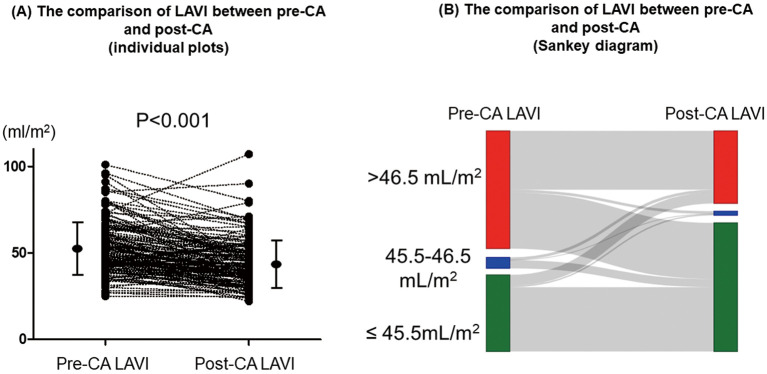
Methods and results: We collected data retrospectively from 150 patients with persistent AF who underwent their first CA. LAVI was calculated during preprocedural echocardiography under AF rhythm (pre-CA LAVI) and 3 months post-CA under sinus rhythm (post-CA LAVI). The cumulative incidence of MACE was compared among 3 subgroups based on the cutoff values of pre-CA (45.5 mL/m2) and post-CA (46.5 mL/m2; both determined using the c-statistic) LAVI. The subgroup of a pre-CA LAVI >45.5 mL/m2 with a post-CA LAVI >46.5 mL/m2 (n=45) had a significantly higher MACE incidence compared with other subgroups (P=0.002). Multivariate analysis identified this subgroup as independently at higher risk for MACE. The subgroup of a pre-CA LAVI >45.5 mL/m2 with a post-CA LAVI ≤46.5 mL/m2 (n=49) had an incidence comparable with those with pre-CA LAVI ≤45.5 mL/m2 (n=56) and exhibited a significantly greater reduction in LAVI than other subgroups did (P<0.001).
Conclusions: Combining pre-CA and post-CA LAVIs is valuable in stratifying long-term MACE development risk following CA.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
