Harendra Ipalawatte, Ariel Ahl, Jasprit Takher, Arian Gower
{"title":"心包积液导致吞咽困难的奇特表现","authors":"Harendra Ipalawatte, Ariel Ahl, Jasprit Takher, Arian Gower","doi":"10.1177/23247096241286364","DOIUrl":null,"url":null,"abstract":"<p><p>Esophageal dysphagia is most commonly caused by motility disorders and intrinsic mechanical obstruction. However, extrinsic obstruction, such as pericardial effusion, is rare causes of dysphagia. We present an 89-year-old male with history of Waldenstrom macroglobulinemia, Charcot-Marie-Tooth syndrome, and basal cell carcinoma presenting with generalized weakness, productive cough, shortness of breath, and dysphagia to both solids and liquids. A chest X-ray obtained showed cardiomegaly with suggested central vascular congestion and pulmonary edema. Further imaging with computed tomography (CT) abdomen and pelvis showed a moderate-to-large pericardial effusion. Patient later developed signs and symptoms of cardiac tamponade, requiring urgent pericardiocentesis with removal of 1 L of sanguineous fluid. Up to today, only 6 cases of dysphagia due to pericardial effusion have been described. This case displays another rare case and highlights the importance of recognizing dysphagia as a critical symptom as well as non-gastrointestinal (GI) causes of dysphagia.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"12 ","pages":"23247096241286364"},"PeriodicalIF":0.8000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11483682/pdf/","citationCount":"0","resultStr":"{\"title\":\"An Odd Presentation of Dysphagia Due to Pericardial Effusion.\",\"authors\":\"Harendra Ipalawatte, Ariel Ahl, Jasprit Takher, Arian Gower\",\"doi\":\"10.1177/23247096241286364\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Esophageal dysphagia is most commonly caused by motility disorders and intrinsic mechanical obstruction. However, extrinsic obstruction, such as pericardial effusion, is rare causes of dysphagia. We present an 89-year-old male with history of Waldenstrom macroglobulinemia, Charcot-Marie-Tooth syndrome, and basal cell carcinoma presenting with generalized weakness, productive cough, shortness of breath, and dysphagia to both solids and liquids. A chest X-ray obtained showed cardiomegaly with suggested central vascular congestion and pulmonary edema. Further imaging with computed tomography (CT) abdomen and pelvis showed a moderate-to-large pericardial effusion. Patient later developed signs and symptoms of cardiac tamponade, requiring urgent pericardiocentesis with removal of 1 L of sanguineous fluid. Up to today, only 6 cases of dysphagia due to pericardial effusion have been described. This case displays another rare case and highlights the importance of recognizing dysphagia as a critical symptom as well as non-gastrointestinal (GI) causes of dysphagia.</p>\",\"PeriodicalId\":16198,\"journal\":{\"name\":\"Journal of investigative medicine high impact case reports\",\"volume\":\"12 \",\"pages\":\"23247096241286364\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11483682/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of investigative medicine high impact case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23247096241286364\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096241286364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
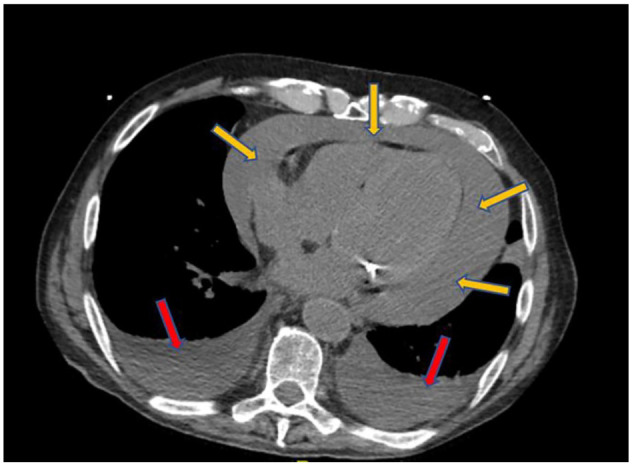
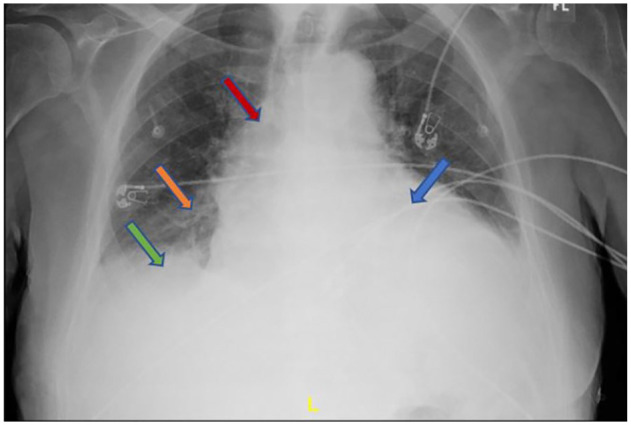
食道吞咽困难最常见的原因是运动障碍和内在机械性梗阻。然而,心包积液等外源性梗阻是导致吞咽困难的罕见原因。我们为大家介绍一位 89 岁的男性患者,他曾患瓦尔登斯特罗姆巨球蛋白血症、夏科-玛丽-托特综合征和基底细胞癌,表现为全身乏力、有痰咳嗽、呼吸急促以及固体和液体吞咽困难。胸部 X 光检查显示心脏肿大,并伴有中央血管充血和肺水肿。腹部和骨盆的进一步计算机断层扫描(CT)显示有中度到大型心包积液。患者后来出现了心脏填塞的症状和体征,需要紧急进行心包穿刺,取出 1 升淤血液。迄今为止,仅有 6 例因心包积液导致吞咽困难的病例。本病例是另一个罕见病例,它强调了认识吞咽困难这一重要症状以及非胃肠道(GI)原因导致吞咽困难的重要性。
An Odd Presentation of Dysphagia Due to Pericardial Effusion.
Esophageal dysphagia is most commonly caused by motility disorders and intrinsic mechanical obstruction. However, extrinsic obstruction, such as pericardial effusion, is rare causes of dysphagia. We present an 89-year-old male with history of Waldenstrom macroglobulinemia, Charcot-Marie-Tooth syndrome, and basal cell carcinoma presenting with generalized weakness, productive cough, shortness of breath, and dysphagia to both solids and liquids. A chest X-ray obtained showed cardiomegaly with suggested central vascular congestion and pulmonary edema. Further imaging with computed tomography (CT) abdomen and pelvis showed a moderate-to-large pericardial effusion. Patient later developed signs and symptoms of cardiac tamponade, requiring urgent pericardiocentesis with removal of 1 L of sanguineous fluid. Up to today, only 6 cases of dysphagia due to pericardial effusion have been described. This case displays another rare case and highlights the importance of recognizing dysphagia as a critical symptom as well as non-gastrointestinal (GI) causes of dysphagia.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
