{"title":"转移性非透明细胞肾癌的护理模式和治疗效果:印度单一中心的经验。","authors":"Somnath Roy, Sreejata Raychaudhuri, Bivas Biswas, Deepak Dabkara, Arnab Bhattacherjee, Sandip Ganguly, Joydeep Ghosh, Yesha Sandipbhai Patel, Souhita Pal, Jagriti Karmakar, Anindita Mitra, Sujoy Gupta","doi":"10.3332/ecancer.2024.1775","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-clear-cell renal cell carcinoma (nccRCC) refers to a rare diverse heterogeneous group of tumours; usually treated with immune check point inhibitors and or tyrosine kinase inhibitors (TKIs). Prospective large-scale data from Asian countries is limited.</p><p><strong>Methods: </strong>This is a retrospective study of patients with metastatic nccRCC treated at Tata Medical Centre, Kolkata, India, from 2012 to 2022. Demographic profiles, histologic subtypes, treatment details, response to therapy (by response evaluation criteria in solid tumours (RECIST v1.1)) and survival status were captured from electronic medical records (EMRs) of hospitals up till May 2023. Kaplan Meier methods were estimated to assess progression-free survival (PFS) and overall survival (OS).</p><p><strong>Results: </strong>A total of 89 consecutive patients were screened for this study, 24 were excluded due to inadequate data in EMR. 65 patients were included in the final analysis, with a median age at diagnosis of 59 years (range 20-84) of which 81% were male. Histologic subtypes comprised of 43% papillary, 31% clear cell with mixed histology, 3% sarcomatoid and 23% others including chromophobe, mucinous-tubular, spindle cell, oncocytic, medullary, poorly differentiated and rhabdoid). The most common site of metastasis was the lung 62% (<i>n</i> = 40) followed by non-regional nodes 32%, bone 26% and liver 14%. 15% patients presented with haematuria and 62% underwent nephrectomy prior to systemic therapy. The majority received pazopanib 46% (<i>n</i> = 30), chemotherapy 20% (<i>n</i> = 13) including bevacizumab plus erlotinib, sunitinib 15% (<i>n</i> = 10) or cabozantinib 14% (<i>n</i> = 9). Only 3(5%) patients received nivolumab plus cabozantinib combination. Response to treatment showed complete response in 1.5%, partial response in 20%, stable disease in 51% and progressive disease in 23% as per RECIST v1.1. 17 patients required dose reduction and interruption due to adverse effects and 33% (<i>n</i> = 22) received second-line therapy with nivolumab 18% (<i>n</i> = 4), axitinib and everolimus among others. After a median follow up of 44 months, the median PFS was 13 months (95%CI 7.2-18.9) and the median OS was 17 months (95%CI 12.1-22.1) for the entire cohort.</p><p><strong>Conclusion: </strong>The overall response and survival for metastatic nccRCC was relatively better in comparison with published data, despite the limited number of patients treated with ICIs due to cost and access barriers.</p>","PeriodicalId":11460,"journal":{"name":"ecancermedicalscience","volume":"18 ","pages":"1775"},"PeriodicalIF":1.3000,"publicationDate":"2024-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489090/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pattern of care and treatment outcomes of metastatic non-clear cell kidney cancer: a single centre experience from India.\",\"authors\":\"Somnath Roy, Sreejata Raychaudhuri, Bivas Biswas, Deepak Dabkara, Arnab Bhattacherjee, Sandip Ganguly, Joydeep Ghosh, Yesha Sandipbhai Patel, Souhita Pal, Jagriti Karmakar, Anindita Mitra, Sujoy Gupta\",\"doi\":\"10.3332/ecancer.2024.1775\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Non-clear-cell renal cell carcinoma (nccRCC) refers to a rare diverse heterogeneous group of tumours; usually treated with immune check point inhibitors and or tyrosine kinase inhibitors (TKIs). Prospective large-scale data from Asian countries is limited.</p><p><strong>Methods: </strong>This is a retrospective study of patients with metastatic nccRCC treated at Tata Medical Centre, Kolkata, India, from 2012 to 2022. Demographic profiles, histologic subtypes, treatment details, response to therapy (by response evaluation criteria in solid tumours (RECIST v1.1)) and survival status were captured from electronic medical records (EMRs) of hospitals up till May 2023. Kaplan Meier methods were estimated to assess progression-free survival (PFS) and overall survival (OS).</p><p><strong>Results: </strong>A total of 89 consecutive patients were screened for this study, 24 were excluded due to inadequate data in EMR. 65 patients were included in the final analysis, with a median age at diagnosis of 59 years (range 20-84) of which 81% were male. Histologic subtypes comprised of 43% papillary, 31% clear cell with mixed histology, 3% sarcomatoid and 23% others including chromophobe, mucinous-tubular, spindle cell, oncocytic, medullary, poorly differentiated and rhabdoid). The most common site of metastasis was the lung 62% (<i>n</i> = 40) followed by non-regional nodes 32%, bone 26% and liver 14%. 15% patients presented with haematuria and 62% underwent nephrectomy prior to systemic therapy. The majority received pazopanib 46% (<i>n</i> = 30), chemotherapy 20% (<i>n</i> = 13) including bevacizumab plus erlotinib, sunitinib 15% (<i>n</i> = 10) or cabozantinib 14% (<i>n</i> = 9). Only 3(5%) patients received nivolumab plus cabozantinib combination. Response to treatment showed complete response in 1.5%, partial response in 20%, stable disease in 51% and progressive disease in 23% as per RECIST v1.1. 17 patients required dose reduction and interruption due to adverse effects and 33% (<i>n</i> = 22) received second-line therapy with nivolumab 18% (<i>n</i> = 4), axitinib and everolimus among others. After a median follow up of 44 months, the median PFS was 13 months (95%CI 7.2-18.9) and the median OS was 17 months (95%CI 12.1-22.1) for the entire cohort.</p><p><strong>Conclusion: </strong>The overall response and survival for metastatic nccRCC was relatively better in comparison with published data, despite the limited number of patients treated with ICIs due to cost and access barriers.</p>\",\"PeriodicalId\":11460,\"journal\":{\"name\":\"ecancermedicalscience\",\"volume\":\"18 \",\"pages\":\"1775\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489090/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ecancermedicalscience\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3332/ecancer.2024.1775\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ecancermedicalscience","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3332/ecancer.2024.1775","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Pattern of care and treatment outcomes of metastatic non-clear cell kidney cancer: a single centre experience from India.
Background: Non-clear-cell renal cell carcinoma (nccRCC) refers to a rare diverse heterogeneous group of tumours; usually treated with immune check point inhibitors and or tyrosine kinase inhibitors (TKIs). Prospective large-scale data from Asian countries is limited.
Methods: This is a retrospective study of patients with metastatic nccRCC treated at Tata Medical Centre, Kolkata, India, from 2012 to 2022. Demographic profiles, histologic subtypes, treatment details, response to therapy (by response evaluation criteria in solid tumours (RECIST v1.1)) and survival status were captured from electronic medical records (EMRs) of hospitals up till May 2023. Kaplan Meier methods were estimated to assess progression-free survival (PFS) and overall survival (OS).
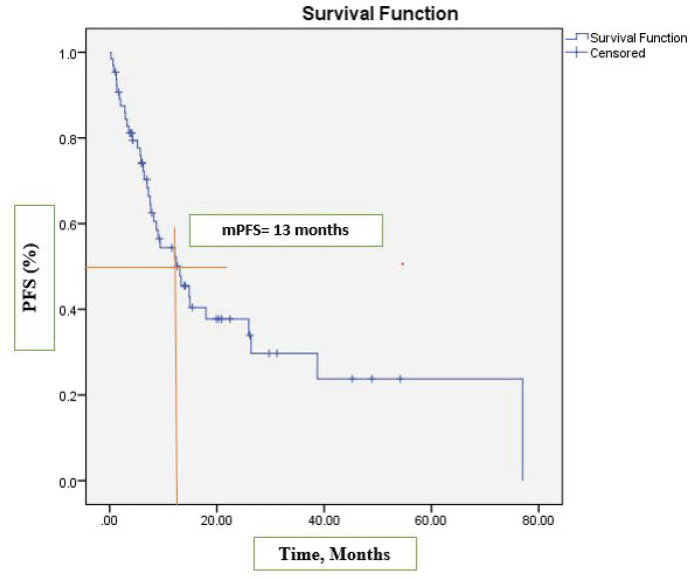
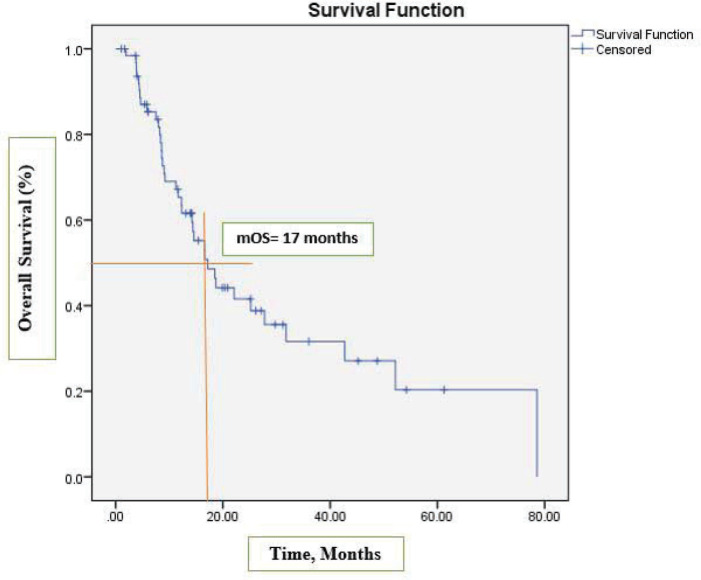
Results: A total of 89 consecutive patients were screened for this study, 24 were excluded due to inadequate data in EMR. 65 patients were included in the final analysis, with a median age at diagnosis of 59 years (range 20-84) of which 81% were male. Histologic subtypes comprised of 43% papillary, 31% clear cell with mixed histology, 3% sarcomatoid and 23% others including chromophobe, mucinous-tubular, spindle cell, oncocytic, medullary, poorly differentiated and rhabdoid). The most common site of metastasis was the lung 62% (n = 40) followed by non-regional nodes 32%, bone 26% and liver 14%. 15% patients presented with haematuria and 62% underwent nephrectomy prior to systemic therapy. The majority received pazopanib 46% (n = 30), chemotherapy 20% (n = 13) including bevacizumab plus erlotinib, sunitinib 15% (n = 10) or cabozantinib 14% (n = 9). Only 3(5%) patients received nivolumab plus cabozantinib combination. Response to treatment showed complete response in 1.5%, partial response in 20%, stable disease in 51% and progressive disease in 23% as per RECIST v1.1. 17 patients required dose reduction and interruption due to adverse effects and 33% (n = 22) received second-line therapy with nivolumab 18% (n = 4), axitinib and everolimus among others. After a median follow up of 44 months, the median PFS was 13 months (95%CI 7.2-18.9) and the median OS was 17 months (95%CI 12.1-22.1) for the entire cohort.
Conclusion: The overall response and survival for metastatic nccRCC was relatively better in comparison with published data, despite the limited number of patients treated with ICIs due to cost and access barriers.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
