Madhava Pai Kanhangad, Vidyadhara Srinivasa, Balamurugan Thirugnanam, Abhishek Soni, Anjana Kashyap, Alia Vidyadhara, Sharath Kumar Rao
{"title":"机器人脊柱系统:克服外科医生经验对椎弓根螺钉准确性的影响:一项前瞻性研究。","authors":"Madhava Pai Kanhangad, Vidyadhara Srinivasa, Balamurugan Thirugnanam, Abhishek Soni, Anjana Kashyap, Alia Vidyadhara, Sharath Kumar Rao","doi":"10.31616/asj.2024.0191","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Prospective single-center study.</p><p><strong>Purpose: </strong>To compare the accuracy of pedicle screws placed by freehand and under fluoroscopy and robotic assistance with intraoperative image acquisition.</p><p><strong>Overview of literature: </strong>Pedicle screws are the most commonly used spinal anchors owing to their ability to stabilize all three spinal columns. Various techniques such as freehand, fluoroscopy-assisted, and navigation-assisted pedicle screw placements have been used with varying degrees of accuracy. Most studies on robotic-assisted pedicle screw placement have utilized preoperatively acquired computed tomography scans. To our knowledge, this is the only study in the literature that compared freehand with fluoroscopy-guided and robotic-assisted pedicle screw insertion with freehand and fluoroscopy.</p><p><strong>Methods: </strong>In this prospective study, a total of 1,120 pedicle screws were placed in the freehand group (n=175), 1,250 in the fluoroscopyassisted group (n=172), and 1,225 in the robotic-assisted group (n=180). Surgical parameters and screw accuracy were analyzed between the three groups. The preoperative plan overlapped with the postoperative O-arm scan to determine if the screws were executed as planned.</p><p><strong>Results: </strong>The frequency of clinically acceptable screw placement (Gertzbein-Robbins grades A and B) in the freehand, fluoroscopy-assisted, and robotic-assisted groups were 97.7%, 98.6%, and 99.34%, respectively. With robotic assistance, an experience-neutralizing effect implied that surgeons with varying levels of experience achieved comparable pedicle screw accuracy, blood loss, O-arm time, robot time, and time per screw. No significant difference in these parameters was found between surgeries commencing before and after 2 PM. No significant differences were noted between the planned and executed screw trajectories in the robotic-assisted group irrespective of surgical experience.</p><p><strong>Conclusions: </strong>The third-generation robotic-assisted pedicle screw placement system used in conjunction with intraoperative threedimensional O-arm imaging consistently demonstrates safe and accurate screw placement with an experience-neutralizing effect.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"663-672"},"PeriodicalIF":2.7000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11538820/pdf/","citationCount":"0","resultStr":"{\"title\":\"Robotic spine systems: overcoming surgeon experience in pedicle screw accuracy: a prospective study.\",\"authors\":\"Madhava Pai Kanhangad, Vidyadhara Srinivasa, Balamurugan Thirugnanam, Abhishek Soni, Anjana Kashyap, Alia Vidyadhara, Sharath Kumar Rao\",\"doi\":\"10.31616/asj.2024.0191\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study design: </strong>Prospective single-center study.</p><p><strong>Purpose: </strong>To compare the accuracy of pedicle screws placed by freehand and under fluoroscopy and robotic assistance with intraoperative image acquisition.</p><p><strong>Overview of literature: </strong>Pedicle screws are the most commonly used spinal anchors owing to their ability to stabilize all three spinal columns. Various techniques such as freehand, fluoroscopy-assisted, and navigation-assisted pedicle screw placements have been used with varying degrees of accuracy. Most studies on robotic-assisted pedicle screw placement have utilized preoperatively acquired computed tomography scans. To our knowledge, this is the only study in the literature that compared freehand with fluoroscopy-guided and robotic-assisted pedicle screw insertion with freehand and fluoroscopy.</p><p><strong>Methods: </strong>In this prospective study, a total of 1,120 pedicle screws were placed in the freehand group (n=175), 1,250 in the fluoroscopyassisted group (n=172), and 1,225 in the robotic-assisted group (n=180). Surgical parameters and screw accuracy were analyzed between the three groups. The preoperative plan overlapped with the postoperative O-arm scan to determine if the screws were executed as planned.</p><p><strong>Results: </strong>The frequency of clinically acceptable screw placement (Gertzbein-Robbins grades A and B) in the freehand, fluoroscopy-assisted, and robotic-assisted groups were 97.7%, 98.6%, and 99.34%, respectively. With robotic assistance, an experience-neutralizing effect implied that surgeons with varying levels of experience achieved comparable pedicle screw accuracy, blood loss, O-arm time, robot time, and time per screw. No significant difference in these parameters was found between surgeries commencing before and after 2 PM. No significant differences were noted between the planned and executed screw trajectories in the robotic-assisted group irrespective of surgical experience.</p><p><strong>Conclusions: </strong>The third-generation robotic-assisted pedicle screw placement system used in conjunction with intraoperative threedimensional O-arm imaging consistently demonstrates safe and accurate screw placement with an experience-neutralizing effect.</p>\",\"PeriodicalId\":8555,\"journal\":{\"name\":\"Asian Spine Journal\",\"volume\":\" \",\"pages\":\"663-672\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11538820/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asian Spine Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31616/asj.2024.0191\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0191","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Robotic spine systems: overcoming surgeon experience in pedicle screw accuracy: a prospective study.
Study design: Prospective single-center study.
Purpose: To compare the accuracy of pedicle screws placed by freehand and under fluoroscopy and robotic assistance with intraoperative image acquisition.
Overview of literature: Pedicle screws are the most commonly used spinal anchors owing to their ability to stabilize all three spinal columns. Various techniques such as freehand, fluoroscopy-assisted, and navigation-assisted pedicle screw placements have been used with varying degrees of accuracy. Most studies on robotic-assisted pedicle screw placement have utilized preoperatively acquired computed tomography scans. To our knowledge, this is the only study in the literature that compared freehand with fluoroscopy-guided and robotic-assisted pedicle screw insertion with freehand and fluoroscopy.
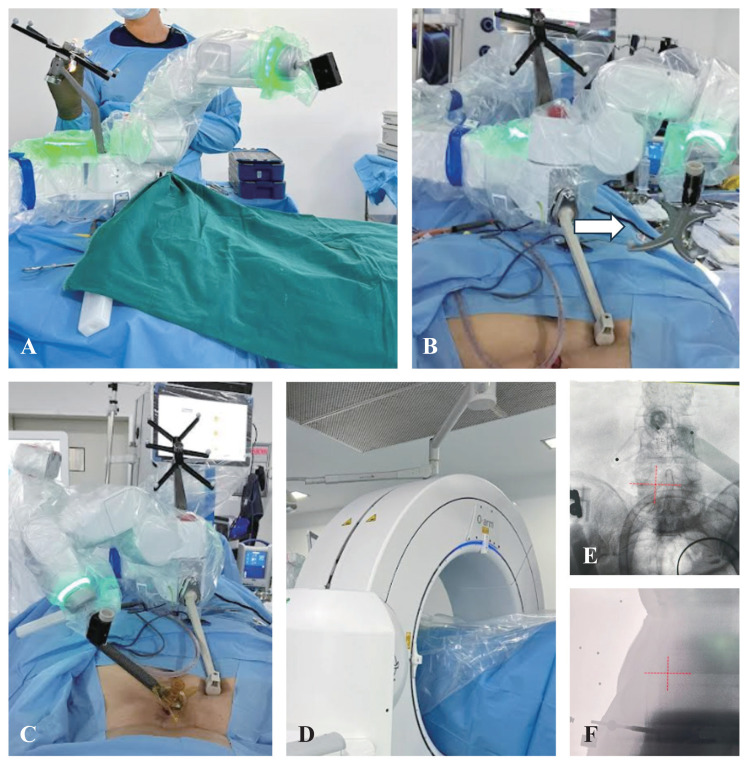
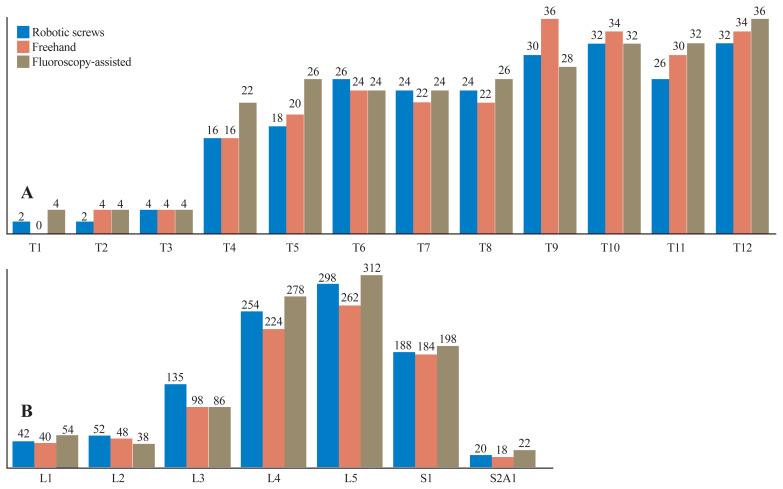
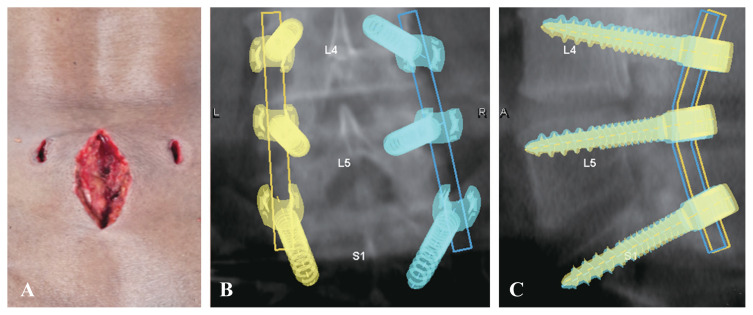
Methods: In this prospective study, a total of 1,120 pedicle screws were placed in the freehand group (n=175), 1,250 in the fluoroscopyassisted group (n=172), and 1,225 in the robotic-assisted group (n=180). Surgical parameters and screw accuracy were analyzed between the three groups. The preoperative plan overlapped with the postoperative O-arm scan to determine if the screws were executed as planned.
Results: The frequency of clinically acceptable screw placement (Gertzbein-Robbins grades A and B) in the freehand, fluoroscopy-assisted, and robotic-assisted groups were 97.7%, 98.6%, and 99.34%, respectively. With robotic assistance, an experience-neutralizing effect implied that surgeons with varying levels of experience achieved comparable pedicle screw accuracy, blood loss, O-arm time, robot time, and time per screw. No significant difference in these parameters was found between surgeries commencing before and after 2 PM. No significant differences were noted between the planned and executed screw trajectories in the robotic-assisted group irrespective of surgical experience.
Conclusions: The third-generation robotic-assisted pedicle screw placement system used in conjunction with intraoperative threedimensional O-arm imaging consistently demonstrates safe and accurate screw placement with an experience-neutralizing effect.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
