{"title":"用于检测肾细胞癌术后晚期复发和随访损失的机器学习分析","authors":"Kodai Sato, Tomokazu Sazuka, Takayuki Arai, Hiroaki Sato, Manato Kanesaka, Keisuke Ando, Shinpei Saito, Sangjon Pae, Yasutaka Yamada, Yusuke Imamura, Shinichi Sakamoto, Tomohiko Ichikawa","doi":"10.1002/bco2.425","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>Renal cell carcinoma (RCC) is shown to have a tendency for late recurrence, occurring 5 or more years after curative surgery. Imaging diagnosis is required for follow-up, and there is no definitive answer as to how long this should continue. Some patients discontinue follow-up visits at their own discretion. How best to predict late recurrence and loss to follow-up (LF) remains unclear.</p>\n </section>\n \n <section>\n \n <h3> Patients and methods</h3>\n \n <p>This study targeted patients diagnosed with non-metastatic RCC who underwent either radical or partial nephrectomy at Chiba University Hospital between 1988 and 2021. Follow-up for patients with RCC is typically lifelong. We used random survival forests (RSFs), a machine learning-based survival analysis method, to predict late recurrence and LF. For verification of prediction accuracy, we applied the time-dependent area under the receiver operating characteristic curve (t-AUC). To analyse the risks of late recurrence and LF, SurvSHAP(t) and partial dependence plots were used.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We analysed 1051 cases in this study. Median follow-up was 58.5 (range: 0–376) months. The predictive accuracy of recurrence using RSF was t-AUC 0.806, 0.761, 0.674 and 0.566 at 60, 120, 180 and 240 months postoperatively, respectively. The recurrence risk impact showed a time-dependent increase up to approximately 50 months postoperatively. Beyond 50 months, there were no distinct risk factors characteristic of late recurrence. The predictive accuracy of LF using RSF was t-AUC 0.542, 0.699, 0.685, 0.628 and 0.674 at 60, 120, 180, 240 and 300 months postoperatively, respectively. The risk of LF increased with advancing age beyond 70 years.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>It is difficult to identify factors that predict late recurrence. For long-term follow-up observation, it is essential to pay particular attention to patients with RCC aged 70 years and above. Establishing frameworks to facilitate collaboration with local hospitals near patients' residences and providing care within the community is necessary.</p>\n </section>\n </div>","PeriodicalId":72420,"journal":{"name":"BJUI compass","volume":"5 10","pages":"1064-1070"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.425","citationCount":"0","resultStr":"{\"title\":\"Machine learning analysis for detecting late recurrence and loss to follow-up after renal cell carcinoma surgery\",\"authors\":\"Kodai Sato, Tomokazu Sazuka, Takayuki Arai, Hiroaki Sato, Manato Kanesaka, Keisuke Ando, Shinpei Saito, Sangjon Pae, Yasutaka Yamada, Yusuke Imamura, Shinichi Sakamoto, Tomohiko Ichikawa\",\"doi\":\"10.1002/bco2.425\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>Renal cell carcinoma (RCC) is shown to have a tendency for late recurrence, occurring 5 or more years after curative surgery. Imaging diagnosis is required for follow-up, and there is no definitive answer as to how long this should continue. Some patients discontinue follow-up visits at their own discretion. How best to predict late recurrence and loss to follow-up (LF) remains unclear.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patients and methods</h3>\\n \\n <p>This study targeted patients diagnosed with non-metastatic RCC who underwent either radical or partial nephrectomy at Chiba University Hospital between 1988 and 2021. Follow-up for patients with RCC is typically lifelong. We used random survival forests (RSFs), a machine learning-based survival analysis method, to predict late recurrence and LF. For verification of prediction accuracy, we applied the time-dependent area under the receiver operating characteristic curve (t-AUC). To analyse the risks of late recurrence and LF, SurvSHAP(t) and partial dependence plots were used.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We analysed 1051 cases in this study. Median follow-up was 58.5 (range: 0–376) months. The predictive accuracy of recurrence using RSF was t-AUC 0.806, 0.761, 0.674 and 0.566 at 60, 120, 180 and 240 months postoperatively, respectively. The recurrence risk impact showed a time-dependent increase up to approximately 50 months postoperatively. Beyond 50 months, there were no distinct risk factors characteristic of late recurrence. The predictive accuracy of LF using RSF was t-AUC 0.542, 0.699, 0.685, 0.628 and 0.674 at 60, 120, 180, 240 and 300 months postoperatively, respectively. The risk of LF increased with advancing age beyond 70 years.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>It is difficult to identify factors that predict late recurrence. For long-term follow-up observation, it is essential to pay particular attention to patients with RCC aged 70 years and above. Establishing frameworks to facilitate collaboration with local hospitals near patients' residences and providing care within the community is necessary.</p>\\n </section>\\n </div>\",\"PeriodicalId\":72420,\"journal\":{\"name\":\"BJUI compass\",\"volume\":\"5 10\",\"pages\":\"1064-1070\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.425\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJUI compass\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://bjui-journals.onlinelibrary.wiley.com/doi/10.1002/bco2.425\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJUI compass","FirstCategoryId":"1085","ListUrlMain":"https://bjui-journals.onlinelibrary.wiley.com/doi/10.1002/bco2.425","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Machine learning analysis for detecting late recurrence and loss to follow-up after renal cell carcinoma surgery
Objectives
Renal cell carcinoma (RCC) is shown to have a tendency for late recurrence, occurring 5 or more years after curative surgery. Imaging diagnosis is required for follow-up, and there is no definitive answer as to how long this should continue. Some patients discontinue follow-up visits at their own discretion. How best to predict late recurrence and loss to follow-up (LF) remains unclear.
Patients and methods
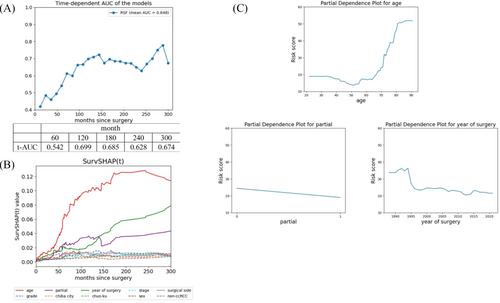
This study targeted patients diagnosed with non-metastatic RCC who underwent either radical or partial nephrectomy at Chiba University Hospital between 1988 and 2021. Follow-up for patients with RCC is typically lifelong. We used random survival forests (RSFs), a machine learning-based survival analysis method, to predict late recurrence and LF. For verification of prediction accuracy, we applied the time-dependent area under the receiver operating characteristic curve (t-AUC). To analyse the risks of late recurrence and LF, SurvSHAP(t) and partial dependence plots were used.
Results
We analysed 1051 cases in this study. Median follow-up was 58.5 (range: 0–376) months. The predictive accuracy of recurrence using RSF was t-AUC 0.806, 0.761, 0.674 and 0.566 at 60, 120, 180 and 240 months postoperatively, respectively. The recurrence risk impact showed a time-dependent increase up to approximately 50 months postoperatively. Beyond 50 months, there were no distinct risk factors characteristic of late recurrence. The predictive accuracy of LF using RSF was t-AUC 0.542, 0.699, 0.685, 0.628 and 0.674 at 60, 120, 180, 240 and 300 months postoperatively, respectively. The risk of LF increased with advancing age beyond 70 years.
Conclusion
It is difficult to identify factors that predict late recurrence. For long-term follow-up observation, it is essential to pay particular attention to patients with RCC aged 70 years and above. Establishing frameworks to facilitate collaboration with local hospitals near patients' residences and providing care within the community is necessary.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
